Practice Essentials
Lyme disease, the most common vector-borne illness in the United States, is a multisystem illness usually caused by infection with the spirochete Borrelia burgdorferi (see the image below) and the body's immune response to the infection. [1, 2] The disease is transmitted to humans via tick bites, from infected ticks of the genus Ixodes.
 Lyme disease. The bacterium Borrelia burgdorferi (darkfield microscopy technique, 400X; courtesy of the US Centers for Disease Control and Prevention).
Lyme disease. The bacterium Borrelia burgdorferi (darkfield microscopy technique, 400X; courtesy of the US Centers for Disease Control and Prevention).
See Lyme Disease and 4 Emerging Tick-Borne Illnesses, a Critical Images slideshow, to help identify and treat several tick-borne conditions.
Signs and symptoms
Signs and symptoms of Lyme disease vary by disease stage. Physical findings in patients with early disease are as follows:
-
Flulike illness - Fever, chills, malaise, myalgias, arthralgia, headache
-
Tender local adenopathy (local, not diffuse)
-
Erythema migrans (EM) - Rash
Physical findings in patients with early disseminated disease are as follows:
-
EM (single or multiple lesions)
-
Headache
-
Fever
-
Tender adenopathy (regional or generalized)
-
Conjunctivitis (uncommon, never prominent)
-
Carditis (usually manifests as heart block)
-
Meningismus as a sign of aseptic meningitis
-
Cranioneuropathy, especially cranial nerve VII and Bell palsy (peripheral seventh nerve palsy with decreased unilateral function, including the forehead)
In patients with late disease, the typical physical finding is arthritis. Arthritis is located mostly in large joints, especially the knee. Warmth, swelling from effusion, and limited range of motion help distinguish arthritis from simple arthralgia.
See Presentation for more detail.
Diagnosis
In endemic areas, patients with probable erythema migrans and a recent source of tick exposure should be started on treatment without blood tests. For serologic testing, the CDC recommends the following two-tier procedure [3] :
-
Step 1: Enzyme immunoassay (EIA) or immunofluorescence assay (IFA) - Total Lyme titer or IgG and IgM titers
-
Step 2: Western blot testing
Western blot testing is performed only if step 1 test results are positive or equivocal. If signs and symptoms have been present for 30 days or less, both IgM and IgG Western blot testing are performed; if signs and symptoms have been present for more than 30 days, only IgG Western blot testing is performed.
Since Western blot testing is necessary to exclude false-positive EIA or IFA results, but unnecessary if the initial test is negative, Lyme titers should always be ordered with a reflex confirmatory test. Most commercial laboratories will perform both IgG and IgM Western blots.
In July 2019, the US Food & Drug Administration (FDA) approved the use of concurrent or sequential EIA testing for diagnosis of Lyme disease. The FDA approved the new indication on the basis of data from clinical studies showing that this alternative approach, referred to as a modified two-tier test, is as accurate as testing with EIA or IFA plus Western blot. [4]
If the patient has been in Europe, where different strains of Borrelia are more common, a C6 peptide ELISA is a more accurate confirmatory test than the Western blots, which have been developed to B burgdorferi, which is the most common strain found in the United States. The C6 peptide is less expensive than the Western blots and is as sensitive and specific for B burgdorferi; it is a reasonable alternative for the Western blots, but has not replaced it as the usual confirmatory test in the United States.
Other studies that may be used are as follows:
-
Joint aspiration - To exclude other causes of effusion (eg, septic arthritis, gout, pseudogout)
-
CSF analysis - In patients with meningitis
-
ECG - To identify Lyme carditis
See Workup for more detail.
Management
With appropriate antibiotic treatment, most patients with early-stage Lyme disease recover rapidly and completely. Antibiotic selection, route of administration, and duration of therapy for Lyme disease are guided by the patient’s clinical manifestations and stage of disease, as well as the presence of any concomitant medical conditions or allergies.
Treatment of Lyme disease is as follows:
-
Adult patients with early localized or early disseminated Lyme disease associated with erythema migrans: Doxycycline, amoxicillin, or cefuroxime axetil
-
Children under 8 years and pregnant or nursing women with early localized or early disseminated Lyme disease: Amoxicillin or cefuroxime axetil
-
Neurologic Lyme disease: IV penicillin, ceftriaxone, or cefotaxime; oral doxycycline, when not contraindicated, in patients with Lyme-associated meningitis, facial nerve palsy, or radiculitis
Treatment of Lyme arthritis is as follows:
-
Oral antibiotics for 28 days
-
Re-treatment with oral antibiotics for mild residual joint swelling
-
Re-treatment with IV antibiotics for refractory cases
-
Oral antibiotics for another month in patients with positive PCR of synovial fluid
-
NSAIDs in patients with negative PCR, supplemented if necessary with hydroxychloroquine
-
Consideration of arthroscopic synovectomy in patients unresponsive to symptomatic therapy
Lyme carditis may be treated with either oral or parenteral antibiotic therapy for 14 days (range, 14-21 days). Hospitalization and continuous monitoring, with consideration for temporary pacing, are advisable for patients with any of the following:
-
Associated symptoms (eg, syncope, dyspnea, or chest pain)
-
Second-degree or third-degree AV block
-
First-degree heart block with prolongation of the PR interval to more than 300 milliseconds (the degree of block may fluctuate and worsen very rapidly in such patients)
See Treatment and Medication for more detail.
Background
Lyme disease is a multisystem illness usually caused by infection with the spirochete Borrelia burgdorferi and the body's immune response to the infection. [2] The disease is transmitted to humans via tick bites, from infected ticks of the genus Ixodes.
Lyme disease is the most common vector-borne illness in the United States. More than 30,000 cases of Lyme disease are reported to the US Centers for Disease Control and Prevention each year; in 2015, it was the sixth most common nationally notifiable disease. [5] Lyme disease is also endemic in other parts of North America, as well as in Europe and Asia. See Epidemiology.
Because only approximately 25-30% of US patients with early Lyme disease recall the tick bite, the clinician must direct the history toward the possibility of a tick bite. Epidemiologic context is extremely important. The probability of a tick bite—and thus, the likelihood of contracting Lyme disease—is highest in persons who spend time outdoors (particularly in wooded, brushy, or grassy habitats) in a geographically endemic area, especially from May through November.
Early localized Lyme disease refers to isolated erythema migrans, the characteristic skin rash of Lyme disease, and to an undifferentiated febrile illness. This stage occurs 1-30 days after the tick bite.
Early disseminated Lyme disease usually develops 3-10 weeks after inoculation. Musculoskeletal and neurologic symptoms are the most common; less common are symptoms from cardiac disturbances; and ocular manifestation, most often conjunctivitis.
Late or chronic Lyme disease refers to manifestations that occur months to years after the initial infection, sometimes after a period of latency. Signs and symptoms of chronic Lyme disease are primarily rheumatologic and neurologic.
See Presentation.
In endemic areas, patients with probable erythema migrans and a recent source of tick exposure should be started on treatment without blood tests. In the absence of erythema migrans, serologic testing is used. The US Centers for Disease Control and Prevention (CDC) recommends a two-step testing procedure. The first step typically consists of a screening enzyme immunoassay (EIA) or enzyme-linked immunosorbent assay (ELISA); if results are positive or equivocal, a Western immunoblot test is performed to confirm the results. [3]
Other tests and procedures (eg, electrocardiogram, cerebrospinal fluid analysis) depend on the presentation. See Workup.
Antibiotic selection, route of administration, and duration of therapy for Lyme disease are guided by the patient's clinical manifestations and stage of disease, as well as the presence of any concomitant medical conditions or allergies. First-line agents include doxycycline, penicillins, cefuroxime, and ceftriaxone; however, doxycycline is contraindicated in patients younger than 8 years and in pregnant and breastfeedingf women. See Treatment and Medication.
Medical societies have created Lyme disease guidelines. The Infectious Diseases Society of America (IDSA), American Academy of Neurology, and American College of Rheumatology have published a joint consensus guideline for the prevention, diagnosis, and treatment of Lyme disease. [6]
Clinical Image Atlas: View clinical images on the features, causes, epidemiology, diagnosis, and treatment of Lyme disease.
Historical background
The original descriptions of the dermatologic manifestations of Lyme disease date back to 1883 in Europe, when a German physician, Alfred Buchwald, described what is now termed acrodermatitis chronica atrophicans (ACA). In 1912, the Swedish dermatologist Arvid Afzelius described the rash, then called erythema chronicum migrans, which currently is referred to simply as erythema migrans (EM).
In the 1920s, Garin and Bujadoux described a patient with meningoencephalitis, painful sensory radiculitis, and erythema migrans following a tick bite, which they attributed to a spirochetal infection. By the mid 1930s, neurologic manifestations associated with Ixodes ticks (also known as deer ticks) were recognized and were known as tick-borne meningoencephalitis. In the 1940s, Bannwarth described several cases of chronic lymphocytic meningitis and polyradiculoneuritis, some of which were accompanied by erythematous skin lesions.
In the United States, Lyme disease was not recognized until the early 1970s, when a statistically improbable cluster of pediatric arthritis cases occurred in the region around Lyme, Connecticut. This outbreak was investigated by Allen Steere, MD, and others from Yale and stimulated intense clinical and epidemiologic research that led to the discovery of the causative agent and its ecology and an expanding geographic range and list of clinical manifestations.
The recognition that the patients in the United States had erythema migrans and the initial antibiotic responsiveness of the cutaneous manifestations that had been described in the 1950s in the European literature was confirmed. [7] This led to the recognition that Lyme arthritis was one manifestation of the same tick-borne condition known in Europe.
After Willy Burgdorfer, MD, discovered a borrelial organism in Ixodes ticks, it was recovered from patients with clinical Lyme disease, confirming Borrelia as the causative agent. This led to the development of antibody tests for the disease. Different strains of Borrelia are recognized, which probably explains why the clinical manifestations of Lyme disease are different between the United States and Europe.
Lyme disease has become common in the United States from Maryland to Maine and in Wisconsin and Minnesota, with a smaller focus in northern California. The emergence of Lyme disease is probably due to the explosion of deer and tick populations with the reforestation of the northeastern United States and the subsequent contact between ticks and humans as people move into deer habitats. The pathogen itself is not new; B burgdorferi has been found in tick specimens collected in the 1940s on eastern Long Island, New York.
The spirochete Borrelia burgdorferi is introduced into the skin with a bite from an infected Ixodes tick. In the northeastern and upper midwestern United States, Ixodes scapularis is the vector. In other parts of the country and world, other Ixodes species serve that function. Other ticks (eg, Amblyomma americanum) and insects can carry B burgdorferi, but Ixodes tick bites are thought to cause the vast majority of cases.
In the southern and mid-central United States, a Lymelike illness has been reported; the vector appears to be A americanum, and the causative organism or organisms is likely to be a related spirochete. [8, 9] One such organism, named Borrelia lonestarii, has been cultured in a single case.
Borrelia burgdorferi infectious cycle
The infectious cycle of B burgdorferi involves colonization, infection of Ixodes ticks, and then transmission to broad a range of mammalian hosts, including humans. Variation in environmental and host conditions promotes different gene expression and changes in the composition of the membrane proteins of the spirochete. This adaptation is a critical step in the pathogenesis and transmission of Lyme disease.
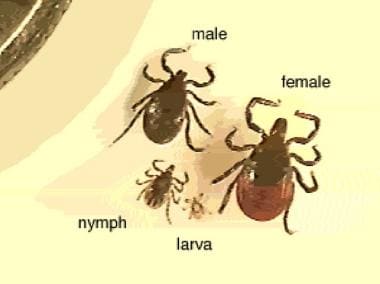
The Ixodes tick progresses through four stages of development: egg, larva, nymph, and adult (see the following image for examples of each stage). Only larvae, nymphs, and adult female ticks require blood meals, and only ticks in the nymphal and adult stages can transmit B burgdorferi.
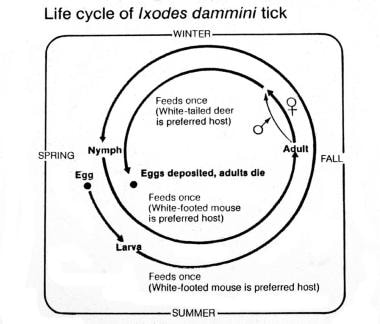
The life cycle of Ixodes ticks spans 2 years (see the image below). The adult lays eggs in the spring, and the larvae emerge in the summer. The larvae feed once, in late summer, on any of a wide variety of small animals (eg, the white-footed mouse) . The following spring, the larvae emerge as nymphs. Nymphs feed once, in the spring and summer. The white-footed mouse is the preferred feeding source of nymphs, but other animals apparently suffice. Nymphs molt into adults the following fall and feed once on a larger animal, with the white-tailed deer being the preferred host.
Ticks can acquire B burgdorferi from feeding on an infected animal host during any of the three life-cycle stages. Unless the tick has fed on an infected host before feeding on a person, infection cannot result from that tick bite. Even if a tick that has previously fed on an infected animal and then feeds on an infected animal, the animal may not acquire the infection. Mice do not appear to develop Lyme disease, but they do carry the bacteria. They may be considered infested rather than infected. Deer also are incompetent hosts for Borrelia.
Ticks carry B burgdorferi organisms in their midgut. The bacteria are introduced into the skin by a bite from an infected tick, and disease is transmitted to humans as the spirochete is translocated from the gut to the salivary glands and then to the person at the site of the bite.
The risk of Lyme disease is highest during the time of the year when Ixodes ticks in the nymphal stage are seeking a blood meal. Although the prevalence of B burgdorferi infection in adult ticks is twice that of nymph ticks, nymphs are responsible for 90% of human disease transmissions because of the great abundance of nymphs; the increase in human outdoor activity in the summer (the peak feeding season of nymphs); and the small size of nymphs, which makes them less likely to be detected and removed before disease transmission occurs.
The risk of transmission of B burgdorferi from an infected tick to a human depends on the length of exposure. It takes hours for the tick to attach fully, and experimental studies have indicated that in most cases, nymphs must feed 36-48 hours and adults 48-72 hours to transmit B burgdorferi, since the blood meal has to trigger the reproduction of the Borrelia to a large enough number to be infective .
Pathogenesis
Once the spirochete is in the skin, one of three events may occur:
-
The spirochete may be overwhelmed and eliminated by host defense mechanisms
-
The spirochete may remain viable and localized in the skin, where it produces erythema migrans (EM), the characteristic skin lesion of Lyme disease
-
Within days to weeks, the spirochete may disseminate through the lymphatics or blood,
After entering the circulation, the organism shows a distinct tropism for the skin, heart, central nervous system (CNS), joints, and eyes. Any part of the body can be affected, however; spirochetes have also been demonstrated histologically in bone marrow, the spleen, lymph nodes, the liver, testes, and the placenta during early hematogenous dissemination.
The clinical manifestations of Lyme disease generally follow three stages of disease progression: early localized, early disseminated, and chronic disseminated (see also Clinical Presentation). All are potentially curable with antibiotic therapy. The infection progresses to disseminated disease in approximately 50% of untreated patients. Only a few genotypes of B burgdorferi appear to be responsible for the large majority of cases of disseminated disease. [10]
Stage 1 disease
Stage 1 is also known as primary or early localized infection. It generally occurs within 30 days of the tick bite. Most patients present with a characteristic expanding rash (erythema migrans) at the site of the tick bite 7-14 days after the tick is removed. Nonspecific symptoms may include the following:
-
Fatigue
-
Myalgias
-
Arthralgias
-
Headache
-
Fever
-
Chills
-
Neck stiffness
Stage 2 disease
Stage 2 is also known as early disseminated disease. It generally occurs weeks to months after the bite. Musculoskeletal and neurologic symptoms are the most common; less common symptoms are cardiac and dermatologic.
B burgdorferi spreads throughout the body and produces symptoms by direct invasion (eg, erythema migrans), particularly in the early stages of the disease. Because growing B burgdorferi in culture is difficult, confirming that the organism is actually present in a specific organ that may be involved in Lyme disease is also difficult. The inflammatory response to B burgdorferi in the skin is probably the explanation for multiple lesions of erythema migrans, as almost all patients with multiple lesions are seropositive, regardless of duration. [11]
Antibodies against spirochetal protein membrane epitopes have been shown to cross-react with neural and connective tissues. This molecular mimicry possibly generates an autoimmune inflammatory reaction. The pathophysiology of early versus late manifestations of the disease is similar to that seen with syphilis.
Early studies showed that B burgdorferi or its DNA can be detected in the bloodstream of roughly 10% of patients with isolated erythema migrans and no systemic symptoms. In addition, early in the course of disease and while erythema migrans still is present, spirochetal DNA has been detected in cerebrospinal fluid (CSF), indicating early CNS penetration. This can occur even in the absence of neurologic symptoms.
Importantly, one study found that if large-volume cultures (9 mL of plasma) were performed in early-presenting patients with erythema migrans, 93 (43.7%) of 213 had spirochetemia. Some of these patients had only isolated erythema migrans and no systemic symptoms. [8]
Stage 3 disease
Stage 3 or chronic Lyme disease happens months to years after infection, which sometimes involves a period of latency. Musculoskeletal (mainly joints) and neurologic systems are most commonly affected.
B burgdorferi induces an immune response that may lead to symptoms in various organs, with little evidence of bacterial invasion. Studies of Lyme arthritis have shown that the arthritis is associated with certain immunologic factors, including the production of proinflammatory cytokines and the formation of immune complexes; and genetic factors, such as carriage of human leukocyte antigen (HLA)–DR4 and HLA-DR2.
Patients with HLA-DR4 or HLA-DR2 and antibodies to OspA and OspB (outer surface protein A) proteins in their joint fluid may be more susceptible to long-term arthritis than persons without these characteristics. The presence of these genes is presumably related to the development of autoimmunity in the joint, which can lead to persistent inflammation even after the spirochete is apparently eradicated.
Animal studies have suggested a primary role of astrocytes and microglial cells in the pathogenesis of neuroborreliosis. Interleukin 6 (IL-6) production by astrocytes and subsequent oligodendrocyte apoptosis have been proposed as mechanisms of cell injury. [12]
A study of maladaptive immune responses in 79 patients with Lyme neuroborreliosis who were followed for 1 year reported that serum levels of interferon-α (IFN-α) were elevated at study entry and remained elevated in patients whose symptoms persisted despite antibiotic therapy. The highest IFN-α levels corresponded with severe disease. In contrast, levels of 19 other cytokines and chemokines associated with innate and adaptive T-cell and B-cell immune responses were initially elevated, particularly in cerebrospinal fluid, but decreased dramatically with effective antibiotic therapy. [13]
The organism also can persist in the skin for very long periods. Experimentally, the spirochete can penetrate human fibroblasts and live intracellularly, even when the extracellular medium contains ceftriaxone at concentrations well above bactericidal levels. Although intracellular organisms have never been demonstrated in vivo, this may be a mechanism by which the organism eludes host defenses.
Etiology
Lyme disease is usually caused by infection with the spirochete Borrelia burgdorferi (see the image below) . The complete genome of B burgdorferi was described in 1998.
Lyme disease. The bacterium Borrelia burgdorferi (darkfield microscopy technique, 400X; courtesy of the US Centers for Disease Control and Prevention).
The species Borrelia burgdorferi sensu lato has three well-characterized groups, as follows:
-
B burgdorferi sensu stricto
-
B garinii
-
B afzelii
B burgdorferi sensu stricto is a broad category of closely related but genetically distinct genospecies that constitutes most North American isolates and is found in Europe as well. B afzelii is found mainly in Europe. B garinii is found epredominantly in Eurasia, but has also been isolated in eastern North America. [14]
These subspecies are associated with different clinical presentations, probably due to genomic variation. Infection with B burgdorferi sensu stricto has a particular predilection to affect joints. In European patients with erythema migrans, B afzelii can be isolated from about 80% of lesions and B garinii from 15%. [15] B afzelii often infects the skin only but may persist in that site, causing various cutaneous manifestations including acrodermatitis chronica atrophicans.
B garinii has some neurotropism and is the isolate that accounts for most cases of lymphocytic meningoradiculitis (Bannwarth syndrome) and white matter encephalitis, which is rare in North America. However, this organism can also cause all the various cutaneous manifestations of Lyme disease.
Other strains, which may be sufficiently different in their genetic structure to be considered separate strains, exist; however, most of these are nonpathogenic to humans. This is an area of active research.
Borrelia miyamotoi, which causes a febrile illness and is transmitted by ixodid ticks, was discovered in 1994 in Japan and has since been reported in North America, Europe, and Asia. B miyamotoi infection is widespread in Ixodes ticks in the northeastern, northern Midwestern, and far western United States and in Canada. Common clinical manifestations of B miyamotoi infection are fever, fatigue, headache, chills, myalgia, arthralgia, and nausea. B miyamotoi infection responds to the same antibiotics used for Lyme disease. [16]
In 2016, Mayo Clinic researchers reported the discovery of a novel species of bacteria, provisionally named Borrelia mayonii, isolated in six patients in the upper Midwest of the US with suspected Lyme disease. Clinically, disease from B mayonii is similar to that from B burgdorferi, except that B mayonii is associated with nausea and vomiting, diffuse rashes, and unusually high spirochetemia. Polymerase chain reaction (PCR) testing targeting the oppA1 gene of B burgdorferi sensu lato proved useful in diagnosis. [17]
B burgdorferi is transmitted by ixodid tick species. In the northeastern and upper midwestern United States, Ixodes scapularis (sometimes termed Ixodes dammini) is the vector. In the northwestern United States, Ixodes pacificus is the vector. In other parts of the world, other Ixodes ticks serve this function. Other tick species (eg, Amblyomma americanum) and insects can carry B burgdorferi, but the vast majority of cases are believed to be caused by bites by Ixodes ticks. See the images below.
 Lyme disease. This patient's erythema migrans rash demonstrates several key features of the rash, including size, location, and presence of a central punctum, which can be seen right at the lateral margin of the inferior gluteal fold. Note that the color is uniform; this pattern probably is more common than the classic pattern of central clearing. On history, this patient was found to live in an endemic area for ticks and to pull ticks off her dog daily.
Lyme disease. This patient's erythema migrans rash demonstrates several key features of the rash, including size, location, and presence of a central punctum, which can be seen right at the lateral margin of the inferior gluteal fold. Note that the color is uniform; this pattern probably is more common than the classic pattern of central clearing. On history, this patient was found to live in an endemic area for ticks and to pull ticks off her dog daily.
 Amblyomma americanum is the tick vector for monocytic ehrlichiosis and tularemia. An adult and a nymphal form are shown (common match shown for size comparison). Image by Darlyne Murawski; reproduced with permission.
Amblyomma americanum is the tick vector for monocytic ehrlichiosis and tularemia. An adult and a nymphal form are shown (common match shown for size comparison). Image by Darlyne Murawski; reproduced with permission.
Note that in the southern and mid-central United States, a Lyme-like disease has been reported for which the vector appears to be A americanum. B burgdorferi has not been isolated from the southern patients, although a closely related spirochete is suspected to be involved. Although some cases from the southern United States are documented with this new spirochete, called Borrelia lonestarii, no organism can be isolated in the vast majority of cases of erythema migrans in this geographic area. [9, 18]
Epidemiology
Lyme disease is endemic in North America, Europe, and Asia, and the distribution of the vectors directly affects the incidence of the disease. Ixodes scapularis is the principal vector found in the Northeast and Central United States and Canada, whereas Ixodes pacificus is more common on the Pacific coast. Ixodes ricinus is the principal vector in Europe. The vector in Asia is the taiga tick, Ixodes persulcatus.
United States statistics
Lyme disease is the most common vector-borne illness in the United States. Over 30,000 cases of Lyme disease are reported each year. [5] In 2018, a total of 33,666 of Lyme disease—23,558 confirmed and 10,108 probable— were reported to the US Centers for Disease Control and Prevention (CDC), a 21% decrease from 2017 figures. [5] Lyme disease led the list of a record number of tickborne disease cases that state and local health departments reported to the CDC In 2016 through 2019. [19]
From 2008 (when the national surveillance case definition was revised to include probable cases) to 2012, the incidence ranged from 9.86-12.71 cases per 100,000 population in the US. [20] In 2015, Lyme disease was the sixth most common nationally notifiable disease. [5]
The CDC tracks cases of Lyme disease by using strict surveillance criteria (not designed for diagnosis of individual cases). The incidence has been increasing over time; this is not simply a result of increased recognition, because in states that perform active surveillance, true incidence and geographic range have increased. The likely causes of this increase are expansion of deer herds and the expanded range of the vector.
Epidemiologic data suggest that the actual incidence of Lyme disease could be as much as 10 times higher than the CDC data indicate. This probably is a result of a restrictive case definition from the CDC, inevitable misdiagnosis, and the fact that physicians tend to underreport reportable diseases of all kinds. The CDC estimates that as many as 476,000 people may get Lyme disease each year in the United States. [5]
The risk of Lyme disease follows a general geographic pattern, with concentrations in the Northeast, mid-Atlantic, and upper Midwest. In 2018, 3-year average incidence of confirmed cases was high (ie, at least 10 per 100,000) in the following states [5] :
-
Connecticut – 36.2
-
Delaware – 45.7
-
Maine – 92
-
Maryland – 18.6
-
Massachusetts – 2.3
-
Minnesota – 21.9
-
New Hampshire – 63.8
-
New Jersey – 36.6
-
New York – 14.5
-
Pennsylvania – 68.1
-
Rhode Island – 56.4
-
Vermont – 79.1
-
Virginia – 10.9
-
West Virginia – 24.9
-
Wisconsin – 25.4
Washington, DC was also a high-incidence area, at 8.9 cases per 100,000 population. Note that Massachusetts uses a surveillance method that relies primarily on laboratory reports, and information on most Lyme disease cases occurring in that state is not sent to the CDC. [5]
In addition, infected ticks have also been found in states neighboring those, as well as in some areas of northern California, Oregon, and Washington. [5] In 2019, confirmed cases of Lyme disease were reported from every US state except Oklahoma and Hawaii. [21]
The map below shows the county of residence for each reported case of Lyme disease in 2018. This does not indicate where each case of Lyme disease was acquired.
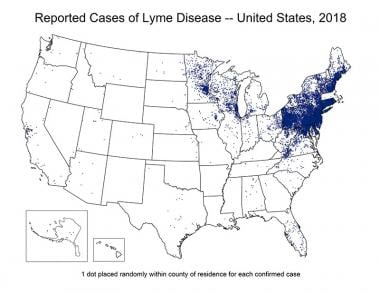 Lyme disease in the United States is concentrated heavily in the northeast and upper Midwest; it does not occur nationwide. Dots on the map indicate the infected person's county of residence, not the place where they were infected. Courtesy of the US Centers for Disease Control and Prevention (CDC).
Lyme disease in the United States is concentrated heavily in the northeast and upper Midwest; it does not occur nationwide. Dots on the map indicate the infected person's county of residence, not the place where they were infected. Courtesy of the US Centers for Disease Control and Prevention (CDC).
In the states where Lyme disease is most common, the average incidence is 39.5 cases per 100,000 persons. [5] Within these states, incidence can be quite variable from county to county and even neighborhood to neighborhood. [22]
Lyme disease has a seasonal influence that reflects the feeding pattern of the Ixodes tick and human outdoor activity. Infection occurs most often between May and November, with a peak incidence in June through August; 75% of cases occur during the summer months.
International statistics
Lyme disease exists throughout much of the world, including Canada, Europe, and Asia. Occasionally, cases are reported in more tropical locales, and Lyme disease may exist in Australia.
In Asia, Borrelia burgdorferi infection has been reported in countries including China, Korea, Japan, Indonesia, Nepal, and eastern Turkey. In Europe, Lyme disease is primarily caused by B afzelii and B garinii.
A systematic review of Lyme disease borreliosis in Europe from 2005 to 2020 found that the highest incidences (> 100 cases per 100,000 population per year [PPY]) were reported in Belgium, Finland, the Netherlands, and Switzerland. Incidences of 20-40/100,000 PPY were reported in the Czech Republic, Germany, Poland, and Scotland, and incidences of < 20/100,000 PPY were reported in Belarus, Croatia, Denmark, France, Ireland, Portugal, Russia, Slovakia, Sweden, and the United Kingdom. However, local high incidences were also noted in areas of countries with low overall incidence. [23]
Racial differences in incidence
Lyme disease is reported primarily in whites, although it occurs in individuals of all races. No genetic explanation is known for this; the disparity most likely stems from social or environmental factors (ie, a higher exposure rate to ticks in whites than in members of other races) and possibly to the fact that erythema migrans is more difficult to diagnose in dark-skinned individuals.
Sexual and age-related differences in incidence
No strong preponderance of Lyme disease is noted in either sex. Reports from Europe indicate that, among children, the rate of Lyme disease is slightly higher in boys than in girls aged 5-19 years, [24] but, in adults over 30 years of age, the disease is more common in women than in men. In the United States from 1992-2006, 53.1% of reported Lyme disease cases occurred in males. [22]
Age distribution in Lyme disease is bimodal: the first peak is in children aged 5-14 years and the second in adults aged 45-54 years. [25] In general, this pattern is related to increased levels of outdoor activity and environmental exposure in these age groups rather than any intrinsic difference in susceptibility.
Prognosis
The prognosis for patients with Lyme disease is generally excellent when they are treated early with appropriate antibiotic regimens. However, recurrent infection is possible if the patient is again bitten by an infected tick; these infections are usually due to a different strain of the local Borrelia. [26]
Patients, especially adults, who receive late treatment or initial treatment with antibiotics other than doxycycline or amoxicillin may develop chronic musculoskeletal symptoms and difficulties with memory, concentration, and fatigue. These symptoms can be debilitating and hard to eradicate.
Some patients develop chronic arthritis that is driven by immunopathogenic mechanisms and not active infection. This condition is more prevalent among individuals with HLA-DR2, HLA-DR3, or HLA-DR4 allotypes. The arthritis is resistant to antibiotic treatment but typically responds to symptomatic treatment and shows eventual resolution. [27]
Cardiac involvement in Lyme disease is rarely chronic. However, patients with third-degree heart block often require a temporary pacemaker insertion and, on rare occasions, a permanent pacemaker insertion.
Lyme disease appears to rarely be fatal. Many of the fatal cases reported have been in patients co-infected with other tick-borne pathogens such as Ehrlichia species and B microti, and in Europe, tick-borne encephalitis. A US Centers of Disease Control and Prevention (CDC) study of death records from 1999-2003 found that only one of 114 total records listing Lyme disease as an underlying or multiple cause of death was consistent with clinical manifestations of Lyme disease. [28] .
Extremely rare cases of neonatal death or stillbirth have been reported after pregnancies complicated by untreated or inadequately treated symptomatic maternal Lyme borreliosis. Subsequent findings from CDC studies suggest that congenital infection with B burgdorferi is unlikely and that it is not directly responsible for adverse fetal outcomes.
Post-treatment Lyme disease syndrome
Lingering symptoms, which may persist for more than 6 months, affect 10-20% of patients who receive recommended treatment for Lyme disease. [5] Common complaints include cognitive disturbances, fatigue, joint or muscle pain, headaches, hearing loss, vertigo, mood disturbances, paresthesias, and difficulty sleeping. This condition is often termed chronic Lyme disease, but is more appropriately called post-treatment Lyme disease syndrome (PTLDS).
No evidence suggests that prolonged antibiotic therapy is effective for PTLDS. Almost all patients recover with time, but recovery may take more than 6 months in some cases. [5]
In one study, many patients who had been diagnosed with Lyme disease 1-11 years previously reported increased symptoms, difficulties with typical daily activities, or both. However, the frequencies of these reports were similar to those in age-matched controls without Lyme disease. [29]
Another study found no difference in musculoskeletal abnormalities, neurologic abnormalities, or neurocognitive performance between control patients and Lyme disease patients examined a mean of 6 years after infection. However, patients with previous Lyme disease had more joint pain and memory impairment, and had poorer functional status due to pain. [30]
Patient Education
Clinicians should educate parents and children who live in endemic areas about the risk of Lyme disease. Education and awareness are the best means of preventing Lyme disease. Anticipatory guidance should focus on prevention measures and post–tick exposure counseling on watching for symptoms and signs of Lyme disease. Personal strategies for preventing Lyme disease fall into two categories: personal habit modification (eg, avoiding ticks/tick habitats, inspecting clothing and pets, using repellents) and prophylaxis.
Educate patients with early stages of Lyme disease about symptoms that can develop later. Development of these symptoms necessitates re-examination and may indicate treatment failure or incorrect diagnosis. Advise patients receiving doxycycline that this antibiotic can cause severe cutaneous photosensitivity. Caution patients to use sunblock with a sun protection factor (SPF) of at least 30 and to wear wide-brimmed hats for further protection.
Patients who have had Lyme disease should be advised that antibodies induced by the infection are not protective against further exposures to Borrelia burgdorferi; one episode of erythema migrans does not always confer immunity to the next. Consequently, preventive strategies remain important for these patients.
For patient education information, see Lyme Disease. Additional information can be obtained from the American Lyme Disease Foundation, Inc.
Avoidance
Educate patients regarding ticks and tick avoidance. Backyard patios, decks, and grassy areas that are mowed regularly are unlikely to have ticks present. This may be because of the lack of cover for mice from owls and other raptors that prey on mice. In addition, these areas do not provide moisture, which ticks need. The areas around ornamental plantings and gardens are more hospitable for mice and ticks.
The highest concentration of ticks is found in wooded areas. Staying to centers of trails and applying repellents to the skin or to clothing helps avoid contact with ticks (see Repellents, below). In addition, wearing long-sleeved shirts and tucking long pants into socks and long hair under a hat when outdoors is recommended. Wearing light-colored clothing improves the odds of seeing ticks on clothing before they can attach.
Inspection and tick removal
Because recommendations for avoidance are not always practical, particularly for children and during the summer, daily close inspection for ticks should be performed each time one has been outdoors. Parents of children in endemic areas must be vigilant to check for ticks—especially the nymphs, because of their smaller size (approximately that of a poppy seed)—from the spring to the fall. Checking inside skin folds, behind ears, the umbilicus, groin, axilla, hairline, and scalp must be routine. If one tick is found, search thoroughly for others.
See the image below for a tick removal diagram and instructions.
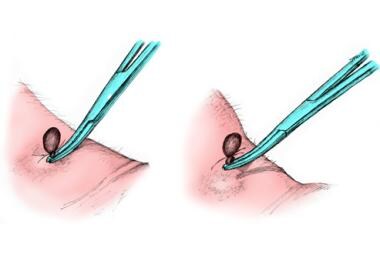 To remove a tick, use fine-tipped forceps and wear gloves. Grasp the tick as close to the skin surface as possible, including the mouth parts, and pull upward with steady, even traction. Do not twist or jerk the tick because this may cause the mouth parts to break off and remain in the skin; however, note that the mouth parts themselves are not infectious. When removing, wear gloves to avoid possible infection.
To remove a tick, use fine-tipped forceps and wear gloves. Grasp the tick as close to the skin surface as possible, including the mouth parts, and pull upward with steady, even traction. Do not twist or jerk the tick because this may cause the mouth parts to break off and remain in the skin; however, note that the mouth parts themselves are not infectious. When removing, wear gloves to avoid possible infection.
While these instructions may represent the optimal method for removing the tick, it is more important to remove it promptly than to delay removing it while obtaining forceps or gloves.
A common misperception is that pressing a hot match to the tick or trying to smother it with petroleum jelly, gasoline, nail polish, or other noxious substances is beneficial. This only prolongs exposure time and may cause the tick to eject infectious organisms into the body. Finally, do not squeeze, crush, or puncture the body of the tick because its fluids (saliva, hemolymph, gut contents) may contain infectious organisms.
Once the tick is removed, wash the bite area with soap and water or with an antiseptic to destroy any contaminating microorganisms. Additionally, the person who removed the tick should wash his or her hands. The removed tick should be submitted for species identification. [6]
The likelihood of infection is related to the duration of tick attachment. [31] Infection is much less likely, but not impossible, when ticks have been attached for less than 24 hours. The degree of engorgement of the tick (see the following image) can be used as an indicator for tick attachment duration.

Repellents
Lyme disease guidelines recommend the following repellents for prevention of tick bites [6] :
-
N,N-diethyl-meta-toluamide (DEET)
-
Picaridin
-
Ethyl-3-(N-n-butyl-N-acetyl)aminopropionate (IR3535)
-
Oil of lemon eucalyptus
-
P-menthane-3,8-diol (PMD)
-
2-Undecanone
-
Permethrin
Products containing DEET, picaridin, IR3535, and oil of lemon eucalyptus are available in numerous over-the-counter skin preparations as sprays or lotions. Permethrin is an acaricide that can be applied to clothing and is used in conjunction with chemical repellents.
The use of tick repellents, sprayed on clothing or directly on the skin, may be appropriate for adults. In children, increased absorption and resultant toxicity is a concern. The American Academy of Pediatrics recommends that children not be exposed to products containing more than 30% DEET, and that insect repellents not be used in children younger than 2 months. [32] To prevent accidental exposure to the mucous membranes, repellents containing DEET should not be applied to children's hands.
Tick repellents containing DEET or permethrin are appropriately used when exposure to an endemic environment is imminent. DEET is available in 5-100% concentrations as sprays, creams, gels, lotions, solutions, towelettes, and other formulations. In most circumstances, products containing 10-35% DEET are sufficient to provide adequate protection from ticks.
The degree of protection is proportionally related to the concentration of DEET; 10% DEET provides protection for about 2 hours, while 30% DEET protects for about 5 hours. Selection of the DEET concentration should be based on the length of time to be spent outside; for example, someone who expects to be outdoors for an hour should use a product with 10% DEET. Extended-release liposphere microdispersion DEET preparations (6.5% and 10%) may decrease exposure to high concentrations of DEET while maintaining a relatively long (2-4 h) duration of activity.
Other recommendations to reduce DEET exposure include the following [32] :
-
Use a minimal amount of product to cover the exposed skin and clothes
-
Avoid contact with mucous membranes, open cuts, or irritated skin
-
Wash treated areas with soap and water immediately after returning indoors
Antibiotic prophylaxis
In general, avoiding exposure and removing ticks promptly is a much better strategy than using prophylactic antibiotics. Even in endemic areas, the risk of transmission from a tick bite is estimated to be only 1-2%. For patients with unattached ticks or with ticks that are not engorged, no prophylactic therapy is recommended. For a description of criteria for prophylactic antibiotic use, see Treatment.
Animals
Because pets can develop Lyme disease and can carry ticks, making sure they are wearing tick collars seems prudent. Applying the suggestions concerning skin inspection may also be prudent after playing with outdoor pets. Any ticks found on pets should be removed promptly. In animal studies, a preferred method of removing ticks is not clearly evident. Removal by holding on to the body of the tick does not increase the transmission rate.
-
Lyme disease. The bacterium Borrelia burgdorferi (darkfield microscopy technique, 400X; courtesy of the US Centers for Disease Control and Prevention).
-
Lyme disease. Magnified ticks at various stages of development.
-
Ticks are the most common vectors for vector-borne diseases in the United States. In North America, tick bites can cause Lyme disease, human granulocytic and monocytic ehrlichiosis, babesiosis, relapsing fever, Rocky Mountain spotted fever, Colorado tick fever, tularemia, Q fever, and tick paralysis. Europe has a similar list of illnesses caused by ticks, but additional concerns include boutonneuse fever and tick-borne encephalitis. Lyme disease is one of the most prominent tick-borne diseases, and its main vector is the tick genus Ixodes, primarily Ixodes scapularis. Image courtesy of the US Centers of Disease Control and Prevention.
-
Lyme disease. Approximate US distribution of Ixodes scapularis. Image courtesy of the US Centers for Disease Control and Prevention.
-
Lyme disease. In general, Ixodes scapularis must be attached for at least 24 hours to transmit the spirochete to the host mammal. Prophylactic antibiotics are more likely to be helpful if feeding is longer. This photo shows 2 I scapularis nymphs. The one on the right is unfed; the other has been feeding for 48 hours. Note its larger size and the fact that the midgut diverticula (delicate brown linear areas on the body) are blurred. Photo by Darlyne Murawski; reproduced with permission.
-
Lyme disease. Normal and engorged Ixodes ticks.
-
Amblyomma americanum is the tick vector for monocytic ehrlichiosis and tularemia. An adult and a nymphal form are shown (common match shown for size comparison). Image by Darlyne Murawski; reproduced with permission.
-
Approximate US distribution of Amblyomma americanum. Image courtesy of the US Centers for Disease Control and Prevention.
-
The soft-bodied tick of the genus Ornithodoros transmits various Borrelia species that cause relapsing fever. Photo courtesy of Julie Rawlings, MPH, Texas Department of Health. Relapsing fever is characterized by recurrent acute episodes of fever (usually >39°C). It is a vector-borne illness spread by lice and ticks. The spirochete species Borrelia is responsible.
-
The Ixodes scapularis tick is considerably smaller than the Dermacentor tick. The former is the vector for Lyme disease, granulocytic ehrlichiosis, and babesiosis. The latter is the vector for Rocky Mountain spotted fever. This photo displays an adult I scapularis tick (on the right) next to an adult Dermacentor variabilis; both are next to a common match displayed for scale. Photo by Darlyne Murawski; reproduced with permission.
-
Approximate US distribution of Dermacentor andersoni. Image courtesy of the US Centers for Disease Control and Prevention.
-
Rhipicephalus ticks are vectors for babesiosis and rickettsial infections, among others. Image courtesy of Dirk M. Elston, MD. In typical practice, testing ticks for tick-borne infectious organisms is not generally recommended. However, healthcare practitioners should become familiar with the clinical manifestations of tick-borne diseases (eg, Lyme disease, especially those practicing in endemic areas) and maintain a high index of suspicion during warmer months. Ticks can be placed in a sealed container with alcohol if they need to be transported and identified.
-
To remove a tick, use fine-tipped forceps and wear gloves. Grasp the tick as close to the skin surface as possible, including the mouth parts, and pull upward with steady, even traction. Do not twist or jerk the tick because this may cause the mouth parts to break off and remain in the skin; however, note that the mouth parts themselves are not infectious. When removing, wear gloves to avoid possible infection.
-
Lyme disease. This patient's erythema migrans rash demonstrates several key features of the rash, including size, location, and presence of a central punctum, which can be seen right at the lateral margin of the inferior gluteal fold. Note that the color is uniform; this pattern probably is more common than the classic pattern of central clearing. On history, this patient was found to live in an endemic area for ticks and to pull ticks off her dog daily.
-
Erythema migrans, the characteristic rash of early Lyme disease.
-
Lyme disease. The thorax and torso are typical locations for erythema migrans. The lesion is slightly darker in the center, a common variation. In addition, this patient worked outdoors in a highly endemic area. Physical examination also revealed a right axillary lymph node.
-
Lyme disease. Photo of the left side of the neck of a patient who had pulled a tick from this region 7 days previously. Note the raised vesicular center, which is a variant of erythema migrans. The patient had a Jarisch-Herxheimer reaction approximately 18 hours after the first dose of doxycycline.
-
Lyme disease. Classic target lesion with concentric rings of erythema, which often show central clearing. Although this morphology was emphasized in earlier North American literature, it only represents approximately 40% of erythema migrans lesions in the United States. This pattern is more common in Europe. Courtesy of Lyme Disease Foundation, Hartford, Conn.
-
Typical appearance of erythema migrans, the bull's-eye rash of Lyme disease.
-
Lyme disease. Bulls-eye rash.
-
Lyme disease. Photo of erythema migrans on the right thigh of a toddler. The size and location are typical of erythema migrans, as is the history of the patient vacationing on Fire Island, NY, in the month of August. No tick bite had been noted at this location. Approximately 25% of patients with Lyme disease are children, which is the same percentage of patients who do not recall a tick bite. Courtesy of Dr John Hanrahan.
-
Lyme disease. Multiple lesions of erythema migrans occur in approximately 20% of patients. A carpenter from Nantucket who worked predominantly outside had been treated with clotrimazole/betamethasone for 1 week for a presumed tineal infection, but the initial lesion grew, and new ones developed. He then presented to the emergency department with the rashes seen in this photo. The patient had no fever and only mild systemic symptoms. He was treated with a 3-week course of oral antibiotics.
-
Lyme disease. The rash on the ankle seen in this photo is consistent with both cellulitis (deep red hue, acral location, mild tenderness) and erythema migrans (presentation in July, in an area highly endemic for Lyme disease). In this situation, treatment with a drug that covers both diseases (eg, cefuroxime or amoxicillin-clavulanate) is an effective strategy.
-
Lyme disease. Borrelial lymphocytoma of the earlobe, which shows a bluish red discoloration. The location is typical in children, as opposed to the nipple in adults. This manifestation of Lyme disease is uncommon and occurs only in Europe. Courtesy of Lyme Disease Foundation, Hartford, Conn.
-
A rarely reported noninfectious complication for tick bites is alopecia. It can begin within a week of tick removal and typically occurs in a 3- to 4-cm circle around a tick bite on the scalp. A moth-eaten alopecia of the scalp caused by bites of Dermacentor variabilis (the American dog tick) has also been described. No particular species appears more likely to cause alopecia. Hair regrowth typically occurs within 1-3 months, although permanent alopecia has been observed.
-
Acrodermatitis chronica atrophicans is found almost exclusively in European patients and comprises an early inflammatory phase and a later atrophic phase. As the term suggests, the lesion occurs acrally and ultimately results in skin described as being like cigarette paper. Courtesy of Lyme Disease Foundation, Hartford, Conn.
-
Blood smear showing likely babesiosis. Babesiosis can be difficult to distinguish from malaria on a blood smear.
-
Life cycle of the Ixodes dammini tick. Courtesy of Elsevier.
-
Lyme disease in the United States is concentrated heavily in the northeast and upper Midwest; it does not occur nationwide. Dots on the map indicate the infected person's county of residence, not the place where they were infected. Courtesy of the US Centers for Disease Control and Prevention (CDC).
Tables
- Table 1. Clinical presentation and therapy for the stages of Lyme disease
- Table 2. Adult and pediatric treatment options, dosages, and routes of administration
- Table 3. Comparison of Infectious Diseases Society of America (IDSA) and International Lyme and Associated Diseases Society (ILADS) recommendations for Lyme disease treatment
Clinical Manifestations |
Adult Dose |
Pediatric Dose |
Erythema migrans |
Doxycycline 100 mg PO BID for 10-14 days, OR
Amoxicillin 500 mg PO TID for 14 days, OR
Cefuroxime axetil 500 mg PO BID for 14 days
Patients unable to take doxycycline or beta-lactam antibiotics: Azithromycin 500 mg PO qDay for 7 days |
Doxycycline 4.4 mg/kg/day PO, divided into 2 doses; not to exceed 100 mg/dose for 10-14 days, OR
Amoxicillin 50 mg/kg/day PO, divided into 3 doses; not to exceed 500 mg/dose for 14 days, OR
Cefuroxime axetil 30 mg/kg/day PO, divided into 2 doses; not to exceed 500 mg/dose for 14 day |
Facial palsy [3] |
Doxycycline 100 mg PO BID for 14-21 days |
Doxycycline 4.4 mg/kg/day PO, divided into 2 doses; not to exceed 100 mg/dose for 14-21 days |
Lyme meningitis or radiculoneuritis [3] |
Doxycycline 200 mg/day PO, divided into 1-2 doses for 14-21 days, OR
Ceftriaxone 2 g IV qDay for 14-21 days; may substitute for oral therapy once the patient is stabilized or discharged to complete the course |
Doxycycline 4.4 mg/kg/day PO, divided into 1-2 doses; not to exceed 100 mg/dose for 14-21 days, OR
Ceftriaxone 50-75 mg/kg IV qDay; not to exceed 2 g/day for 14-21 days; may substitute for oral therapy once the patient is stabilized or discharged to complete the course |
Lyme disease–associated meningitis, cranial neuropathy, radiculoneuropathy, or with other peripheral nervous system (PNS) manifestations |
Without parenchymal involvement of brain or spinal cord: IV ceftriaxone, cefotaxime, penicillin G, or oral doxycycline With parenchymal involvement of brain or spinal cord: IV antibiotics are preferred |
|
Mild lyme carditis (1st degree AV block with PR interval < 300 milliseconds) [3] |
Doxycycline 100 mg PO BID for 14-21 days, OR
Amoxicillin 500 mg PO TID for 14-21 days, OR Cefuroxime axetil 500 mg PO BID for 14-21 days |
Doxycycline 4.4 mg/kg/day PO, divided into 2 doses; not to exceed 100 mg/dose for 14-21 days, OR
Amoxicillin 50 mg/kg/day PO, divided into 3 doses; not to exceed 500 mg/dose for 14-21 days, OR
Cefuroxime axetil 30 mg/kg/day PO, divided into 2 doses; not to exceed 500 mg/dose for 14-21 days |
Severe lyme carditis (symptomatic, 1st degree AV block with PR interval ≥300 milliseconds, 2nd or 3rd degree AV block) [3] |
Ceftriaxone 2 g IV qDay for 14-21 days; once symptoms and high-grade AV block resolve, consider transitioning to oral antibiotics to complete treatment course |
Ceftriaxone 50-75 mg IV qDay; not to exceed 2 g/day for 14-21 days; once symptoms and high-grade AV block resolve, consider transitioning to oral antibiotics to complete treatment course |
Borrelial lymphocytoma |
Oral antibiotic therapy for 14 days |
|
Arthritis |
Doxycycline 100 mg PO BID for 28 days, OR
Amoxicillin 500 mg PO TID for 28 days, OR
Cefuroxime axetil 500 mg PO BID for 28 days |
For ≥8 years:
Doxycycline 4.4 mg/kg/day PO, divided into 2 doses; not to exceed 100 mg/dose for 28 days, OR
Amoxicillin 50 mg/kg/day PO, divided into 3 doses; not to exceed 500 mg/dose for 28 days, OR
Cefuroxime axetil 30 mg/kg/day PO, divided into 2 doses; not to exceed 500 mg/dose for 28 days
For < 8 years:
Amoxicillin 50 mg/kg/day PO, divided into 3 doses; not to exceed 500 mg/dose for 28 days, OR
Cefuroxime axetil 30 mg/kg/day PO, divided into 2 doses; not to exceed 500 mg/dose for 28 days |
Arthritis without any response to initial treatment |
Ceftriaxone 2 g IV qDay for 14-28 days |
Ceftriaxone 50-75 mg IV qDay; not to exceed 2 g/day for 14-28 days |
Acrodermatitis chronica atrophicans |
Oral antibiotic therapy 21-28 days |
|
|
Treatment |
Adult Dose |
Pediatric Dose |
Oral Therapy |
Doxycycline (patients > 8 y) |
100 mg twice a day |
Doxycycline 4.4 mg/kg/day PO (up to 100 mg BID) |
Amoxicillin |
500 mg three times a day |
50 mg/kg/day (up to 500 mg) in 3 divided doses |
|
Cefuroxime axetil |
500 mg twice a day |
30 mg/kg/day (up to 500 mg) in 2 divided doses |
|
Phenoxymethylpenicillin |
500 mg four times a day, or 1 gm three times a day |
50-100 mg/kg/day in three divided doses; maximum 1 g/dose |
|
Azithromycin (for patients unable to take doxycycline or beta-lactams) |
500 mg once a day
|
50-100 mg/kg/day in three divided doses; maximum 1 g/dose |
|
Intravenous therapy |
Ceftriaxone |
2 g once a day |
10 mg/kg/day (maximum, 500 mg/day) |
Cefotaxime |
2 g every 8 h |
150-200 mg/kg (up to 2 g) every 8 h |
|
Penicillin G |
18-24 million U/d divided every 4 h |
200,000-400,000 mg/kg (up to 2 g) every 8 h |
Treatment Focus |
IDSA |
ILADS |
Treatment of a tick bite without symptoms of Lyme disease |
Doxycycline, 200 mg as a single dose |
Doxycycline, 100 mg bid for 20 days |
Erythema migrans |
Doxycycline, amoxicillin, or cefuroxime for 14-21 days |
Doxycycline, amoxicillin, or cefuroxime for 28-42 days or azithromycin for at least 21 days |
“Persisting symptoms of Lyme disease” |
No antibiotic therapy |
Multiple agents (individually or in combination) are mentioned without specific doses or duration recommended |





