Background
Wyburn-Mason syndrome (WMS), also known as Bonnet-Dechaume-Blanc syndrome or retinoencephalofacial angiomatosis, is a rare nonhereditary congenital phakomatosis characterized by arteriovenous malformations (AVMs) of the retina, brain, and, in some cases, facial skin. Wyburn-Mason syndrome is usually unilateral and often asymptomatic. [1]
An example of a retinal AVM is shown in the image below.
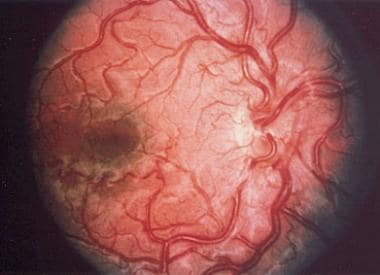 The dilated and abnormal retinal vasculature characteristic of a retinal arteriovenous malformation.
The dilated and abnormal retinal vasculature characteristic of a retinal arteriovenous malformation.
Although these combined vascular abnormalities were recognized prior to the reports of Bonnet (1937) [2] and Wyburn-Mason (1943), [3] this syndrome is most frequently referred to as Wyburn-Mason syndrome (WMS) to honor the initial author of the classic case series. Wyburn-Mason syndrome is a congenital, nonhereditary, sporadic disorder without sexual or racial predilection. [1] Other vascular malformations may be present elsewhere in the body, including facial skin. In contrast to other phakomatoses, Wyburn-Mason syndrome does not commonly cause cutaneous manifestations. However, WMS manifests as subtle facial nevi with angiomas around the trigeminal territory.
Pathophysiology
Although the exact etiology and risk factors associated with Wyburn-Mason syndrome are unknown, studies have suggested a role for genetic factors in the pathogenesis of retinal AVMs. Vascular dysgenesis of the embryological anterior plexus occurs early in the gestational period, characterized by variable alterations in capillary and arteriolar networks. Small AVMs may be asymptomatic and subtle, with only minor alterations within the capillary system. Alternatively, the classic large "bag-of-worms" racemose AVM lesions are characterized by direct artery-to-vein communication, without interposing capillary or arteriolar elements causing high blood flow. [1] The timing of the insult determines the embryonic tissue that is affected.
Epidemiology
Frequency
United States
Wyburn-Mason syndrome is rare, and the precise incidence and prevalence are poorly defined. To date, fewer than 100 cases have been reported in the literature.
International
The worldwide incidence of Wyburn-Mason syndrome is also rare.
Race
Wyburn-Mason syndrome has no reported racial predilection, and there is no familial form of the syndrome.
Sex
Wyburn-Mason syndrome has no sexual predilection.
Age
Wyburn-Mason syndrome is a congenital disorder. Larger retinal AVMs that cause visual or neurologic impairment are generally diagnosed earlier in life, whereas smaller AVMs may remain asymptomatic and may not be diagnosed until later in life.
-
The dilated and abnormal retinal vasculature characteristic of a retinal arteriovenous malformation.




