Background
A macular hole is a defect of the foveal retina involving its full thickness from the internal limiting membrane (ILM) to the outer segment of the photoreceptor layer.
See the image below.
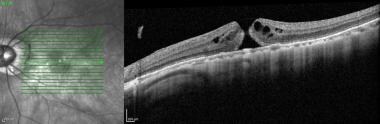
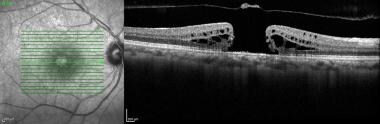
 SD-OCT Image of a Stage 3 full thickness macular hole similar to the fundus image. Note the cuff of subretinal fluid, cystic changes to the retina and RPE changes in the base of the hole.
SD-OCT Image of a Stage 3 full thickness macular hole similar to the fundus image. Note the cuff of subretinal fluid, cystic changes to the retina and RPE changes in the base of the hole.
A macular hole first was described by Knapp in 1869 in a patient who sustained blunt trauma to the eye. Subsequent case reports and series pointed to antecedent episodes of ocular trauma such that the two were customarily linked to each other. However, throughout this century, ophthalmologists increasingly have recognized that this condition more commonly occurs in atraumatic settings and have differentiated these macular holes from trauma-induced holes by describing them as idiopathic full-thickness macular holes. In fact, case series as far back as the 1970s reported that more than 80% of macular holes are idiopathic and that only less than 10% have associated history of trauma to the eye.
Pathophysiology
The causes underlying trauma-related macular holes and idiopathic macular holes are understandably divergent.
Trauma-related macular holes are suspected to be related to the transmission of concussive force in a contrecoup manner, which results in the immediate rupture of the macula at its thinnest point. Patients who underwent successful repair of a rhegmatogenous retinal detachment were also found to infrequently develop macular holes (< 1% incidence). The underlying pathophysiology for formation of these holes is not well understood, though epiretinal membrane formation, foveal photoreceptor atrophy, and hydraulic forces may play a role.
While the vitreous was suspected to be involved in the causation of idiopathic macular holes by Lister in 1924, Johnson and Gass, in 1988, first described a classification system that focused on anteroposterior and tangential vitreous traction on the fovea as a primary underlying cause for idiopathic macular holes. [1, 2] Shrinkage of prefoveal cortical vitreous with persistent adherence of vitreous to the foveal region results in the causative traction.
Gass macular hole stages are described below.
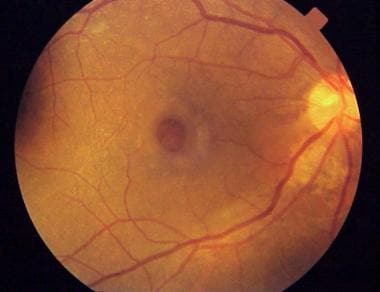
Stage 1a (foveal detachment; macular cyst): Tangential vitreous traction results in the elevation of the fovea marked by increased clinical prominence of xanthophyll pigment. This stage is occasionally referred to as the yellow dot stage and can also be seen in cases of central serous chorioretinopathy, cystoid macular edema, and solar retinopathy as depicted below.
 Fundus photograph of a stage 1a macular hole with characteristic yellow spot at the center of the fovea.
Fundus photograph of a stage 1a macular hole with characteristic yellow spot at the center of the fovea.
Stage 1b: As the foveal retina elevates to the level of the perifoveal, the yellow dot of xanthophyll pigment changes to a donut shaped yellow ring. Persistent traction on the fovea leads to dehiscence of deeper retinal layers at the umbo.
Stage 2: This is the first stage when a full-thickness break in the retina exists. It is defined as a full-thickness macular hole less than 400 µm in size. The full-thickness defect may appear eccentric, and there may be a pseudo-operculum at this stage if there has been spontaneous vitreofoveolar separation. These opercula have been examined and found to be vitreous condensation and glial proliferation without harboring any retinal tissue.
 SD-OCT image of a Stage 2 full thickness macular hole. Note the eccentric location of the full thickness retinal defect on the infra-red scout image.
SD-OCT image of a Stage 2 full thickness macular hole. Note the eccentric location of the full thickness retinal defect on the infra-red scout image.
Stage 3: A full-thickness macular hole in the retina exists. It is greater than 400 µm in size and is still with partial vitreomacular adhesion/traction.
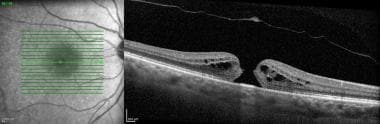
 SD-OCT image of a large macular hole. Note its size on the infra-red scout image in relation to the optic nerve. The posterior cortical hyaloid face is visible along with a pseudo-operculum. Depending on whether the vitreous is also detached from the optic nerve determines whether this particular macular hole is a stage 3 or stage 4 full thickness macular hole.
SD-OCT image of a large macular hole. Note its size on the infra-red scout image in relation to the optic nerve. The posterior cortical hyaloid face is visible along with a pseudo-operculum. Depending on whether the vitreous is also detached from the optic nerve determines whether this particular macular hole is a stage 3 or stage 4 full thickness macular hole.
Stage 4: A full-thickness macular hole exists in the presence of a complete separation of the vitreous from the macula and the optic disc. There is evidence, however, that, even in the presence of an apparent posterior vitreous detachment, a thin shell of residual cortical vitreous may still remain and contribute to the macular hole.
The advent of ocular coherence tomography (OCT) has provided in vivo structural support to hypotheses focused on vitreous traction underlying idiopathic macular holes. The OCT has allowed careful evaluation of the vitreoretinal interface demonstrating persistent adhesion on the fovea resulting in oblique traction on the fovea even with a partial posterior vitreous detachment. The persistent traction on the fovea prior to anatomic changes to the fovea has been referred to as Stage 0. This clinical appearance may resolve without progression in 40-50% of patients. [3]
Visual dysfunction in patients with macular hole is directly related to the absence of retinal tissue in the fovea. However, visual dysfunction may seem out of proportion to the size of the macular hole and potentially may also be related to the presence of a cuff of subretinal fluid with associated photoreceptor atrophy.
See Causes.
Epidemiology
Frequency
United States
The overall prevalence is approximately 3.3 cases in 1000 in those persons older than 55 years. Peak incidence of idiopathic macular hole development is in the seventh decade of life, and women typically are affected more than men. Reasons for this, at best, are speculative at this point. Some epidemiologic risk factors, such as cardiovascular disease, hypertension, and a history of hysterectomy, have been reported by other studies. However, none of these have been proven to have any significant association with macular hole formation.
International
The prevalence rate of macular hole in India is a reported 0.17%, with a mean age of 67 years.
The Beijing Eye Study found the rate of macular holes to be 1.6 out of 1000 elderly Chinese, with a strong female predilection.
Mortality/Morbidity
The natural history of a macular hole varies based on its current clinical stage. It has been reported that around 50% of stage 0 and stage 1 macular holes may resolve both in the anatomic changes and the symptoms produced. Stage 2 holes progress and worsen in most cases to stage 3 or stage 4, resulting in worsening vision. Best estimates for the incidence of development of an idiopathic full-thickness macular hole in the fellow eye are approximately 12%. In rare instances (0-10%), a full-thickness macular hole may spontaneously close with resultant good vision.
Race
There is no racial predilection reported, though prevalence rates for the epidemiologic studies in India and China are consistent with reported data.
Sex
Women typically are affected more than men.
Age
Peak incidence is in the seventh decade of life.
Prognosis
In 1994, Wendel reported a series of 235 consecutive eyes undergoing repair of macular holes. [4] In this series, 93% of patients were successfully managed with only a single operation; 60% patients experienced 4+ lines of visual improvement; and 84% patients experienced 2+ lines of improvement. [4] Within this group, 58% of patients achieved 20/40 or better final visual acuity. [4]
Multiple other studies cite similar success rates, though vision recovery may be protracted and also further delayed by onset of cataract formation. Use of ILM peeling may further increase the rate of single operation success, though it may potentially slow or affect final vision recovery. See Controversies surrounding the surgical repair of macular holes.
OCT imaging preoperatively and postoperatively has provided additional prognostic data for visual recovery following macular hole surgery. Factors on OCT predictive of good visual acuity macular hole surgical outcome are as follows:
-
Size of macular hole (minimum diameter < 311 µm)
-
Traction on macular hole edges as defined by various parameters (eg, macular hole height)
-
Development of a normal photoreceptor inner segment and outer segment junction, which can occur as early as 1 month postoperatively but typically by 6 months postoperatively as shown in the images below.
-
The presence of an epiretinal membrane on OCT may be a poor prognostic sign for closure of a full thickness macular hole{ref82
-
The height of the external limiting membrane (ELM) on OCT has also been found to be predictive of postoperative visual acuity. Patients with small macular holes and a low ELM height on OCT have better visual recovery following surgery. [86]
 SD-OCT Image of a stage 2 full thickness macular hole. Note the size of the macular hole, as well as the last of residual traction on the edges of the hole and the height of the external limiting membrane. No epiretinal membrane is observed on the surface of the retina. This eye should have a good prognosis for postoperative visual acuity.
SD-OCT Image of a stage 2 full thickness macular hole. Note the size of the macular hole, as well as the last of residual traction on the edges of the hole and the height of the external limiting membrane. No epiretinal membrane is observed on the surface of the retina. This eye should have a good prognosis for postoperative visual acuity.
OCT images are also used to study changes following surgical repair of macular holes. There are patterns of gliotic proliferation following surgery that can effect the best final visual acuity as well as the pace of recovery of visual acuity. [85]
While surgery for macular holes is considered elective, it is important for the patient to consider prognostically that there is potentially a risk for the fellow eye to develop a macular hole as well (12%).
Patient Education
Older individuals should be educated on the necessity of a yearly eye examination since early symptoms of a macular hole can easily go undetected by the patient.
-
Full-thickness macular hole showing a surrounding cuff of subretinal fluid.
-
Full-thickness macular hole with typical yellowish granular deposits on the retinal pigment epithelium.
-
Fluorescein angiogram showing a central window defect.
-
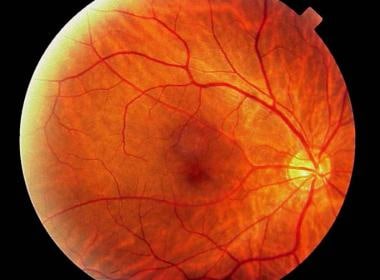
Preoperative fundus photograph of a macular hole.
-
Fundus photograph of the same patient as in the image above at 6 months postoperatively. Note the increased media opacity caused by cataractous changes of the lens.
-
Fundus photograph of a stage 1a macular hole with characteristic yellow spot at the center of the fovea.
-
SD-OCT Image of a Stage 3 full thickness macular hole similar to the fundus image. Note the cuff of subretinal fluid, cystic changes to the retina and RPE changes in the base of the hole.
-
SD-OCT image of a Stage 2 full thickness macular hole. Note the eccentric location of the full thickness retinal defect on the infra-red scout image.
-
SD-OCT image of a large macular hole. Note its size on the infra-red scout image in relation to the optic nerve. The posterior cortical hyaloid face is visible along with a pseudo-operculum. Depending on whether the vitreous is also detached from the optic nerve determines whether this particular macular hole is a stage 3 or stage 4 full thickness macular hole.
-
SD-OCT image of a patient with a myopic full thickness macular hole. On this OCT image, note the foveal schisms and the presence of an epiretinal membrane.
-
SD-OCT image of a large chronic macular hole. Note the retinal pigment epithelial atrophy both on the infrared scout image as well as by increased transmission on the OCT image on the corresponding margins of the hole. Also, an epiretinal membrane is present on the surface of the retina surrounding the macular hole.
-
SD-OCT Image of a stage 2 full thickness macular hole. Note the size of the macular hole, as well as the last of residual traction on the edges of the hole and the height of the external limiting membrane. No epiretinal membrane is observed on the surface of the retina. This eye should have a good prognosis for postoperative visual acuity.