Practice Essentials
Lattice corneal dystrophy is a rare inherited condition characterized by amyloid deposition in the corneal stroma. It is a bilateral, slowly progressive disease that results in recurrent corneal erosions and decreased vision due to opacification of the cornea. There are two genetically distinct types of lattice corneal dystrophy: lattice corneal dystrophy type I (classic type), which is a primary amyloidosis localized to the corneas only, and lattice corneal dystrophy type II (gelsolin type, or Meretoja syndrome), which has systemic amyloidosis manifestations.
The onset of corneal changes generally occurs in the first decade of life in lattice corneal dystrophy type I and in the fourth or fifth decade of life in lattice corneal dystrophy type II. Affected individuals may first develop recurrent corneal erosion syndrome, which is a recurring painful breakdown of the corneal epithelium. Vision compromise generally occurs much later as the density of amyloid deposits in the corneal stroma increases.
Under slit-lamp examination, early manifestations of lattice dystrophy include subtle anterior stromal opacities or small refractile linear lesions. Later manifestations include thicker, radially oriented branching lines that form a latticelike pattern. Later in the course of disease, lattice lines extend to the corneal periphery and progress to deep stroma. [13, 15]
Lattice corneal dystrophy is inherited in an autosomal-dominant fashion. The genetic defect of lattice corneal dystrophy type I has been mapped to the TGFBI (BIGH3) gene on chromosome 5q. [3, 4] Lattice corneal dystrophy type II results from a mutation in the GSN gene.
Treatment of lattice corneal dystrophy includes management of recurrent corneal erosion syndrome and rehabilitation of lost visual acuity. Recurrent erosion syndrome may be treated with hypertonic saline drops, lubricating drops, bandage contact lenses, or laser surface ablation. When compromised visual acuity occurs, treatment options include laser surface ablation and partial or full-thickness corneal transplantation. These treatment modalities have a high success rate, and most patients are able to retain good visual acuity throughout life with proper care.
Background
Lattice corneal dystrophy (LCD), an IC3D category 1 dystrophy, is an autosomal-dominant condition and one of the most common stromal dystrophies. It is a slowly progressive disease that results in significant discomfort and visual impairment.
There are two genetically distinct types: lattice corneal dystrophy type I (classic type), which is isolated to the eye, and the less common lattice corneal dystrophy type II (gelsolin type), which has systemic amyloidosis manifestations. [1] Although lattice corneal dystrophy type II is regarded as a type of familial amyloidosis and not a true corneal dystrophy, it can be easily misdiagnosed as lattice corneal dystrophy type I. [2]
Like granular and Avellino dystrophies, the genetic defect of lattice corneal dystrophy type I has been mapped to the TGFBI (BIGH3) gene on chromosome 5q. [3, 4] Lattice corneal dystrophy type II results from a mutation in the GSN gene. Onset of corneal changes in lattice corneal dystrophy type I usually occurs in the first decade of life, although patients may remain asymptomatic for years. Examination of the cornea in the second to third decade of life reveals branching, refractile lattice lines with intervening haze, which are observed best in retroillumination.
An example of lattice corneal dystrophy is shown in the image below.
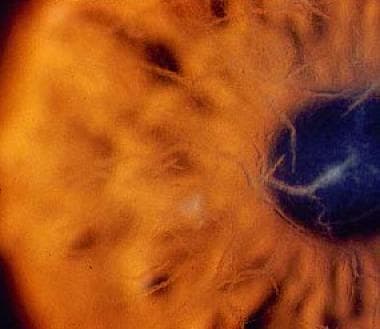 Lattice corneal dystrophy. Image courtesy of James J. Reidy, MD, FACS, Associate Professor of Ophthalmology, State University of New York, School of Medicine & Biomedical Sciences, Buffalo, New York.
Lattice corneal dystrophy. Image courtesy of James J. Reidy, MD, FACS, Associate Professor of Ophthalmology, State University of New York, School of Medicine & Biomedical Sciences, Buffalo, New York.
Pathophysiology
The cornea is the clear outer coat of the front of the eye. A dystrophy of the cornea is defined as a bilateral noninflammatory clouding of the cornea. Corneal dystrophies can be placed into 3 categories based on their location within the cornea: (1) Anterior corneal dystrophies affect the corneal epithelium and may involve the Bowman layer, (2) stromal corneal dystrophies affect the central layer of the cornea (the stroma), and (3) posterior corneal dystrophies involve the Descemet membrane and the endothelium.
Lattice corneal dystrophy is primarily a stromal corneal dystrophy that starts as fine, branching linear central opacities in the Bowman layer and that spread to the periphery. Although the process may involve the deep stroma, it does not reach the Descemet membrane.
The age of onset for most corneal dystrophies is less than 20 years (exceptions include map-dot-fingerprint dystrophy and Fuchs corneal dystrophy). Most corneal dystrophies are inherited in a dominant pattern. Exceptions include macular corneal dystrophy, type 3 lattice corneal dystrophy, and the autosomal-recessive form of congenital hereditary endothelial dystrophy.
Epidemiology
Frequency
United States
Although lattice corneal dystrophy type I is one of the most common stromal dystrophies in the Western world, it is still relatively rare. [5, 1]
International
Cases of lattice corneal dystrophy type I have been recognized throughout the world. Lattice corneal dystrophy type II is most common in Finland. [6]
Mortality/Morbidity
Excessive corneal erosions can lead to decreased visual acuity, which may require a corneal transplant or phototherapeutic keratectomy (PTK).
Sex
No sexual predilection is noted.
Age
In lattice corneal dystrophy type I, onset of the corneal changes such as recurrent epithelial erosions usually occurs in the first decade of life, although patients may remain asymptomatic for years. Examination of the cornea in the second to third decade of life reveals branching, refractile lattice lines, which are observed best in retroillumination. Over time, the lattice lines and other opacities coalesce, forming anterior stromal haze that decreases visual acuity. Onset of corneal changes in lattice corneal dystrophy type II occurs at age 30-40 years, but most patients do not experience symptoms until their seventh decade of life. [2]
Prognosis
Lattice corneal dystrophy demonstrates variable penetrance and expression. Typically, lattice corneal dystrophy type I becomes clinically apparent by age 10 years; however, decreased visual acuity is common after age 40 years. Morbidity associated with painful recurrent erosions is also common. Patients with lattice corneal dystrophy type II commonly present between age 30 and 40 years, retain good visual acuity until age 60 years or later, and infrequently develop recurrent corneal erosions. [2]
The predominantly bilateral nature of lattice corneal dystrophy type I and type II contributes to the morbidity of this condition. The painful recurrent erosion syndrome associated with lattice corneal dystrophy may result in frequent visits to the ophthalmologist and loss of productivity. Loss of visual acuity may progress from mild blurring of vision to debilitating blindness. Fortunately, recurrent erosions and vision loss due to corneal opacity are treatable.
Patients with lattice corneal dystrophy type II may develop pseudoexfoliation and glaucoma in addition to corneal deposits. Systemic manifestations include cranial and peripheral neuropathies, which can result in facial paresis, loss of peripheral vibration sense and touch, orthostatic hypotension, and/or cardiac conduction abnormalities. Therefore, these patients require comanagement with appropriate medical specialists. [17]
Patient Education
Patients should be educated regarding the autosomal-dominant inheritance of lattice corneal dystrophy and understand its implication in childbearing.
Family members should be counseled to establish care with an ophthalmologist, even during childhood or adolescence.
Patients should be educated on the natural history of lattice corneal dystrophy, including issues surrounding recurrent corneal erosion syndrome and loss of corneal clarity. They should be informed that treatment options are available and that, despite the recurrent nature of the condition, proper management often enables good visual acuity throughout the patient’s lifetime.
Patients with lattice corneal dystrophy type II should be educated on the systemic manifestations of amyloidosis and be referred to the appropriate medical specialist.
-
Lattice corneal dystrophy. Image courtesy of James J. Reidy, MD, FACS, Associate Professor of Ophthalmology, State University of New York, School of Medicine & Biomedical Sciences, Buffalo, New York.
-
Slit lamp image of lattice corneal dystrophy. Image courtesy of James J. Reidy, MD, FACS, Associate Professor of Ophthalmology, State University of New York, School of Medicine & Biomedical Sciences, Buffalo, New York.
Tables
Feature |
Granular Dystrophy |
Macular Dystrophy |
Lattice Dystrophy |
|---|---|---|---|
Age of onset |
First decade of life |
First decade of life |
First decade of life |
Heredity |
Autosomal dominant |
Autosomal recessive |
Autosomal dominant |
Reduced vision |
Fourth or fifth decade of life |
First or second decade of life |
Second or third decade of life |
Erosions |
Uncommon |
Common |
Frequent |
Opacities |
Discrete, intervening stroma Clear, not to limbus |
Indistinct margins, intervening Stroma hazy, extends to limbus |
Refractile lines and dots Usually not to limbus |
Material |
Hyaline |
Glycosaminoglycans |
Amyloid |

