Background
Schnyder corneal dystrophy (SCD), also called Schnyder crystalline corneal dystrophy (SCCD), is a rare autosomal-dominant stromal dystrophy that is characterized by bilateral corneal opacification, resulting from an abnormal accumulation of cholesterol and lipid. The causative gene for this disease is UBIAD1, which is present on 1p36. The gene is involved in cholesterol metabolism.
Please refer to the image below depicting the natural history of Schnyder corneal dystrophy specific to age.
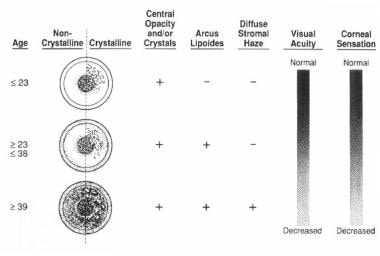 The natural history of Schnyder dystrophy with age. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
The natural history of Schnyder dystrophy with age. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
Van Went and Wibaut first described crystalline dystrophy in the Dutch literature in 1924, and it was delineated further by Schnyder in the Swiss literature in 1929. [1, 2]
While the incidence in the general population is unknown, the world's largest pedigree (>200 patients with Schnyder corneal dystrophy) has a Swede-Finn heritage and has been traced to the southwest coast of Finland on the Bay of Bothnia. However, the dystrophy has been reported in other ethnicities and in all racial groups.
Pathophysiology
The pathogenesis remains unknown, but it is postulated to result from a localized defect of lipid metabolism. It has been demonstrated in affected corneas versus normal corneas that the cholesterol content increases 10-fold and the phospholipid content increases 5-fold. Immunohistochemical analysis has revealed the preferential deposition of apolipoprotein components of high-density lipoprotein (HDL), that is, apoA I, apoA II, and apoC, but not of low-density lipoprotein (LDL), that is, apoB. This finding suggests an abnormal metabolism of HDL in the cornea with Schnyder corneal dystrophy.
The discovery of the causative gene, UBIAD1 (UbiA prenyltransferase domain-containing protein-1), will be the link to further understanding of this disease. The gene produces a protein that contains a prenyltransferase domain that could play a role in cholesterol metabolism. In addition, UBIAD1 interacts with the C-terminal portion of apolipoprotein E (apoE), which is known to help mediate cholesterol removal from the cells. Further research will determine whether the excess cholesterol results from increased cholesterol production or decreased removal.
Epidemiology
Frequency
United States
The dystrophy has been reported in the United States, although the incidence in the general population is unknown.
International
While the incidence is unknown, the dystrophy has been reported in eastern and western Europe, Taiwan, Japan, and Turkey.
Mortality/Morbidity
A long-term study of 34 families over a period of 18 years revealed that most morbidity derives from progressive corneal clouding, leading to glare and decreased vision in daylight. [3]
In this study, mean Snellen uncorrected visual acuity (UCVA) was between 20/25 and 20/30 in patients younger than 40 years and between 20/30 and 20/40 in patients aged 40 years or older. Scotopic vision remained relatively good until later in life, when corneal opacification increased.
Studies of those affected reveal that 54% of patients aged 50 years and older and 77% of patients aged 70 years and older had corneal transplant surgery. Although study numbers are small, there is no evidence of increased mortality from cardiovascular disease in Schnyder corneal dystrophy. Of note, however, 71% of patients who had corneal transplant surgery reported the use of cholesterol-lowering agents. This was not statistically different from those patients who had not undergone corneal transplant surgery.
Race
Schnyder corneal dystrophy can occur in whites, Asians, and African Americans.
Sex
Although rare sporadic cases have been reported, Schnyder corneal dystrophy is primarily an autosomal dominant disease, affecting both sexes with equal probability.
Age
The disease may appear as early as the first decade of life and slowly progresses with age. However, a diagnosis may be delayed until the fourth decade in patients with corneal opacification without crystalline deposits.
Prognosis
Results of clinical examination have shown that crystalline deposits are present in only 51% of patients with Schnyder corneal dystrophy. [4]
While Schnyder corneal dystrophy may be diagnosed easily during the first decade of life, the diagnosis Schnyder corneal dystrophy sine crystals is more challenging and is reported to be delayed up to the fourth decade of life. Some patients have been documented to have unilateral crystalline deposition. Why the corneal cholesterol forms crystals in some patients, but not in others, remains unclear.
Contrary to prior reports, many patients with Schnyder corneal dystrophy eventually require corneal transplantation because of glare and decreased vision in daylight.
Patient Education
For excellent patient education resources, visit eMedicineHealth's Cholesterol Center. Also, see eMedicineHealth's patient education articles High Cholesterol, Cholesterol FAQs, and Atorvastatin (Lipitor).
-
A 22-year-old woman with circular corneal opacity best seen in retroillumination. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
-
A 20-year-old woman with ringlike deposition of anterior stromal cholesterol crystals. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
-
A 37-year-old man with central disclike opacity, affecting the entire stromal thickness, anterior stromal cholesterol crystals, and peripheral arcus lipoides. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
-
A 78-year-old woman with dense arcus lipoides in the corneal periphery, sparing the corneal scleral limbus. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.
-
The natural history of Schnyder dystrophy with age. Weiss JS: Schnyder's dystrophy of the cornea: a Swede-Finn connection. Cornea 1992; 11(2): 93-101.

