Practice Essentials
A boutonnière (buttonhole) deformity (BD) may develop either in the acute setting (secondary to trauma) or progressively (secondary to arthritis). The term is used to describe the clinical scenario in which a patient’s finger exhibits pathologic flexion at the proximal interphalangeal (PIP) joint and hyperextension at the distal interphalangeal (DIP) joint (see the image below). [1, 2]
 Boutonnière deformity. Image courtesy of David Bozentka, MD, University of Pennsylvania School of Medicine, published by Medscape (Late Reconstruction of Flexor and Extensor Tendon Injuries at http://www.medscape.com/viewarticle/717388).
Boutonnière deformity. Image courtesy of David Bozentka, MD, University of Pennsylvania School of Medicine, published by Medscape (Late Reconstruction of Flexor and Extensor Tendon Injuries at http://www.medscape.com/viewarticle/717388).
This article will provide an overview of BD, discuss the pathophysiology of the deformity (see below), and delineate the standard approach to management (see Treatment).
Anatomy
A BD manifests after injury to the extensor mechanism of the finger. To understand the pathoanatomy of a BD, it is necessary first to understand the complex normal anatomy of the extensor mechanism of the finger. [3]
Three muscles give rise to the extensor mechanism of the fingers: the extensor digitorum communis (EDC) muscle, the lumbrical muscle, and the dorsal interosseous muscle. The EDC trifurcates into a single central slip and two lateral slips as it passes dorsal to the proximal phalanx and proximal to the PIP joint (see the image below).
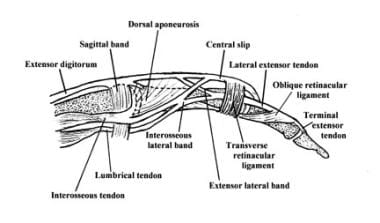
The central slip traverses the PIP joint dorsally and inserts at the dorsal base of the middle phalanx, extending the PIP joint when the extensor mechanism is fired. Each lateral slip advances radially or ulnarly to insert on the radial or ulnar conjoint lateral band. It is important to note that the two lateral bands normally pass dorsal to the axis of rotation of the PIP joint and eventually fall dorsally to coalesce with each another and insert at the dorsal base of the distal phalanx, working to extend the DIP joint when the extensor mechanism is fired.
Both the lumbrical muscle and the dorsal interosseous muscle contribute to the conjoint lateral bands distally, further generating an extension force at the DIP joint.
Pathophysiology
A BD occurs as a consequence of disruption of the central slip of the extensor tendon and attenuation of the triangular ligament, which connects the lateral bands to the terminal tendon. This disruption permits each of the conjoint lateral bands of the digit to slide volarly. Once the lateral bands slide volar to the axis of rotation of the PIP joint, this joint is subjected to a pathologic flexion force and an extension lag; all tendons traversing the PIP joint in this setting elicit flexion of the joint. (See the images below.)
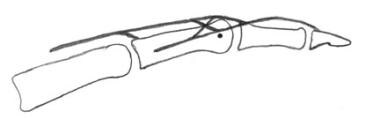 Normal lateral band location, dorsal to axis of rotation of proximal interphalangeal joint.
Normal lateral band location, dorsal to axis of rotation of proximal interphalangeal joint.
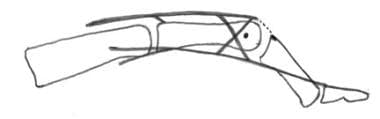 After central slip disruption, lateral bands migrate volar to axis of rotation of proximal interphalangeal joint.
After central slip disruption, lateral bands migrate volar to axis of rotation of proximal interphalangeal joint.
Shortly after the disruption of the central slip, the dorsal interphalangeal joint may experience an extensor lag; however, under the pull of the lumbrical and interosseous muscles, the untethered conjoint lateral bands contract and eventually create a pathologic extension force across the DIP joint. This occurs as the triangular ligament becomes further attenuated and the transverse retinacular ligaments contract.
With the DIP joint in hyperextension, the oblique retinacular ligament, which is located at the dorsal DIP joint, will contract over time, contributing to the hyperextension deformity of this joint.
Etiology
BDs may develop secondary to trauma (including a direct laceration to the extensor mechanism), secondary to rheumatoid arthritis (RA), and in the setting of burns. There are even reports of congenital BDs. [4] The pathogenesis of a BD varies according to its etiology. [3]
Patients who suffer a traumatic BD may have been subject to a direct injury to the central slip or a force that placed the central slip on stretch, leading to failure of the extensor mechanism. Direct injuries can occur when lacerations disrupt the central slip. Central slip injuries may also occur in the setting of passively forced flexion of an actively extended PIP joint. In another scenario, a volar PIP joint dislocation can avulse the dorsal lip of the middle phalanx base and create a central slip disruption.
BDs in the setting of RA develop and progress over time as the soft tissues of the digit are compromised. Specifically, synovial proliferation within the PIP joint results in stretching of the extensor mechanism. Consequently, a subtle extensor lag may develop as the central slip is unable to achieve full extension.
With the PIP joint in slight flexion, the lateral bands are subluxated volarly and become fixed volar to the axis of rotation. Furthermore, the oblique retinacular ligaments contract, resulting in hyperextension and restricted flexion at the DIP joint. Early in the progression of the deformity, the joints remain passively correctable; however, over time, capsular tissues contract and fibrosis occurs within and around the PIP joint. At this time, the BD becomes a fixed deformity. [5]
BDs secondary to burns may occur due to direct injury of the central slip, as in the case of a full-thickness burn. Alternatively, the central slip may be injured by the onset of an infection; in rare cases, the central slip may undergo ischemic necrosis resulting from the pressure of an overlying eschar. [6, 7]
Case reports have described congenital BDs. [8, 9] Such cases offer an interesting perspective into how altered anatomy may affect the forces across the metacarpophalangeal (MCP), PIP and DIP joints. In one such report, Kim et al described BDs of bilateral little fingers secondary to an extensor mechanism that failed to trifurcate into a central slip and two lateral bands and that consequently failed to insert at the dorsal base of the middle phalanx. [4] Presumably as a result, the triangular ligament also failed to develop.
-
Lateral view of relevant finger anatomy.
-
Normal lateral band location, dorsal to axis of rotation of proximal interphalangeal joint.
-
After central slip disruption, lateral bands migrate volar to axis of rotation of proximal interphalangeal joint.
-
Boutonnière deformity. Image courtesy of David Bozentka, MD, University of Pennsylvania School of Medicine, published by Medscape (Late Reconstruction of Flexor and Extensor Tendon Injuries at http://www.medscape.com/viewarticle/717388).
-
Radiographic evidence of boutonnière deformities. Image courtesy of Radiopaedia.org; case by Dr Aditya Shetty (http://radiopaedia.org/cases/rheumatoid-arthritis-13).
-
Bunnell safety-pin splint.
-
Boutonnière deformity.








