Practice Essentials
Traumatic injuries of the scapula have received little attention in the literature because they are uncommon. Scapula fractures account for approximately 1% of all fractures. Historically, they have been treated by closed means. One of the earliest descriptions of treating scapula fractures was published in 1805 in a treatise by Desault. Hardegger et al reported that if significant displacement occurs, conservative treatment alone cannot restore congruence, and stiffness and pain may result, thereby indicating open reduction and stabilization. [1]
Their relative infrequency notwithstanding, scapula fractures have a high association with other injuries. [2, 3, 4] Research has shown that 80-95% of scapula fractures are accompanied by associated injuries, which may be multiple, life-threatening, or both. As a result, diagnosis and treatment of scapular injuries may be delayed or suboptimal. Long-term functional impairment may occur. As more focus is placed on the proper management of scapular injuries, functional outcomes should improve. [5]
Medical therapy for a patient with a scapula fracture generally is the same as that for any trauma patient. Fluid resuscitation is performed, the cardiopulmonary system is stabilized, and life-threatening injuries are addressed before operative fixation of scapula fractures.
Most scapula fractures can be managed effectively with closed treatment. Some injuries with significant displacement have poor long-term outcomes for the shoulder and the upper extremity as a whole if treated with closed techniques. This article reviews closed management of scapula fractures, discusses open treatment, and provides guidelines for injuries that require operative intervention.
Anatomy
The scapula serves as the attachment site for 18 muscles, which link it to the thorax, spine, and upper extremity. (See the image below.) The subscapularis covers the anterior surface, and the serratus anterior attaches to the inferior angle along the anterior medial border. The supraspinatus and the infraspinatus lie on the posterior border of the scapula. Overlying them is the trapezius, which inserts on the spine and the clavicle. The deltoid originates from the scapular spine, acromion, and anterior clavicle. Many other muscles attach to the scapular margins.
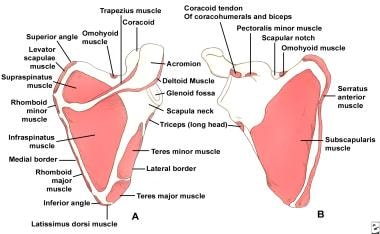
The coracoid process projects from the superior border of the scapula. The coracobrachialis and the short head of the biceps originate from the coracoid, and the pectoralis minor inserts on the coracoid. The brachial plexus and the axillary artery run posterior to the pectoralis minor tendon. The scapular notch lies just medial to the coracoid base and is covered by the transverse scapular ligament. The suprascapular nerve runs under the ligament, and the suprascapular artery passes over it.
The acromion is the lateral projection from the spine of the scapula. The spinoglenoid notch is the gap between the acromion and the glenoid neck of the scapula. The suprascapular nerve and vessels pass through the notch en route to the infraspinatus.
Etiology
Typically, scapula fractures result from high-energy trauma. [6] Direct forces are most common, but indirect mechanisms can also be responsible. An example of an indirect force is a fall on an outstretched arm that causes the humeral head to impact on the glenoid cavity.
Scapula fracture has been reported as a potential complication of reverse total shoulder arthroplasty for rotator cuff tear arthropathy. [7, 8, 9]
Epidemiology
Scapula fractures account for 1% of all fractures, 3% of shoulder-girdle injuries, and 5% of all shoulder fractures. They are reported to account for 0.1% of all pediatric fractures, mostly occurring in children aged 10 years or older. [10]
Approximately 50% of scapula fractures involve the body and spine. Fractures of the glenoid neck constitute about 25% of all scapula fractures, whereas fractures of the glenoid cavity (glenoid rim and fossa) make up approximately 10% of scapula fractures. The acromial and coracoid processes account for 8% and 7%, respectively.
Prognosis
Because of the low incidence of scapula fractures, little in the way of outcome data exists. Hardegger et al reported 79% good-to-excellent results associated with five displaced glenoid neck fractures treated surgically (follow-up, 6.5 y). [1] Kavanaugh et al at the Mayo Clinic reviewed 10 displaced glenoid cavity fractures treated with open reduction and internal fixation (ORIF) and found this to be a useful and safe approach that can restore excellent function of the shoulder. [11]
Nonoperative treatment can sometimes result in malunion, leading to poor range of motion (ROM), chronic pain, and poor cosmesis. Cole et al reported that surgical reconstruction of malunited scapula neck or body fractures can yield good functional and cosmetic outcomes. [12]
Until more data are available, it is reasonable to predict a good-to-excellent functional result if surgical management restores normal or near-normal anatomy, articular congruity, and glenohumeral stability; if surgery provides secure fixation; and if a well-structured and intensive rehabilitation program is implemented. [13, 14, 15, 16, 17]
Bi et al performed a systematic review of the existing literature (42 studies; N = 669) regarding operative (n = 464) and conservative treatment (n = 205) of extra-articular fractures of the scapula. [18] In the operative group, the mean union rate was 99.4%, the Constant score was 84.4, and end forward elevation was 158°; in the nonoperative group, the mean union rate was 85.1%, the Constant score was 79.0, and end forward elevation was 153°.
In a study (N = 74) that included patients with displaced intra-articular or extra-articular scapula fractures who received either surgical (n = 40) or conservative treatment (n = 34), Graafland et al found that functional results in the two groups were similar, even though more complex fractures and more intra-articular fractures were treated surgically. [19] Osteosynthesis of both intra- and extra-articular scapula fractures was safe and led to good functional results.
-
(Click Image to enlarge.) Classification of glenoid cavity fractures: IA - Anterior rim fracture; IB - Posterior rim fracture; II - Fracture line through the glenoid fossa exiting at the lateral border of the scapula; III - Fracture line through the glenoid fossa exiting at the superior border of the scapula; IV - Fracture line through the glenoid fossa exiting at the medial border of the scapula; VA - Combination of types II and IV; VB - Combination of types III and IV; VC - Combination of types II, III, and IV; VI - Comminuted fracture
-
Classification of glenoid neck fractures. Type I includes all minimally displaced fractures. Type II includes all significantly displaced fractures (translational displacement greater than or equal to 1 cm; angulatory displacement greater than or equal to 40°)
-
Superior shoulder suspensory complex. (A) anteroposterior view of the bony/soft tissue ring and the superior and inferior bony struts; and (B) lateral view of the bony/soft tissue ring.
-
Fixation of acromion fractures. (A) tension band construct; and (B) plate-screw fixation (most appropriate for proximal fractures).
-
(Click Image to enlarge.) Scapular anatomy. Muscle origin and insertion.
-
Illustrations depicting fixation techniques available for stabilization of fractures of the glenoid cavity. (1) interfragmentary compression screw; (2) Kirschner wires; (3) construct using Kirschner wires and cerclage wires or Kirschner wires and cerclage sutures; (4) cerclage wire or suture; (5) staple; and (6) 3.5-mm malleable reconstruction plate.
-
Fixation of glenoid neck fractures. (A) stabilization with a 3.5-mm malleable reconstruction plate (note the Kirschner wire running from the acromial process to the glenoid process that can be used for either temporary or permanent fixation); (B) stabilization with 3.5-mm cannulated interfragmentary screws; and (C) stabilization with Kirschner wires (in this case, Kirschner wires passed from the acromion and clavicle into the glenoid process).
-
Illustrations showing techniques for managing coracoid fractures. (A) interfragmentary screw fixation (if the fragment is sufficiently large and noncomminuted), and (B) excision of the distal fragment (if small and/or comminuted) and suture fixation of the conjoined tendon to the remaining coracoid process.









