Practice Essentials
Blount disease is a developmental disorder characterized by disordered growth of the medial aspect of the proximal tibial physis resulting in progressive lower-limb deformity. [1, 2, 3] Although it is also referred to as tibia vara (because the varus coronal plane deformity is most distinctive), the disease usually results in a multiplanar limb deformity consisting of varus, procurvatum, and internal rotation of the tibia. This pattern is a result of the asymmetry of disordered physeal growth, most pronounced in the posteromedial aspect of the proximal tibial physis. Blount disease can also be associated with a limb-length discrepancy and, in some patients, deformity of the distal femur as well. [4, 5]
Erlacher was the first to describe a case of tibia vara in 1922. Walter Blount brought attention to the disease in 1937 in an article describing 13 children with tibia vara or osteochondrosis deformans. Because he was the first to identify the similar clinical, radiographic, and pathologic characteristics of the cases in the literature, the disease has become associated with Blount. Later, in 1952, Langenskiöld described a progression of radiographic changes seen with the disease in the Scandinavian population. [6] (See the image below.)
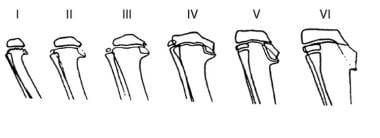 Diagram depicting radiographic changes in infantile form of Blount disease described by Langenskiöld.
Diagram depicting radiographic changes in infantile form of Blount disease described by Langenskiöld.
The natural history of Blount disease leads to irreversible pathologic changes, especially at the medial portion of the proximal tibial epiphysis because of growth disturbances of the physis. The progression and characteristics of the disease are distinct in the two described forms of the disease. (See the image below.)
 14-year-old boy with unilateral Blount disease demonstrating tibia vara on left. Courtesy of S Robert Rozbruch, MD.
14-year-old boy with unilateral Blount disease demonstrating tibia vara on left. Courtesy of S Robert Rozbruch, MD.
Classically, Blount disease has been described as occurring in two distinct forms: early-onset (or infantile) disease and late-onset (or adolescent) disease. Early-onset Blount disease is diagnosed at age 1-3 years, presenting when a child begins to ambulate; it is less commonly associated with obesity and is often bilateral. Late-onset Blount disease has been further subcategorized into juvenile, occurring at age 4-10 years, and adolescent, occurring at older than 10 years. Blount disease occurring in older children is more commonly seen in association with obesity and is more often unilateral. [7, 8]
Conservative treatment can be an option in early-onset Blount disease and consists of brace treatment. In late-onset patients and early-onset patients in whom brace management fails, operative intervention is indicated for increasing severity of symptoms or progression of deformity. [3]
Anatomy
The relevant anatomy for this disease is that of the proximal tibia and its surrounding structures. Structures at risk in this area on the medial side include the saphenous nerve and its branches. On the lateral side, the peroneal nerve courses around the neck of the fibula before dividing into deep and superficial branches.
During the performance of osteotomies or with pin insertion, these nerves, as well as the anterior tibial artery and its recurrent branch, are at risk. With acute correction of the varus deformity, medial-side structures are at risk for stretch injury. Compartment syndrome is a risk, particularly with acute correction of tibial deformity.
Pathophysiology
Blount disease most likely is caused by a combination of excessive compressive forces on the proximal medial metaphysis of the tibia and altered enchondral bone formation. [7] It is unclear whether the deformity is caused by an intrinsic alteration of bone formation that is exacerbated by compressive forces or by compressive forces that cause a disruption in normal endochondral bone formation.
The combination of mechanical and biologic factors in tibia vara most likely influences the disease to varying extents. The mechanical forces contributing to the disease are the weight of the child, age at walking, and the varus deformity. In accordance with the Heuter-Volkmann principle, compressive force across the medial femoral physis leads to growth retardation.
Damaged cartilage ossifies in a delayed fashion. As growth is selectively inhibited at the medial side of the knee due to these compressive forces, a resultant varus deformity progresses. The posteromedial aspect of the physis is most suppressed, contributing to the procurvatum deformity also seen in the disease. However, it is important to note that histologic changes are seen in the entirety of the growth plate, but the medial side is most affected.
Cook et al demonstrated the degree of growth inhibition in children, showing that in an obese 5-year-old child with 10° of varus angulation, sufficient force across the growth plate is generated to retard physeal growth. [9] The relation between obesity and deformity is more linear in the late-onset population than in early-onset Blount disease. [10]
A dynamic component to the overload also has been described, due to the large thigh girth of these patients. The resultant “fat thigh gait” has been implicated as causing a varus movement on the knee contributing to medial overload. The result is a progressive varus angulation below the knee and an increase in the compressive forces on the physis, which changes the direction of the weightbearing forces on the upper tibial epiphysis from perpendicular to oblique. The obliquity of this force tends to displace the tibial epiphysis laterally. In addition to the delayed growth of the physis, pressure on the adjacent epiphysis leads to delayed ossification and intra-articular anomalies.
Disease progression has commonly been believed to be the result of this cycle of growth disturbance, varus deformity, and further growth disturbance. Distal femoral valgus or varus deformity and/or distal tibial varus or valgus deformities also can occur in conjunction with tibia vara. [4, 11] Whether these occur as compensatory mechanisms or are due to intrinsic factors of Blount disease is unknown. These deformities should be corrected at the same time that the tibial vara deformity is corrected.
Whereas the mechanical etiology has been shown to contribute, it does not explain the development of unilateral disease. A number of authors have noted a positive family history of Blount disease in some affected individuals. [12] These studies are limited but worthy of mention. An increased incidence with family history was seen by Bathfield, [13] but without a clear pattern of inheritance. Sevastikoglou and Eriksson found four persons with tibia vara in the same family, of whom two were identical twins. [14] Blount disease has a multifactorial etiology to which various genetic, environmental, and biomechanical factors contribute.
It is important to distinguish that there is controversy as whether the two forms of the disease have similar pathophysiology. Some authors have emphasized the similarities between the two forms, whereas others have considered them separate entities. Adolescent Blount disease does not appear to be as progressive or as common as the infantile form. Factors such as injury or infection of the physis have been suspected to play an etiologic role; however, most patients have no history of trauma or infection, which has led many authors to discount these as the only possible causes. [15, 16, 17]
Etiology
The cause of Blount disease remains controversial, but it is most likely secondary to a combination of hereditary and developmental factors.
The disease has an increased incidence in overweight children who walk at an early age. [18] These findings have led to theories that mechanical overloading of the proximal tibia contributes to Blount disease. The mechanical overload of the physis is attributed to obesity and varus deformity. [19] It is clear, however, that mechanical factors in isolation cannot cause the disease, given that the infantile form is often seen in children with normal weight.
An association between vitamin D deficiency and Blount disease has been suggested, [20] but an independent association between the two, without regard to obesity, has not been proved. [21]
The disease has a genetic component as well, but a direct pattern of inheritance has not been shown. Clearly, the etiology of Blount disease is multifactorial and may differ in the early- and late-onset forms of the disease.
Epidemiology
The epidemiology of Blount disease is not well documented. Large series of patients with Blount disease indicated that the estimated prevalence is less than 1% in the United States. [22] In South Africa, it was estimated by Bathfield and Beighton to be 0.03%. [13] There is an increased incidence of disease in the African American population for both early- and late-onset Blount disease. [23, 24]
Predisposition to Blount disease has been attributed to race, genetics, age at walking, and obesity. Blount disease has increased prevalence in the overweight African American population and in the Scandinavian population. Increased occurrence has been seen in South Africa. [13]
Demographics appear to differ somewhat between early-onset and late-onset forms of the disease. In a meta-analysis by Rivero et al, those patients with the early-onset form Blount disease were more likely to have bilateral involvement and were less likely to be male or African American. [25]
Prognosis
In long-term follow-up of infantile tibia vara, Doyle et al found that the outcome depended on the patient's age and the severity of deformity at the time of intervention. [26] An understanding of the natural history of Blount disease is important for treatment. The prognosis in the infantile form of Blount disease must be considered separately from that in the adolescent form. Infantile tibia vara has a good prognosis, and recurrence rates of deformity are low when the condition is treated at a young age and an early stage.
Untreated infantile tibia vara is believed to be progressive. Whereas partial or complete regression may occur in the early stages of disease, later stages continue to progress and eventually lead to joint degeneration. In the late-onset form of the disease, regression does not occur and the varus deformity may worsen over time. These patients may eventually develop sequelae as a result of joint malalignment.
Data on long-term follow-up of Blount disease are limited, and further studies are needed to characterize the relationship between the deformity and the development of arthroses. Severity of deformity has been shown to correlate with severity of proximal tibial deformity, and poor outcomes appear to be related to the degree of physeal damage. With advances in treatment, retrospective studies on different treatment groups may show whether progression to arthrosis is a significant concern.
-
10-year-old boy with Blount disease. Marked obesity and bilateral genu varum are present. Courtesy of S Standard, MD.
-
Anteroposterior radiograph of knee demonstrating medial plateau depression and prominent metaphyseal beaking (Langenskiöld stage II-III) typical of infantile genu varum regardless of age of presentation.
-
Diagram depicting radiographic changes in infantile form of Blount disease described by Langenskiöld.
-
14-year-old boy with unilateral Blount disease demonstrating tibia vara on left. Courtesy of S Robert Rozbruch, MD.
-
5-year-old girl with Blount disease. Courtesy of Austin T Fragomen, MD.
-
Anteroposterior radiograph of knee and tibia in 5-year-old demonstrating medial plateau depression and prominent metaphyseal beaking (Langenskiöld III) typical of infantile genu varum. Courtesy of Austin T Fragomen, MD.
-
Anteroposterior radiograph of knee and tibia demonstrating metaphyseal-diaphyseal angle (MDA) in child with infantile Blount disease. Courtesy of Austin T Fragomen, MD.
-
Clinical picture of child with infantile Blount disease prior to surgery. Courtesy of Austin T Fragomen, MD.
-
Anteroposterior radiograph of tibia of child with infantile Blount disease at time of distal femoral eight-Plate application tibial osteotomy and Taylor spatial frame. Courtesy of Austin T Fragomen, MD.
-
Subsequent standing hip-to-ankle anteroposterior radiograph of lower extremities demonstrating improved alignment after gradual correction. Courtesy of Austin T Fragomen, MD.
-
Clinical picture of child with infantile Blount disease at completion of treatment. Courtesy of Austin T Fragomen, MD.
-
Clinical picture and anteroposterior radiograph of tibia of child with infantile Blount disease at time of distal femoral eight-Plate application tibial osteotomy and Taylor spatial frame. Bilateral lower extremity films demonstrating overcorrection into valgus. Subsequent standing hip-to-ankle anteroposterior radiograph of lower extremities demonstrating improved alignment after gradual correction with monitoring by clinical pictures and radiographs at most recent visit. Courtesy of Austin T Fragomen, MD.
-
Standing hip-to-ankle anteroposterior radiograph of lower extremities before osteotomy and Taylor spatial frame for treatment of adolescent Blount disease. Patient also had distal femoral malalignment managed with distal femoral osteotomy. Courtesy of S Robert Rozbruch, MD.
-
Clinical photograph of patient before osteotomy and Taylor spatial frame for treatment of adolescent Blount disease. Patient also had distal femoral malalignment managed with distal femoral osteotomy. Courtesy of S Robert Rozbruch, MD.
-
Standing hip-to-ankle anteroposterior radiograph of lower extremities after osteotomy and Taylor spatial frame for treatment of adolescent Blount disease. Patient also had distal femoral malalignment managed with distal femoral osteotomy. Courtesy of S Robert Rozbruch, MD.
-
Clinical photographs of patient after osteotomy and Taylor spatial frame for treatment of adolescent Blount disease. Patient also had distal femoral malalignment managed with distal femoral osteotomy. Courtesy of S Robert Rozbruch, MD.
-
Standing hip-to-ankle anteroposterior radiograph of lower extremities after osteotomy and Taylor spatial frame for treatment of adolescent Blount disease. Patient also had distal femoral malalignment managed with distal femoral osteotomy. Courtesy of S Robert Rozbruch, MD.








