Background
In 1883, Marcus Gunn described a 15-year-old girl with a peculiar type of congenital ptosis that included an associated winking motion of the affected eyelid on the movement of the jaw. [1, 2] This synkinetic jaw-winking phenomenon now bears his name. See the image below.

Patients with Marcus Gunn jaw-winking syndrome have variable degrees of blepharoptosis in the resting, primary position. Although Marcus Gunn jaw-winking syndrome is usually unilateral, it can present bilaterally in rare cases. [1, 3, 4]
The wink reflex consists of a momentary upper eyelid retraction or elevation to an equal or higher level than the normal fellow eyelid upon stimulation of the ipsilateral pterygoid muscle. This response is followed by a rapid return to a lower position. The amplitude of the wink tends to be worse in downgaze. This rapid, abnormal motion of the eyelid can be the most disturbing aspect of the jaw-winking syndrome.
The wink phenomenon may be elicited by opening the mouth, thrusting the jaw to the contralateral side, jaw protrusion, chewing, smiling, or sucking. [1, 5, 6, 7, 8] This wink phenomenon is often discovered early, as the infant is bottle-feeding or breastfeeding. See the image below.
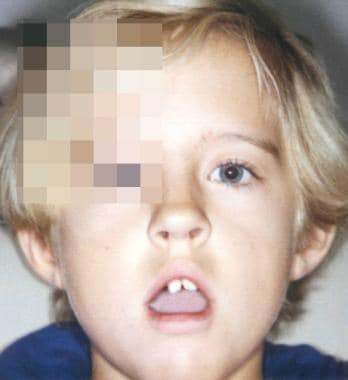 Marcus Gunn jaw-winking with left upper eyelid retraction on opening of the mouth.
Marcus Gunn jaw-winking with left upper eyelid retraction on opening of the mouth.
Jaw-winking ptosis is almost always sporadic, but familial cases with an irregular autosomal dominant inheritance pattern have been reported. [9]
Pathophysiology
Marcus Gunn jaw-winking is thought to be a form of synkinetic ptosis. An aberrant connection appears to exist between the motor branches of the trigeminal nerve (CN V3) innervating the external pterygoid muscle and the fibers of the superior division of the oculomotor nerve (CN III) that innervate the levator superioris muscle of the upper eyelid. [1, 10, 11, 12, 13]
Electromyographic studies demonstrate this synkinetic innervation by showing simultaneous contraction of the external pterygoid and levator muscle. In rare cases, synkinesis may be present between the internal pterygoid and levator muscles. In these cases, the eyelid elevates on closing the mouth and clenching the teeth. [14]
A few authors have speculated that the jaw-winking is not due to a new aberrant pathway, but rather the disinhibition of preexisting phylogenetically more primitive mechanisms. [15] This is thought to explain why individuals who are not affected will often open their mouths while attempting to widely open their eyes to place eye drops or to apply makeup.
Since jaw-winking ptosis is believed by most to be due to abnormal innervation of the levator muscle and not secondary to myopathic changes, it is not surprising that most histopathologic studies have revealed normal striated muscle.
One study found variable degrees of fibrosis within the affected levator muscle and to a lesser degree in the muscle of the normal, nonptotic eyelid. [16, 17]
Epidemiology
Frequency
United States
Approximately 50% of blepharoptosis cases are congenital. Incidence of Marcus Gunn jaw-winking syndrome among this population is approximately 5%. [5]
Mortality/Morbidity
Marcus Gunn jaw-winking syndrome is associated with strabismus in 50-60% of cases. [5] Superior rectus palsy is found in 25% of cases, and double elevator palsy is found in another 25% of cases. [5] In double elevator palsy, a deficiency in elevation of the globe occurs in all positions of gaze, secondary to an apparent weakness of the superior rectus and inferior oblique muscles. On rare occasions, horizontal strabismus in the absence of a vertical motility disturbance may occur.
Incidence of anisometropia among patients with Marcus Gunn jaw-winking syndrome is reported to be 5-25%. [5] Anisometropia exists when a refractive difference between the 2 eyes of 1.25 diopters of sphere or 1 diopter of cylinder is present.
Amblyopia occurs in 30-60% of patients with Marcus Gunn jaw-winking syndrome and almost always is secondary to strabismus or anisometropia, and, only rarely, is due to occlusion by a ptotic eyelid. [5] Amblyopia usually is defined as a decrease in vision of 2 or more lines on the Snellen chart.
Race
No known racial predilection exists.
Sex
Early reports showed jaw-winking ptosis to be more prevalent in females than in males; however, larger case series have shown an equal prevalence among males and females. [5, 18]
Age
Marcus Gunn jaw-winking syndrome usually is evident at birth. The winking phenomenon often is first noted by the parents when the infant is feeding.
It has been suggested, and older patients often claim, that the jaw-winking improves over time; however, it has not proven to be true on objective evaluation. More likely, patients stop seeking care as they get older, or they learn to compensate for and mask the wink response. [5, 10, 18, 19]
Likewise, the degree of ptosis may be underestimated with the patient able to adjust the height with varying jaw positions. This is referred to by some as "habitual" ptosis. [20]
Prognosis
Satisfactory results usually are achieved by a medical and surgical approach to managing Marcus Gunn jaw-winking ptosis.
Patient Education
Discuss the following with the patient or the parents:
-
Connection between jaw movement and abnormal movement of the eyelid
-
Importance of treating amblyopia or strabismus prior to any surgical repair of ptosis
-
Various surgical approaches, to include possible benefits of bilateral eyelid surgery
-
Congenital left upper eyelid ptosis.
-
Marcus Gunn jaw-winking with left upper eyelid retraction on opening of the mouth.






