Practice Essentials
The eponym Monteggia fracture is most precisely used to refer to a dislocation of the proximal radioulnar joint (PRUJ) in association with a forearm fracture, most commonly a fracture of the ulna. These injuries are relatively uncommon, accounting for fewer than 5% of all forearm fractures. The mechanism of injury is most often a fall on an outstretched hand.
The ulna fracture is usually clinically and radiographically apparent. Findings associated with the concomitant radial head dislocation are often subtle and can be overlooked. The keys to successful diagnosis of a Monteggia fracture are clinical suspicion and radiographs of the entire forearm and elbow. Properly assessing the nature of this injury in a timely fashion is imperative in order to prevent permanent disability or limb dysfunction. [1]
The first challenge is correctly assessing the extent and nature of the injury. The ulna fracture is usually noted, commonly in the proximal third of the ulna. The olecranon, midshaft, and distal shaft may be involved. In his classic 1943 text, Watson-Jones stated that "no fracture presents so many problems; no injury is beset with greater difficulty; no treatment is characterized by more general failure." [2]
Some injuries associated with radiocapitellar dislocation (such as the transolecranon fracture-dislocation of the elbow) are mislabeled as Monteggia lesions, when in fact the PRUJ remains intact. The Monteggia lesion is most precisely characterized as a forearm fracture in association with dislocation of the PRUJ.
The radial head dislocation may not be apparent and will possibly be missed if the elbow is not included in the radiograph. Whenever a fracture of a long bone is noted, the joints above and below should be evaluated with radiographs in orthogonal planes (planes at 90° angles to each other). If one of the forearm bones is injured, injury should be looked for in the other bone and in associated joints of the forearm, elbow, and wrist. This principle also applies to a Galeazzi fracture, which is a fracture of the distal radius with concomitant dislocation of the distal radioulnar joint (DRUJ).
Separate radiographs should be taken of the elbow. The radial head should point towards the capitellum on all radiographs of the elbow.
Unrecognized dislocations may result from reduction of the dislocated radius prior to presentation. This may occur in the field spontaneously or as a result of manipulation by emergency responders. The treating physician may reduce an unrecognized dislocation while reducing or immobilizing the ulna fracture. [3]
Indications for treatment of Monteggia fractures (see Treatment) are based on the specific fracture pattern and the age of the patient (ie, pediatric or adult). Although most pediatric fracture patterns can be managed conservatively with closed reduction and long arm casting, most adult fractures require open reduction and internal fixation (ORIF). Few contraindications for surgery exist. Once the radial head is reduced in closed injuries, surgical treatment may be delayed until the patient is stable and the surgery may be performed in a more elective fashion.
For patient education resources, see the Breaks, Fractures, and Dislocations Center, as well as Broken Arm, Broken Elbow, and Elbow Dislocation.
Anatomy
The anular (annular) and radial collateral ligaments stabilize the radial head. These ligaments stretch or rupture during radial head dislocation. [4] The radial head articulates with the humeral capitellum and the radial notch of the proximal ulna. The radius and ulna are closely invested by the interosseous membrane, which accounts for the increased risk of displacement or injury to the radius when the ulna fractures.
The distal ulna and radius also articulate at the DRUJ. [5] The ulna provides a stable platform for rotation of the radius and forearm. The ulna and interosseous membrane also may provide stable platforms for dislocation of the proximal radius, leading to the Monteggia fracture.
The posterior interosseous nerve travels around the neck of the radius and dives under the supinator as it courses into the forearm. The median and ulnar nerves enter the antecubital fossa just distal to the elbow. The close proximity of these nerves may lead to injuries when a Monteggia fracture occurs. Neural injuries are generally traction injuries and result from stretching around the displaced bone or from energy dispersed during the initial injury.
Pathophysiology
The forearm structures are intricately related, and any disruption to one of the bones affects the other. The ulna and radius are in direct contact with each other only at the PRUJ and the DRUJ; however, they are unified along their entire length by the interosseous membrane. This allows the radius to rotate around the ulna. When the ulna is fractured, energy is transmitted along the interosseous membrane, displacing the proximal radius. The end result is a disrupted interosseous membrane proximal to the fracture, a dislocated PRUJ, and a dislocated radiocapitellar joint.
Radial head dislocation may lead to radial nerve injury. The posterior interosseous branch of the radial nerve, which courses around the neck of the radius, is especially at risk, particularly in Bado type II injuries. [6] Injuries to the anterior interosseous branch of the median nerve and the ulnar nerve also have been reported. Most nerve injuries are neurapraxias and typically resolve over a period of 4-6 months. Splinting of the wrist in extension and finger range-of-motion (ROM) exercises help prevent contractures from developing while the patient awaits resolution of the nerve injury.
Classification
In 1814, Giovanni Battista Monteggia of Milan first described this injury as a fracture to the proximal third of the ulna with associated anterior dislocation of the radial head. [7] Interestingly, he described this injury pattern in the pre-Roentgen era solely on the basis of the history of injury and the physical examination findings. However, this particular fracture pattern only accounts for about 60% of these types of injuries.
More than 150 years later, in 1967, Bado coined the term Monteggia lesion and classified the injury into the following four types [8] :
-
Type I - Fracture of the proximal or middle third of the ulna with anterior dislocation of the radial head (see the first and second images below)
-
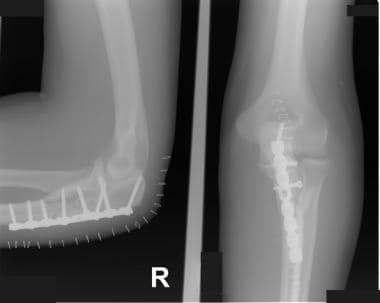
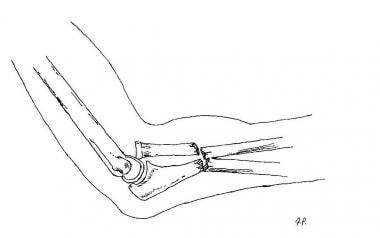
Type II - Fracture of the proximal or middle third of the ulna with posterior dislocation of the radial head (see the third and fourth images below)
-
Type III - Fracture of the ulnar metaphysis with lateral dislocation of the radial head (see the fifth and sixth images below)
-
Type IV - Fracture of the proximal or middle third of the ulna and radius with anterior dislocation of the radial head (see the seventh image below)





The Bado classification is based on the recognition that the apex of the fracture is in the same direction as the radial head dislocation.
Etiology
Monteggia fractures are primarily associated with falls on an outstretched hand with forced pronation. If the elbow is flexed, the chance of a type II or III lesion is greater. In some cases, a direct blow to the forearm can produce similar injuries.
Evans in 1949 [9] and Penrose in 1951 [10] studied the etiology of Monteggia fractures on cadavers by stabilizing the humerus in a vise and subjecting different forces to the forearm. Penrose considered type II lesions a variation of posterior elbow dislocation. Bado believed that the type III lesion, the result of a direct lateral force on the elbow, was primarily observed in children.
In essence, high-energy trauma (eg, a motor vehicle collision) and low-energy trauma (eg, a fall from a standing position) can result in the described injuries. A high index of suspicion, therefore, should be maintained with any ulna fracture.
Epidemiology
Monteggia fractures account for fewer than 5% of forearm fractures, with published literature supporting figures in the range of 1-2%. [11, 12] Of the Monteggia fractures, Bado type I has been reported to be the most common (59%), followed by type III (26%), type II (5%), and type IV (1%). Monteggia fractures are one third as common as the more familiar Galeazzi fractures.
Prognosis
In 1991, Anderson and Meyer used the following criteria to evaluate forearm fractures and their prognosis [13] :
-
Excellent - Union with less than 10° loss of elbow and wrist flexion/extension and less than 25% loss of forearm rotation
-
Satisfactory - Union with less than 20° loss of elbow and wrist flexion/extension and less than 50% loss of forearm rotation
-
Unsatisfactory - Union with greater than 30° loss of elbow and wrist flexion/extension and greater than 50% loss of forearm rotation
-
Failure - Malunion, nonunion, or chronic osteomyelitis
Pain, nerve dysfunction, and cosmetic deformity are other factors to consider in evaluating the outcome of treatment in Monteggia fracture-dislocations. Type II lesions that are associated with ulnohumeral dislocation have been noted to have outcome scores with greater disability than those without ulnohumeral dislocation. [14]
In a retrospective study on the functional and radiologic long-term outcome of ORIF in 11 skeletally mature patients with Bado type I Monteggia fractures, Guitton et al found that the mean arc of elbow flexion increased from 110º at early follow-up to 120º at late follow-up. [5] The mean arc of forearm rotation increased from 145º to 149º. The mean Broberg and Morrey score increased from 89 points to 94 points, and the median Disabilities of the Arm, Shoulder, and Hand (DASH) score was 7 points at long-term follow-up.
In a study evaluating long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in 22 children (14 boys, 8 girls; age range, 4 y to 15 y 11 mo), Nakamura et al noted that the postoperative Mayo Elbow Performance Index (MEPI) at follow-up ranged from 65 to 100, with 19 excellent results, two good results, one fair result, and zero poor results. [14]
In 17 of the 22 patients, the radial head remained in a completely reduced position, and it was subluxated in five patients. [14] Osteoarthritic changes were seen at the radiohumeral joint in four patients. Radiographically, there were 15 good results, seven fair results, and zero poor results. A good radiographic result was seen in all patients who underwent open reduction within 3 years after injury or before reaching 12 years of age.
Datta et al conducted a prospective, longitudinal study of 21 children with Monteggia fracture with dislocation (18 type I, three type III), all of whom were treated by modified Hirayama corrective osteotomy of the ulna with wedge bone grafting, restoration of bone length, reconstruction of the anular ligament using the Bell Tawse method, and fixation of the radial head with transcapitellar Kirschner wire (K-wire). [15] The average follow-up period was 5.5 years.
The investigators evaluated outcomes on the basis of the 100-point MEPI, radiology, and questionnaire. [15] The mean postoperative increase in MEPI score was 30. ROM increased by an average of 30º. Subluxation of the radial head occurred in three patients; one patient experienced transient palsy of the posterior interosseous nerve; and distortion of the radial head (which had no bearing on function) occurred in three.
-
Bado type I lesion. This is the most common type of Monteggia fracture.
-
Bado type I lesion.
-
Bado type II lesion.
-
Bado type II lesion after open reduction and internal fixation.
-
Bado type III lesion with lateral displacement of the radial head.
-
Bado type III lesion with lateral displacement of the radial head.
-
Bado type IV lesion.









