Practice Essentials
Open angle glaucoma (OAG) is a multifactorial optic neuropathy characterized by progressive retinal ganglion cell death and characteristic visual field pattern loss. Glaucoma is an increasingly important cause of blindness as the world's population ages. It is the second leading cause of blindness globally, but the blindness it causes is a greater public health challenge than that caused by cataracts and unaddressed refractive errors, the top two causes of blindness.
No cure is available for glaucoma, but, in some cases, disease progression can be controlled. Even with effective treatment, patients must have regular eye examinations. Treatment often continues for the patient's lifetime.
Lowering the intraocular pressure (IOP) is the focus of treating patients with glaucoma. Lowering IOP is done to a level to limit further optic nerve damage; this level is referred to as the target pressure and is determined by the ophthalmologist based on the structural and functional examination of each patient. The target IOP differs for each patient, and a patient's target pressure may change during the course of a lifetime. The IOP may be controlled by medical or surgical therapy.
In addition to topical and oral pharmacologic agents, laser trabeculoplasty procedures help open the trabecular meshwork to aid the outflow of anterior chamber fluid. Other procedures have focused on destruction of the ciliary processes that produce aqueous humor.
The use of daily topical medications is burdensome for patients, and adherence with daily drops is reportedly very low. Responses to topical medications and laser treatments are variable, and may not be effective in the long term for controlling IOP. For these reasons, incisional surgical techniques have been developed to increase the drainage of aqueous humor in those who fail to respond to or who are nonadherent with topical therapy.
These techniques include implanting artificial drainage valves (tube shunts) and surgically cutting additional passageways to drain the fluid by filtering surgery (trabeculectomy or Xen Gel stent). Complications associated with filtering surgery include infection, cataracts, bleeding, hypotony, and filtration failure.
Primary open angle glaucoma (POAG) is characterized by an elevated IOP at some point during the course of the disease with an open anterior chamber angle and a characteristic optic nerve and/or visual field change in the absence of concurrent ocular disease. Primary open-angle glaucoma, the most common form of glaucoma, is characterized by a chronic insidious onset. In primary open-angle glaucoma, elevated IOP likely results from low-grade obstruction of aqueous humor outflow in the trabecular meshwork. Elevated IOP, in turn, can produce mechanical and/or ischemic damage to the optic nerve. The onset is usually insidious and asymptomatic, with changes in the visual field not generally noticeable until late in the disease, when cupping of the optic disc can be seen.
Secondary glaucoma is characterized by elevated IOP associated with concurrent ocular disease. A few examples of secondary glaucoma causes include pigment dispersion and pseudoexfoliation syndrome, uveitis with the formation of peripheral anterior synechiae in the iridocorneal angle, intraocular hemorrhage with trabecular meshwork obstruction, intraocular neoplasia, and lens displacement.
Surgical intervention is indicated in the following circumstances:
-
Patients with uncontrolled intraocular pressure (IOP) on maximum tolerated medical therapy in the presence of significant changes in the optic disc and/or visual field
-
Noncompliance with topical medial therapy
-
Advanced optic nerve or visual field changes found early in the presentation
Critical factors for surgical interventions are individually based and depend on the amount of functional vision loss, the rapidity of visual deterioration, and the patient's life expectancy.
The primary objectives of trabeculectomy are to maintain useful vision and to avoid further glaucomatous damage by lowering the IOP. [1]
Workup
Clinical evaluation to screen, diagnose, and detect progression of glaucoma includes a slit lamp exam, tonometry, gonioscopy, ophthalmoscopy, central corneal thickness, corneal hysteresis, visual field tests, and imaging studies. Slit lamp is used to examine the anterior segment structures, especially for signs of pigmentary glaucoma (PG). PG presents with trabecular meshwork heavy pigmentation due to an accumulation of iris pigment. The slit lamp can also be used to measure the depth of the anterior chamber to determine the drainage angle.
Imaging studies use laser, light, and sound waves to provide quantitative analysis of the optic disc, retinal nerve fiber layer, and ganglion cell layer, which are affected in glaucoma. Imaging modalities include optical coherence tomography (OCT), heidelberg retina tomography (HRT), and scanning laser polarimetry (SLP).
Medical Treatment
Topical medications increase the outflow of aqueous humor from the eye or decrease the amount of aqueous humor produced. Systemic adverse effects can be reduced and higher intraocular concentration of medication can be achieved with topical medications compared to oral drugs. Topical medications include miotics (eg, pilocarpine, carbachol), prostaglandin analogs (eg, latanoprost), epinephrine compounds, beta-blockers (eg, timolol, betaxolol), local carbonic anhydrase inhibitors, and alpha-adrenergic agonists (eg, clinidine, apraclinidine, brimonidine).
Oral medication can control IOP. Carbonic anhydrase inhibitors (CAIs; acetazolamide and methazolamide), which slow the production of aqueous humor in the eye, are the most common. Systemic CAIs have been shown to reduce IOP by 20% to 30%. [2]
Many of the same medications used to treat patients with open-angle glaucoma are used to treat patients with angle-closure glaucoma, which can cause IOP to rise quickly. To rapidly lower the pressure to prevent vision loss, the opthalmologist may administer a hyperosmotic agent. The effects of this drug last only 6 to 8 hours; therefore, it is not used for the long-term management of glaucoma.
Possible adverse effects associated with glaucoma medication include the following: (see Glaucoma Medications for further details)
-
Stinging or redness of eyes
-
Blurred vision
-
Headache
-
Bradycardia or bronchospasm
-
Changes in sexual desire
-
Mood changes
-
Tingling of fingers and toes
-
Drowsiness
-
Loss of appetite
-
Change of iris color (in patients with light-colored eyes taking prostaglandin analogs)
Surgical Treatment
For some patients, surgery might be the best option. Surgery may be performed first or after attempts to lower IOP with medications are tried. Several types of surgery are available to treat patients with glaucoma. The type and the severity of the glaucoma, the patient's other ocular diseases, and the patient's health are all considerations in selecting the type of operation. Surgery may be performed by using a laser or with more conventional approaches, such as incisional surgery, viscocanalostomy, or tube shunt placement.
Laser surgery
Laser surgeries include trabeculoplasty, idridotomy, and cyclophotocoagulation.
Most laser surgeries can be performed in the ophthalmologist's office or in an outpatient surgical facility. Because patients usually have little discomfort, eye drops are used to numb the eye for topical anesthesia. Recovery is quick, and patients may have local eye irritation, but they can usually resume their normal activities within 1 to 2 days.
Incisional surgery
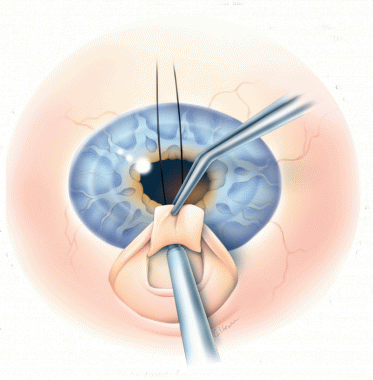
Filtering surgery (trabeculectomy) is usually performed in a hospital or in an outpatient surgical center with local anesthesia and sometimes sedation. Using delicate instruments, the ophthalmic surgeon removes a tiny piece of the sclera, leaving a tiny hole where aqueous humor can flow into a space between the conjunctiva and sclera, thereby reducing IOP. The bloodstream then reabsorbs the aqueous humor.
Some patients require the placement of a glaucoma drainage device or tube shunt (eg, Ahmed, Molteno, Baerveldt). This device is adhered to the sclera between the rectus muscles, and a drainage tube is inserted into the anterior or posterior chamber through a tiny incision in the sclera. It allows the fluid to flow out from the interior of the eye, where it can be reabsorbed.
Viscocanalostomy
Viscocanalostomy was developed as an alternative to trabeculectomy. Although many viscocanalostomy techniques are available, the procedure involves production of superficial and deep scleral flaps, excision of the deep scleral flap to create a scleral reservoir, and unroofing of the Schlemm canal.
Shunt placement
The Ex-PRESS shunt is a 3-mm device that is inserted at the edge of the cornea. It is a microscopic conduit that drains excess fluid out of the eye and into the tissues that surround the eye. Standard glaucoma surgeries can take from 30 minutes to 1.5 hours, but surgery with this new shunt takes 10 minutes. According to one study, the incidence of complications after the implantation of an Ex-PRESS shunt directly under the conjunctiva was unacceptably high, despite a significant reduction in the IOP. [3]
Glaucoma surgery is generally performed as an outpatient procedure with the patient under local anesthesia with sedation. Before glaucoma surgery, the ophthalmic surgeon must evaluate the patient carefully to assess for concurrent ocular disease, neovascular glaucoma, uveitis, and/or conjunctival scarring, all of which guide an individualized surgical approach. The surgeon will discuss the specific condition, the details of the procedure to be performed, and the risks and the benefits of the procedure with the patient. The patient is required to sign an informed consent agreement before glaucoma surgery is performed.
Background
Open angle glaucoma (OAG) is a multifactorial optic neuropathy characterized by progressive retinal ganglion cell death and characteristic visual field pattern loss. Glaucoma is an increasingly important cause of blindness as the world's population ages. Statistics gathered by the World Health Organization (WHO) and Vision Loss Expert Group of the Global Burden of Disease Study in 2020 showed that glaucoma is the second leading cause of blindness worldwide, after cataracts and unaddressed refractive errors. [4] However, glaucoma presents a greater public health challenge because the blindness it causes often is progressive and irreversible.
In the United States alone, glaucoma has been diagnosed in about three million people, who are at risk of becoming blind. [5] Therefore, extensive research into the pathophysiology and understanding of glaucoma is underway to help guide pharmacologic and surgical interventions to slow this progressive optic neuropathy.
Elevated intraocular pressure (IOP) is a major risk factor for OAG, and treatment aims focus on reducing and controlling IOP to limit disease progression. [6] Although additional risk factors for glaucoma have been identified, current treatments for decreasing IOP focus on either reducing the production of aqueous humor from the ciliary processes or on increasing the ability of the aqueous humor to drain from the eye via outflow pathways.
Treatments include the use of topical and oral pharmacologic agents to inhibit the production of aqueous humor or to help with the outflow of aqueous humor along the trabecular or uveoscleral pathway. In addition, laser trabeculoplasty procedures have been designed to help open the trabecular meshwork to aid the outflow of anterior chamber fluid. Other procedures have focused on destruction of the ciliary processes that produce aqueous humor.
Despite additional risk factors having been identified, such as a decrease in retrobulbar ocular blood flow, reduction in the IOP remains the only modifiable risk factor proven to slow the progression of glaucoma.
However, use of daily topical medications creates a burden for patients, and studies have reported a very low compliance rate in patients using daily drops. [7] Furthermore, patients often have variable responses to topical medications and laser treatments, and these treatment effects are often limited and ineffective at controlling IOP over many years. As a result of this, incisional surgical techniques have been designed to increase the drainage of aqueous humor in patients unresponsive to or noncompliant with topical therapy. These techniques include implanting artificial drainage valves (tube shunts) and surgically cutting additional passageways to drain the fluid by filtering surgery (trabeculectomy or xen gel). Complications associated with filtering surgery include infection, cataracts, bleeding, hypotony, and filtration failure, which will be discussed in more detail in the latter portion of this article.
History of the Procedure
In 1857, von Graefe found that removing a large piece of the iris helped many patients with glaucoma. Von Graefe's early work on this subject was translated into English and published by the New Sydenham Society in 1859. Eserine eye drops, made from the Calabar bean, were used before iridectomy to produce a miosis so that the iridectomy could be done peripherally in the iris. Occasionally, patients with glaucoma seemed better after using the eserine eye drops, so surgery was not needed. Von Graefe also suggested that patients undergo a visual field examination in the office. Toward the end of the 19th century, glaucoma was considered to be identical to elevated IOP (and vice versa). Low-tension glaucoma, by definition, did not exist.
In 1909, Elliot, who was working at the Government Ophthalmic Hospital in Madras, India, used a trephine to make an anterior sclerectomy under a conjunctival flap, coupled with a peripheral iridectomy, in the attempt to improve on the operation of Lagrange (in Bordeaux). When Elliot reported 50 cases in 1909, he did not know that Fergus (in Glasgow) and Holth (in Christiania) had recently reported similar findings. Elliot's first book, Sclero-corneal Trephining in the Operative Treatment of Glaucoma, appeared in 1913 after he completed 900 cases, and the procedure received worldwide publicity.
Elliot participated in a discussion about glaucoma with Lagrange and Smith (the English-language glaucoma expert) at the International Congress of Medicine in London. Elliot then traveled to America, where he visited many ophthalmic centers and performed his operation 135 more times. Elliot's trephining procedure was more effective than iridectomy in treating patients with chronic glaucoma. For the next 40 years, his trephining procedure took its place beside Holth's iridencleisis as one of the most popular glaucoma operations.
Elliot followed up his first book with annual progress summaries on glaucoma in the Ophthalmic Yearbooks of 1913-1916 and a short book, Glaucoma: A Handbook for the General Practitioner, in 1917. In 1918, he published Glaucoma: A Textbook for the Student of Ophthalmology; in 1922, the enlarged second edition of this book, now called Treatise on Glaucoma, was a significant contribution to ophthalmology, as it improved the quality of teaching about glaucoma and posed questions about the mechanisms of the disease process.
Iridencleisis was eventually abandoned because of fear of sympathetic ophthalmia and postoperative complications of cyclodialysis. Variations of Elliot's trephining procedure are still in use. Scheie's thermal sclerectomy was popular for a while. Cairns' trabeculectomy, developed in 1968, has evolved to a commonly used surgical management method today. Starting with Watson’s modification in 1970, surgical technique and postoperative management of trabeculectomy improved over the past few decades. Postsurgical scarring was one of the biggest complications, which is now better managed with antifibrotics. Surgical technique was modified regarding incision site, flap size, releasable sutures, and closure method.
Subconjunctival microinvasive filtering surgeries, such as Xen gel stent, are increasing in use due to its minimally invasive technique and effectiveness in reducing IOP. [8] Xen gel stent was FDA approved in 2016 and is a surgically implantable permanent 6mm stent that allows draining from the anterior chamber into the subconjunctiva. [9]
Problem
The definition of glaucoma has evolved to include more than just increased IOP. Glaucoma is defined as "the final common pathway of a group of diseases with decreased retinal ganglion cell sensitivity and function, retinal ganglion cell death, optic nerve axonal loss and concurrent cup enlargement, incremental reduction in visual fields, and blindness. Most of these diseases either result in or are associated with increased IOP in their mid to late stages." Although this definition is complicated, it highlights the fact that the understanding of the various clinical manifestations of glaucoma is expanding. Despite additional risk factors having been identified, such as a decrease in retrobulbar ocular blood flow, reduction in the IOP remains the only modifiable risk factor proven to slow the progression of glaucoma.
Epidemiology
Glaucoma is typically associated with aging, and its frequency increases as people reach their sixth decade of life. The disease is estimated to affect 1% to 2% of the US population and an estimated 64 million people worldwide in 2014. [10, 11, 12, 13] Global prevalence for people between ages 40 to 80 is more than 3%. [10] People of African descent are more likely to have POAG than those of European descent. [14, 10] Prevalence of POAG is higher in men than women. [14]
 Eye that has undergone a trabeculectomy. The aqueous humor drains more easily after a small section of the trabecular meshwork was removed.
Eye that has undergone a trabeculectomy. The aqueous humor drains more easily after a small section of the trabecular meshwork was removed.
Etiology
Primary open angle glaucoma (POAG) is characterized by an elevated IOP at some point during the course of the disease with an open anterior chamber angle and a characteristic optic nerve and/or visual field change in the absence of concurrent ocular disease. Primary open-angle glaucoma, the most common form of glaucoma, is characterized by a chronic insidious onset.
The exact etiology of POAG is not known, as glaucoma appears to be a multifactorial disease. POAG has been associated with increased intraocular pressure, decreased retrobulbar blood flow, hypertension, gender, race, and many other factors, providing further evidence that this disease is likely an overlap of many different elements. Additional population subsets within the spectrum of open angle glaucoma have recently been defined. For instance, normal tension glaucoma is defined as a progressive optic neuropathy, but with an IOP measuring less than 21 mm Hg. Furthermore, ocular hypertension has been defined as an IOP greater than 21 mm Hg, but with a normal anterior chamber angle and no optic nerve or visual field changes. Alternatively, individuals with primary glaucoma may have narrow-angle glaucoma, in which the iridocorneal angle progressively closes over time, resulting in obstruction of aqueous humor outflow.
 Iridocorneal angle. Structures of the angle are well recognized stereoscopically. From top to bottom: posterior surface of the cornea, Schwalbe line, nonpigmented trabecular meshwork, pigmented trabecular meshwork, scleral spur, ciliary body band, and iris root.
Iridocorneal angle. Structures of the angle are well recognized stereoscopically. From top to bottom: posterior surface of the cornea, Schwalbe line, nonpigmented trabecular meshwork, pigmented trabecular meshwork, scleral spur, ciliary body band, and iris root.
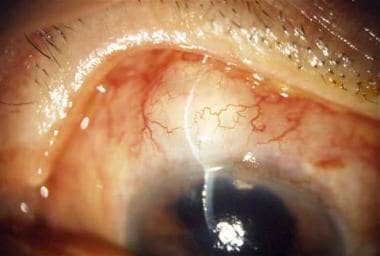
Secondary glaucoma is characterized by elevated IOP associated with concurrent ocular disease. A few examples of secondary glaucoma causes include pigment dispersion and pseudoexfoliation syndrome, uveitis with the formation of peripheral anterior synechiae in the iridocorneal angle, intraocular hemorrhage with trabecular meshwork obstruction, intraocular neoplasia, and lens displacement, as is shown in the image below.
 Secondary glaucoma is characterized by elevated intraocular pressure associated with concurrent ocular disease, such as lens dislocation.
Secondary glaucoma is characterized by elevated intraocular pressure associated with concurrent ocular disease, such as lens dislocation.
Pathophysiology
Glaucoma is a group of ocular diseases characterized by progressive damage to the optic nerve. The disease is usually chronic and can lead to visual field loss and blindness. Cupping of the optic disc and loss of retinal nerve fibers indicate damage to the optic nerve. The loss of nerve fibers results in a corresponding patterns of visual field loss. Elevated IOP is a major risk factor for the development of POAG.
The rate of aqueous humor production, the resistance in outflow routes, and episcleral venous pressure regulate IOP. Aqueous humor, produced by the ciliary processes, flows into the anterior chamber and leaves the eye by two pathways: trabecular (conventional) outflow and uveoscleral outflow. Most aqueous humor exits the eye through the trabecular meshwork, the Schlemm canal, and the episcleral veins; the remaining 10% to 20% exits via the uveoscleral route, passing between the ciliary muscle bundles.
In a healthy eye, the production and outflow of aqueous humor maintain an IOP in the range of 10 to 21 mm Hg. Pressure usually is similar in both eyes and shows diurnal variations. In most patients with glaucoma, the resistance to aqueous humor outflow increases, resulting in elevated IOP.
Glaucoma is categorized as open angle or closed angle. Open-angle glaucoma, the most common type, includes primary glaucoma, capsular glaucoma, pigmentary glaucoma, normal-tension glaucoma, and some types of congenital glaucoma and secondary glaucoma. Closed-angle glaucoma results from partial or total obstruction of the anterior chamber angle, which blocks the trabecular network.
In primary open-angle glaucoma, elevated IOP likely results from low-grade obstruction of aqueous humor outflow in the trabecular meshwork. Elevated IOP, in turn, can produce mechanical and/or ischemic damage to the optic nerve. The onset is usually insidious and asymptomatic, with changes in the visual field not generally noticeable until late in the disease, when cupping of the optic disc can be seen.
Patients with normal-tension glaucoma have pathologic optic disc cupping and visual field loss but normal IOP (< 21 mm Hg). In these patients, reducing IOP significantly delays glaucomatous changes. Normal tension glaucoma is thought to be related to ocular blood flow, as it has been associated with migraines, nocturnal hypotension, and a reduction in ocular perfusion pressure.
Patients with ocular hypertension have elevated IOP (>21 mm Hg) but a normal visual field and optic disc. The relationship between ocular hypertension and glaucoma is not clear, but patients with ocular hypertension should be regularly monitored for visual field loss or changes in the optic nerve.
Presentation
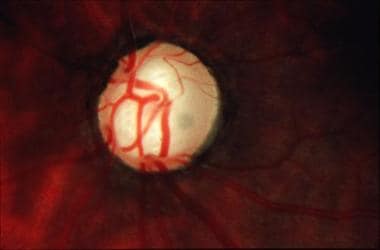
Patients with open-angle glaucoma are usually asymptomatic and it usually is found on routine eye exam. Eyes with early glaucoma may have subtle structural and functional optic nerve changes, but it is very important to identify patients with glaucoma early in order to initiate therapy to limit injury to the nerve fibers. Clinical signs of late glaucoma often reveal extensive cupping of the optic disc due to the retinal ganglion cell injury and loss (as demonstrated in the image below). Patients may have elevated IOP or reduced peripheral visual field acuity. Patients in acute angle closure glaucoma usually complain of decreased vision, pain, and halos around lights. Exam will be notable for conjunctival injection, corneal edema, mid-dilated pupil and elevated IOP.

Indications
Surgical intervention is indicated in the following circumstances:
-
Patients with uncontrolled intraocular pressure (IOP) on maximum tolerated medical therapy in the presence of significant changes in the optic disc and/or visual field
-
Noncompliance with topical medial therapy
-
Advanced optic nerve or visual field changes found early in the presentation
Critical factors for surgical interventions are individually based and depend on the amount of functional vision loss, the rapidity of visual deterioration, and the patient's life expectancy.
The primary objectives of trabeculectomy are to maintain useful vision and to avoid further glaucomatous damage by lowering the IOP. [1]
Relevant Anatomy
The two primary types of disease, open-angle glaucoma and angle-closure glaucoma, are classified according to the anatomy of the anterior chamber angle and are shown in the image below.
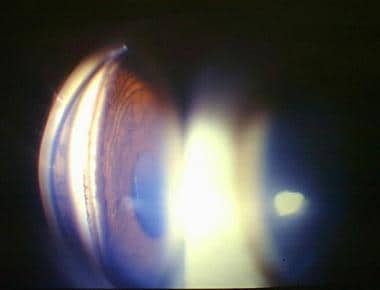 Open-angle glaucoma and angle-closure glaucoma are classified according to the anatomy of the anterior chamber angle, as determined on visual inspection of the angle by using a special lens. This image is seen through a 3-mirror gonioscope.
Open-angle glaucoma and angle-closure glaucoma are classified according to the anatomy of the anterior chamber angle, as determined on visual inspection of the angle by using a special lens. This image is seen through a 3-mirror gonioscope.
This classification is determined on visual inspection of the angle by using a special lens, called a goniolens, on the slit lamp biomicroscope. Patients with open-angle glaucoma can be treated with glaucoma-filtering surgery.
Contraindications
Contraindications to glaucoma-filtering surgery include the following:
-
Intraocular neoplasia
-
Hyphema
-
Anterior lens luxation
-
Elevated episcleral venous pressure
-
Blind eye
-
Neovascular glaucoma
-
Active iritis
-
Conjunctival scaring
-
Thinned sclera as seen in necrotizing scleritis
Prognosis
It is estimated that the lifetime risk for bilateral blindness in patients with POAG approximates 8% in patients of African descent and 4% in European descent. The best predictor of blindness is based on the baseline visual field at presentation. [15]
The Early Manifest Glaucoma Trials (EMGT) revealed that reduction of the IOP early in the course of the disease reduced the progression of visual field loss. The Collaborative Initial Glaucoma Treatment Study Essentials (CIGTS) evaluated if newly diagnosed OAG was better treated with medication or immediate filtering surgery. They reported that patients had a similar quality of life, but patients who underwent surgery reported more local ocular symptoms. At 9 years, both treatment groups were found to have similar visual field loss. The surgery group had quicker loss likely secondary to the higher risk for cataracts. At 8 years, the mean deviation (MD) worsened by more than 3 dB in 21.3% in the surgery group and 25.5% in the medication group. They also report that, in patients with worse baseline visual field, there was less progression when trabeculectomy was performed first. Topical medications were found to decrease IOP approximately 38%, whereas surgery was found to decrease IOP approximately 46%. [16]
-
Traditional glaucoma-filtering surgery.
-
Iridocorneal angle. Structures of the angle are well recognized stereoscopically. From top to bottom: posterior surface of the cornea, Schwalbe line, nonpigmented trabecular meshwork, pigmented trabecular meshwork, scleral spur, ciliary body band, and iris root.
-
Secondary glaucoma is characterized by elevated intraocular pressure associated with concurrent ocular disease, such as lens dislocation.
-
Reduced peripheral acuity in early glaucoma.
-
Cupping of the optic disc in late glaucoma.
-
Open-angle glaucoma and angle-closure glaucoma are classified according to the anatomy of the anterior chamber angle, as determined on visual inspection of the angle by using a special lens. This image is seen through a 3-mirror gonioscope.
-
Pupillary block angle-closure glaucoma. Courtesy of the Ocular Imaging Center, New York Eye and Ear Infirmary.
-
Hyphema. Deposition of RBCs in the anterior chamber.
-
Eye that has undergone a trabeculectomy. The aqueous humor drains more easily after a small section of the trabecular meshwork was removed.
-
Trabeculectomy. Courtesy of Gina Urwin, Urwin Medical Illustrations.
Tables
| GSS Stage | Definition | Humphrey MD score |
|---|---|---|
| 0 | Ocular hypertension/earliest glaucoma - No or minimal defect | MD > 0.00 dB |
| 1 | Early defect | MD ≥ −6.00 dB |
| 2 | Moderate defect | MD of −6.01 to −12.00 dB |
| 3 | Advanced defect | MD of −12.01 to −20.00 dB |
| 4 | Severe defect | MD < −20.00 dB |
| 5 | End stage - Poor visual acuity/inability to perform visual field testing due to severe vision loss | No measurable visual field |






