Practice Essentials
Injuries of the lower (subaxial) cervical spine (C3-C7) are among the most common and potentially most devastating injuries involving the axial skeleton. The cervical spine often is injured in motor vehicle accidents and falls, resulting in bony or soft-tissue injury; however, the presence of multiple traumatic injuries may distract the examiner from the cervical spine. In the evaluation of the polytrauma patient, examining the cervical spine is a high priority and must take precedence.
The cervical spine is important to consider in positioning the head in space. The dominant motion in the lower cervical spine is flexion-extension, but the cervical spine's anatomy permits a fair amount of motion in all planes. In high-speed injuries, the head can act as a significant lever arm on the cervical spine and, depending on the mechanism, can create a wide array of injury patterns.
The lower cervical spine can suffer minor bony or ligamentous injury that nevertheless results in severe neurologic injury. However, the converse is also true: Major bony or ligamentous injury to the lower cervical spine can present with only neck pain. Thus, a thorough and orderly approach to the examination is paramount. Recognizing injury to the lower cervical spine is important because of the association between these injuries and spinal cord and nerve root injury. Little room for malalignment exists in the lower cervical spine, and safe and expeditious realignment is of the utmost priority.
In patients presenting to an emergency facility with a history of a high-speed motor vehicle accident, significant head or facial trauma, a neurologic deficit, or neck pain, a cervical spine injury should be assumed to be present until proved otherwise. Whereas assessment of airway, breathing, and hemodynamic stability continues to be the highest priority in caring for the patient with multiple traumatic injuries, central nervous system (CNS) evaluation follows closely behind. The CNS assessment begins in the field; the cervical spine is protected until workup proves that it is not injured.
Medical management involves treating the multiple traumas and, more specifically, treating concomitant neurologic injury. The use of steroids for neurologic injury has become standard to prevent secondary causes of spinal cord damage, such as release of toxic peroxidases, and to minimize associated local edema.
The primary indications for surgical intervention in subaxial cervical injuries include the following:
-
Malalignment of the spine, with or without neurologic deficits
-
Progressive neurologic deterioration in the face of persistent compression from bone or disk fragments
Although malalignment can be managed initially with cervical tong traction, definitive surgical stabilization, with or without decompression, generally is required. (See Treatment.)
Anatomy
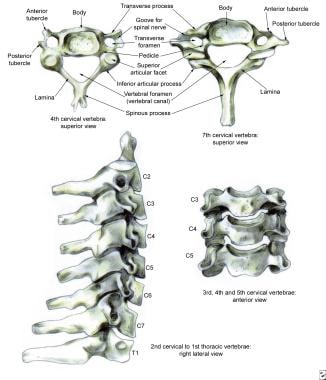
The subaxial cervical spine can conveniently be divided into anterior and posterior columns. The anterior column consists of the typical cervical vertebral body sandwiched between supporting disks. The anterior surface is reinforced further by the anterior longitudinal ligament and the posterior body by the posterior longitudinal ligament, both of which run from the axis to the sacrum. Articulations include the disk-vertebral body, uncovertebral joints, and zygapophyseal joints.
The disk is thicker anteriorly, contributing to the normal cervical lordosis, and the uncovertebral joints located in the posterior aspect of the body define the lateral extent of most surgical exposures. The zygapophyseal or facet joints are oriented at 45º to the axial plane, allowing a sliding motion, as the joint capsule is weakest posteriorly. Supporting ligamentum flavum and posterior and interspinous ligaments also strengthen the posterior column. [1] (See the image below.)
In the neuroanatomy of the cervical spine, the cord is enlarged, with lateral extension of the gray matter consisting of the anterior horn cells. The lateral dimension spans 13-14 mm, and the anterior-posterior extent measures 7 mm. An additional 1 mm is necessary for the cerebrospinal fluid (CSF) anteriorly and posteriorly, as well as 1 mm for the dura. A total of 11 mm is needed for the cervical spinal cord. Exiting at each vertebral level is the spinal nerve root, which is the result of the union of the anterior and posterior nerve roots. (See the image below.)

Interconnections are present between the sympathetic nervous system and the nerve root proper. Because the numbering of the cervical roots commences above the atlas (C1), eight cervical roots exist, with C8 exiting between the seventh cervical vertebra and the first thoracic level.
The vascular anatomy consists of a larger anterior spinal artery located in the central sulcus of the cord and paired posterior spinal arteries located on the dorsum of the cord. It is generally accepted that the anterior two thirds of the cord is supplied by the anterior spinal artery and the posterior one third by the posterior arteries.
Pathophysiology
Various mechanisms may be responsible for ligamentous and bony failure in the subaxial cervical spine. The importance of the position of the head and neck at the time of impact and the direction of force causing injury cannot be overemphasized. Clinical examination and critical review of the imaging studies help determine the type of failure and, therefore, the reconstruction required.
Conceptually, the cervical spine may be viewed as being composed of two columns. An anterior load-bearing structure consists of all structures anterior to and including the posterior longitudinal ligament. The posterior column includes the pedicles, laminae, facet joints, spinous processes, and posterior ligament complexes (ligamentum flavum, interspinous ligaments, and supraspinous ligaments). Tension is resisted by the posterior column, which fails under extreme flexion or distraction and which may be associated with concomitant injury to the anterior column.
Allen et al introduced a comprehensive classification system of injuries, [2] which included the following three common mechanisms:
-
Compression-flexion
-
Distraction-flexion
-
Compression-extension
Vertical compression injury results in the burst-type injury with anterior column failure. Less common modes of insult are the distraction-extension and lateral flexion subtypes. These are classified further into stages of progressive injury. [3]
Etiology
Motor vehicle accidents (MVAs), falls, and accidents resulting from recreational activities are the leading causes of injuries to the lower cervical spine. Motorcycle accidents account for approximately 20% of motor vehicle accidents leading to spinal cord injuries (SCIs). The incidence of falls leading to injury is higher in older persons (≥65 y). Spinal injuries have increased among skiers and snowboarders. [4]
Epidemiology
Cervical spine injury has been reported in 2-4.6% of patients presenting with blunt trauma. It is the most devastating musculoskeletal injury and occurs most frequently in young patients. SCI occurs in more than 11,000 patients per year, or in 40-50 persons per 1 million population. Injuries to the cervical spine produce neurologic damage in approximately 40% of patients. In approximately 10% of traumatic SCIs, radiographs reveal no obvious evidence of bony abnormality.
The age distribution of patients presenting with injuries to the lower cervical spine and spinal cord is bimodal. Injuries in persons aged 15-24 years are usually the result of high-energy trauma, such as MVAs, accidents resulting from sporting activities, or acts of violence. [5] Injuries in persons older than 55 years usually result from low-energy trauma, such as falls from the standing position. The age-associated cervical spondylosis narrows the spinal canal and predisposes the cervical cord to injury at this level. [6]
Prognosis
The clinical outcome after lower cervical spinal injury generally is related to the level and severity of associated SCI. Operative treatment is safe and effective but must be patient- and injury-specific. [7] Incomplete SCIs, as defined by objective motor or sensory preservation below the level of trauma, have the potential for recovery. In general, the sooner the evidence of return, the better the overall prognosis, though recovery may continue for 1 year or longer.
The level of injury also determines the overall functional status of the patient, as follows:
-
The patient with C3- to C4-level SCI must use a sip-and-puff (mouth) or chin/head control for mobilization in a wheelchair
-
Patients with C5-level injuries, as defined by greater than three fifths strength in the respective muscle group, are able to assist with upper-body dressing, can feed themselves with assistive devices, and can operate a power wheelchair
-
Some grooming and assistance with bowel and bladder programs are within the realm of capabilities of the quadriplegic patient with C6-level injuries; these patients are able to feed themselves with hand or tenodesis splints and can transfer to and from wheelchairs or toilets with some assistance
-
Patients with C7-level injuries can transfer independently to the bed, car, or toilet; can use manual or power wheelchairs; and can dress independently using assistive devices
-
Patients with injuries at the C8 level or below should be independent in all transfers and be able to use a manual wheelchair and assist in some homemaking activities
The life expectancy of patients with cervical SCIs has increased with better management of urinary complications. Urinary complications are no longer among the most common causes of death after the first postinjury year.
A study by Raisch et al (N = 275) found that secondary dislocations (sDLs) occurred in 4.0% of patients with surgically treated type B or C subaxial cervical spine fractures; sDLs were frequent after solitary anterior stabilization but rare after posterior or combined stabilization. [8] Older age and concomitant unstable facet joint injury were significantly associated with the development of sDLs.
-
Cross-sectional anatomy of the cervical cord.
-
Normal anatomy of the lower cervical spine.
-
Lateral film of a C5 burst/teardrop fracture.
-
Sagittal CT scan of C5 burst fracture.
-
Axial CT scan of C5 burst fracture.
-
Reduction of C5 burst fracture after tongs traction.
-
Postoperative image of C5 burst fracture; note anterior and posterior fixation.
-
Postoperative image of C5 burst fracture.
-
Standard lateral cervical spine of an 80-year-old patient after a motor vehicle accident; patient has no neurologic deficits and no neck pain.
-
Swimmer's view of the same 80-year-old patient as in Image 9; note the C7-T1 fracture/dislocation.
-
Axial CT scan of C7-T1 fracture/dislocation.
-
Sagittal CT of C7-T1 fracture/dislocation.
-
MRI of C7-T1 fracture/dislocation.
-
Reduction of C7-T1 fracture/dislocation.
-
Postoperative anteroposterior view of C7-T1 fracture/dislocation.
-
Postoperative lateral view of C7-T1 fracture/dislocation.




