Background
Barratta first described aniridia (Greek for absence of the iris) in 1818. Congenital aniridia is a rare, bilateral, panophthalmic disorder in which iris hypoplasia or aplasia is the most striking feature.
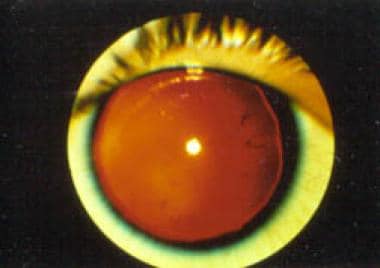 Aniridia. Note the almost complete absence of the iris.
Aniridia. Note the almost complete absence of the iris.
Aniridia also has corneal, lens, optic nerve, and retinal manifestations. Foveal and optic nerve hypoplasia often are present, causing reduced visual acuity and congenital sensory nystagmus. Progressive worsening of vision may occur later in life as a result of cataracts, glaucoma, and corneal opacification, all of which can contribute to ambylopia. [1] Lifelong follow-up with an ophthalmologist is essential for detection and management of these progressive eye pathologies.
Pathophysiology
Aniridia may be familial or sporadic. In most cases, familial aniridia is caused by a mutation in the PAX6 gene on chromosome 11, leading to involvement of most eye structures. [2]
Approximately 85% of cases are familial (designated AN1) with autosomal dominant inheritance with complete penetrance but variable expressivity. These familial cases usually have isolated ocular involvement.
The 15% of cases that are sporadic have a deletion or mutation on the short arm of chromosome 11. The same deletion is responsible for the development of Wilms tumor (nephroblastoma).
The exact pathogenesis of aniridia is unknown. After early reports of ocular colobomas in patients with aniridia, some authors proposed that it is a colobomatous disorder. Others attributed it to a failure of mesodermal development with involvement of the rim of the optic cup, causing iris hypoplasia. Still others advocated the neuroectodermal theory, which links the presence of retinal anomalies and iris muscular hypoplasia to a developmental failure of neuroectoderm.
Epidemiology
Frequency
United States
Aniridia is a very rare disorder, and limited studies exist regarding its prevalence. A single population-based study in Michigan estimated aniridia affects approximately 1 per 61,000 newborns. [3]
International
A 2001 study from Denmark reported the point prevalence rate as high as 1 per 40,000 live births. [4] Age-specific prevalence of aniridia in Sweden has been reported to be 1:70,000 and, in Norway, 1:76,000. [5]
Mortality/Morbidity
Aniridia itself is not lethal. A homozygous mutation of the aniridia gene may be lethal, although limited data exists. [6] The morbidity of aniridia is significant due to decreased vision and nystagmus. Congenital reduced vision is further complicated with progressive eye diseases such as cataracts, glaucoma, and corneal opacifications.
Race
No racial predilection has been described.
Sex
There is no significant sex predilection described in the literature. In Sweden and Norway, the reported pooled male/female ratio in patients with aniridia is 0.94. [5]
Age
Aniridia is a congenital inherited disorder apparent at birth, and it is not known to be acquired later in life. All diagnosed patients without a family history of aniridia should undergo a systemic work-up.
Patient Education
Educating patients and parents about aniridia and associated progressive ocular conditions is necessary so timely treatment can be given. Since the condition often has an autosomal dominant transmission, genetic counseling, and family ophthalmic evaluations should be performed.
-
Aniridia. Note the almost complete absence of the iris.






