Practice Essentials
Foot drop is a deceptively simple name for a potentially complex problem. It can be defined as a significant weakness of ankle and toe dorsiflexion. The foot and ankle dorsiflexors include the tibialis anterior, the extensor hallucis longus (EHL), and the extensor digitorum longus (EDL). These muscles help the body clear the foot during swing phase and control plantarflexion of the foot on heel strike.
Weakness in this group of muscles results in an equinovarus deformity. This is sometimes referred to as steppage gait, because the patient tends to walk with an exaggerated flexion of the hip and knee to prevent the toes from catching on the ground during swing phase. During gait, the force of heel strike exceeds body weight, and the direction of the ground reaction vector passes behind the ankle and knee center (see the image below).
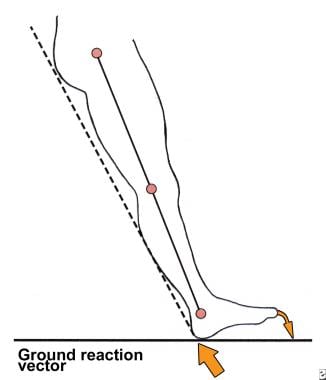
This causes the foot to plantarflex and, if uncontrolled, to slap the ground. Ordinarily, eccentric lengthening of the tibialis anterior, which controls plantar flexion, absorbs the shock of heel strike. Foot drop can result if there is injury to the dorsiflexors or to any point along the neural pathways that supply them.
Foot drop can be associated with a variety of conditions, including dorsiflexor injuries, peripheral nerve injuries, stroke, neuropathies, drug toxicities, or diabetes. The causes of foot drop may be divided into three general categories: neurologic, muscular, and anatomic. These causes may overlap.
Treatment is variable and is directed at the specific cause (see Treatment). Attention to the patient’s psychological needs is very important. Pain should be managed. Optimizing glucose control can also be useful. When foot drop is not amenable to surgical treatment, an ankle-foot orthosis (AFO) is often used. If the foot drop is due to hemiplegia, peroneal nerve stimulation can be considered. Foot drop due to direct trauma to the dorsiflexors generally calls for surgical repair. When nerve insult is the cause of foot drop, treatment is directed at restoring nerve continuity, either by direct repair or by removal of the insult.
Anatomy
Fibers from the dorsal branches of the ventral rami of L4-S1 are found in the peroneal nerve, which is paired with the tibial nerve to constitute the sciatic nerve. The sciatic nerve leaves the pelvic cavity at the greater sciatic foramen, just inferior to the piriformis. It bifurcates to form the peroneal and tibial nerves either in the distal third of the thigh or at the midthigh level.
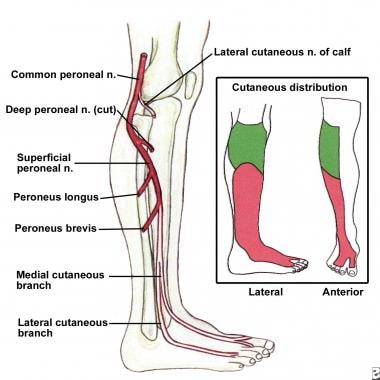
The peroneal nerve crosses laterally to curve over the posterior rim of the fibular neck to the anterior compartment of the lower leg, dividing into superficial and deep branches. The superficial branch travels between the two heads of the peronei and continues down the lower leg to lie between the peroneal tendon and the lateral edge of the gastrocnemius. It then branches to the ankle anterolaterally to supply sensation to the dorsum of the foot (see the image below).
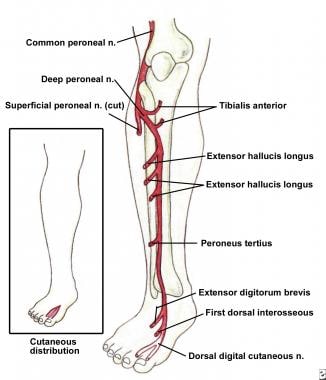
The deep branch divides just after rounding the fibular neck. Its initial branch supplies the tibialis anterior, and the remaining branches supply the EDL, the EHL, and a small sensory patch at the first dorsal web space (see the image below).
The peroneal nerve is susceptible to injury all along its course. In that it is part of the sciatic nerve, its funiculi are relatively isolated from those of the tibial nerve. Therefore, trauma to the sciatic nerve may affect only one of its divisions. The funiculi of the peroneal nerve also are larger and have less protective connective tissue than those of the tibial nerve, making the peroneal nerve more susceptible to trauma. In addition, the peroneal nerve has fewer autonomic fibers; thus, in any injury, motor and sensory fibers bear the brunt of the trauma.
The peroneal nerve runs a more superficial course than the tibial nerve does, especially at the fibular neck, and this relatively exposed position makes it vulnerable to direct insult. Its close adherence to the periosteum of the proximal fibula renders it susceptible to injury during surgical procedures in this area.
Pathophysiology
The pathophysiology of nerve damage that commonly causes foot drop is as follows. The functional integrity of an axon and its target depends on the continued supply of trophic substances synthesized in the neuronal perikaryon and transported down the axon (axoplasmic flow). A laceration interrupts axoplasmic flow; a crush injury may compromise it as well. A double-crush phenomenon occurs when a proximal insult in a nerve root diminishes axoplasmic flow, making it more susceptible to injury.
A distal lesion further compromises axoplasmic flow, and clinical palsy results. This is the phenomenon thought to be responsible for the increased risk of foot drop after hip replacement in a patient with preexisting spinal stenosis. The spinal stenosis causes the proximal compromise, and intraoperative stretch of the sciatic nerve provides the distal insult.
Etiology
Foot drop may follow direct injury to the dorsiflexors. A few cases of rupture of the anterior tibial tendon leading to foot drop and suspicion of peroneal nerve palsy have been reported. This subcutaneous tendon rupture usually occurs after a minor trauma with the foot in plantarflexion.
Compartment syndromes also may lead to foot drop. These are surgical emergencies and are not associated only with fracture or acute trauma. March gangrene, a form of anterior compartment syndrome, is thought to be due to edema and small hemorrhages in the muscles of the anterior compartment occurring after strenuous activity in individuals not accustomed to it. Deep posterior compartment syndrome also may result in foot drop as a late sequela due to contracture formation.
Neurologic causes of foot drop include mononeuropathies of the deep peroneal nerve, the common peroneal nerve, or the sciatic nerve. Lumbosacral plexopathy, lumbar radiculopathy, motor neuron disease, or parasagittal cortical or subcortical cerebral lesions also can manifest as foot drop. These lesions can be differentiated by means of clinical and electrodiagnostic examinations.
A common behavioral cause of foot drop is habitual crossing of the legs. [1] These cases typically resolve with discontinuance of the habit.
Foot drop may be of iatrogenic origin (eg, resulting from traction applied during treatment of a fracture [2] ).
Foot drop also may be seen as a combination of neurologic, muscular, and anatomic dysfunction. Charcot foot is one example.
Epidemiology
Peroneal neuropathy caused by compression at the fibular head is the most common compressive neuropathy in the lower extremity. Foot drop is its most notable symptom. All age groups are affected equally, but the condition is more common in males (male-to-female ratio, 2.8:1). About 90% of peroneal lesions are unilateral, and they can affect the right or the left side with equal frequency.
A foot drop of particular concern to orthopedic surgeons is the peroneal nerve palsy seen after total knee arthroplasty (TKA; 0.3-4% of cases) or proximal tibial osteotomy (3-13% of cases). Ischemia, mechanical irritation, traction, crush injury, and laceration can cause intraoperative injury to the peroneal nerve. It has also been suggested that correction of a severe valgus or flexion deformity can stretch the peroneal nerve and lead to palsy. Postoperative causes of peroneal nerve palsy include hematomas and constrictive dressings.
In a study by Cohen et al, the relative risk of palsy was 2.8 times higher with epidural anesthesia for TKA than with general or spinal anesthesia. [3] Epidural anesthesia probably decreased proprioception and sensation (intraoperatively and, to some extent, postoperatively), allowing the limb to rest in an unprotected state susceptible to local compression. In addition, intraoperative neurologic damage may not have been readily apparent in the immediate postoperative period, because of ongoing effects of epidural anesthesia.
In the same study, the relative risk of palsy was 6.5 times greater in patients who had a prior lumbar laminectomy. [3]
A series of patients who developed foot drop after primary hip arthroplasty were carefully examined and found to have spinal stenosis. [4] As many as 70% of patients undergoing hip arthroplasty have electromyographic (EMG) evidence of nerve injury, but they rarely have clinical symptoms. [5] Patients with preexisting spinal stenosis are believed to be at increased risk for foot drop after hip arthroplasty because of this proximal compromise; this is the double-crush phenomenon.
Prognosis
Prognosis and outcome vary according to the cause of the foot drop. In a peripheral compressive neuropathy, recovery can be expected in up to 3 months, provided that further compression is avoided. A partial peroneal nerve palsy after total knee replacement has a uniformly good prognosis. [6] A variable amount of recovery is seen with a complete postoperative palsy. Follow-up EMG and nerve conduction studies may be useful for assessing recovery.
A partial palsy recovers faster because of local sprouting. With complete axonal loss, reinnervation is achieved solely through proximal-to-distal axonal growth, which usually proceeds at a rate of 1 mm/day. Thus, injuries of a nerve close to its target muscle also have a more favorable outcome. In a nerve root compressive neuropathy, one study concluded that severe motor weakness lasting longer than 6 months, a negative straight leg-raising test, and old age were poor prognostic factors for recovery of dorsiflexion. [7]
When there is direct injury to the peroneal nerve, the outcome is more favorable for penetrating trauma than for blunt trauma; a traction or stretch injury to the nerve has an intermediate outcome. When nerve grafting is performed, functional recovery depends on the severity of injury and thus on the length of the graft used. With grafts longer than 12 cm, good functional recovery is rare.
Wound infection may occur after surgical treatment, as may nerve graft failure. In tendon transfer procedures, recurrent deformity has been reported. In arthrodeses or fusion procedures, pseudoarthrosis, delayed union, or nonunion may be noted.
In a study evaluating factors predictive of short- and long-term recovery outcomes after surgery for foot drop secondary to lumbar degenerative disease, Berger et al determined that whereas early surgery may improve the recovery rate in these patients, the strongest predictor of the extent of recovery was the severity of preoperative tibialis anterior muscle weakness. [8] Maximal recovery in the short-term postoperative period was associated with sustained long-term functional improvement and independence.
-
Diagram of ground reaction vector during heel strike.
-
Common and superficial peroneal nerves, branches, and cutaneous innervation.
-
Deep peroneal nerve, branches, and cutaneous innervation.
-
Incisions for Bridle procedure.
-
Posterior leg with retrieved posterior tibial tendon above ankle. Window in interosseous membrane is labeled with X.
-
Posterior tibial tendon (C) is pulled through slit in anterior tibial tendon (A) and inserted into second cuneiform. Posterior tibial tendon is anastomosed to anterior tibial tendon and distal stump of peroneus longus (B) that has been rerouted anterior to lateral malleolus.
-
Gait of patient with foot drop.






