Background
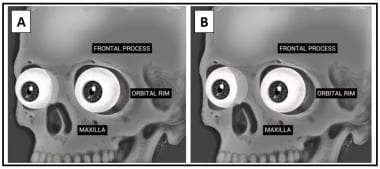
Enophthalmos is the posterior displacement of the globe into the orbital cavity. [1] The anterior projection of the eye is most commonly measured relative to the outer edge of the orbit, but also may be assessed relative to the frontal and maxillary prominences, or the contralateral eye. An image of the eyes and their relative position to the skull is below. In panel A, the eyes are at roughly equivalent positions with the equator of the eye at the lateral orbital rim. In panel B, the right eye is posteriorly displaced in a relatively enophthalmic position.
Pathophysiology
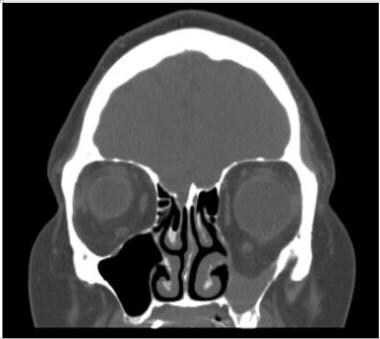
Primary enophthalmos indicates a congenital or developmental etiology. Some degree of facial asymmetry is common, but congenital relative enophthalmos or ocular retrusion may occur with in utero maldevelopment (eg, plagiocephaly, microphthalmos). Secondary enophthalmos is due to an acquired change in volumetric relationship between the rigid bone cavity, the orbit, and its contents (predominantly the orbital fat, the extraocular muscles, and the eye). Expansion of the orbital cavity without change in the volume of orbital contents (ie, a blow-out fracture) leads to enophthalmos. [2] An example of a blow-out fracture with post-traumatic enophthalmos is shown in the image below. The arrow points to the downward displacement of the orbital floor bone into the blood-filled maxillary sinus.
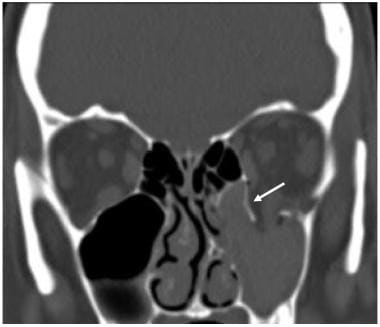
Spontaneous enlargement of the orbit may occur in silent sinus syndrome, as depicted in the figure below, where a negative pressure develops within the maxillary sinus, thinning the orbital floor and drawing it downward. [3] The maxillary sinus is filled with mucoid material, not blood, in silent sinus syndrome.
Alternatively, scarring contracture of the orbital fat and extraocular muscles may decrease soft tissue volume, making the orbital cavity less full and causing enophthalmos. Several disorders may cause this, including metastatic sclerosing or scirrhous breast carcinoma or linear scleroderma. [4, 5] Other potential causes for enophthalmos include age-related fat atrophy or HIV-related lipodystrophy, although these usually present with bilaterally symmetric enophthalmos.
Epidemiology
Frequency
United States
Enophthalmos is common.
International
Same as in the United States.
Mortality/Morbidity
Enophthalmos greater than 2 mm relative to the contralateral eye creates an observable cosmetic deformity. Depending on the etiology, other significant morbidity may be associated.
Age
This condition occurs at all ages, but different ages have different common etiologies.
Prognosis
The prognosis of enophthalmos is directly related to both the underlying cause and the degree of deformity.
Most causes of enophthalmos are treatable, and surgical correction is most frequently excellent following outpatient surgery.
Patient Education
Perhaps the single most important advice to give a patient until the workup of suspected new-onset enophthalmos has been completed is not to blow their nose and to sneeze with their mouth open.
One of the most common causes of enophthalmos is orbital fracture. Barometric changes in the nasopharynx (wind velocity may exceed 200 mph during a sneeze) can force air into the orbit. The loose orbital fat may then fall back into place covering the bone defect, acting as a ball valve, trapping the air, and creating an acute orbital compartment syndrome with blinding potential.
Other causes of bone loss between the orbit and the sinuses (most notably varix and silent sinus syndrome) also may be affected by dramatic barometric pressure changes.
-
Eye and orbit.
-
Conventional frontal tomograph of a blow-out fracture.
-
Relative enophthalmos.
-
Enophthalmos.
-
Coronal computed tomograph of silent sinus syndrome.
-
Worms' eye view showing left enophthalmos.