Practice Essentials
Giant cell arteritis (GCA), or temporal arteritis, is a systemic inflammatory vasculitis of unknown etiology that occurs in older persons and can result in a wide variety of systemic, neurologic, and ophthalmologic complications. [1, 2] GCA is the most common form of systemic vasculitis in adults. Other names for GCA include arteritis cranialis, Horton disease, granulomatous arteritis, and arteritis of the aged.
GCA is classified as a large-vessel vasculitis [3] but typically also involves medium and small arteries, particularly the superficial temporal arteries—hence the term temporal arteritis. In addition, GCA most commonly affects the ophthalmic, occipital, vertebral, posterior ciliary, and proximal vertebral arteries. Medium- and large-sized vessels that may be involved include the aorta and the carotid, subclavian, and iliac arteries. [4]
Histopathologically, GCA is marked by transmural inflammation of the intima, media, and adventitia of affected arteries, as well as patchy infiltration by lymphocytes, macrophages, and multinucleated giant cells. Mural hyperplasia can narrow the arterial lumen, resulting in distal ischemia. (See Pathophysiology.)
Age and female sex are established risk factors for GCA, a genetic component seems likely, and infection may have a role (see Etiology). One school of thought considers GCA and polymyalgia rheumatica to be different manifestations of the same disease process, while others see them as closely related but different diseases. [5, 6]
Common signs and symptoms of GCA reflect the involvement of the temporal artery and other medium-sized arteries of the head and the neck and include visual disturbances, headache, jaw claudication, neck pain, and scalp tenderness. Constitutional manifestations, such as fatigue, malaise, and fever, may also be present. (See Presentation.)
GCA should always be considered in the differential diagnosis of a new-onset headache in patients 50 years of age or older with an elevated erythrocyte sedimentation rate. Temporal artery biopsy remains the criterion standard for diagnosis of this granulomatous vasculitis (see the image below). However, increasing evidence supports the use of imaging studies for diagnosis in patients at high clinical risk.
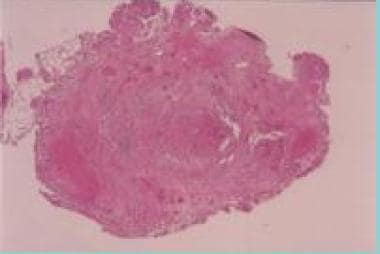 Hematoxylin- and eosin-stained superficial temporal artery biopsy specimen, cross section. The hallmark histologic features of GCA shown here include intimal thickening with luminal stenosis, mononuclear inflammatory cell infiltrate with media invasion and necrosis, and giant cell formation in the media.
Hematoxylin- and eosin-stained superficial temporal artery biopsy specimen, cross section. The hallmark histologic features of GCA shown here include intimal thickening with luminal stenosis, mononuclear inflammatory cell infiltrate with media invasion and necrosis, and giant cell formation in the media.
Visual loss is one of the most significant causes of morbidity in GCA. Permanent visual impairment may occur in as many as 20% of patients, and, in some cases, GCA can cause bilateral blindness. [7] Newly recognized GCA should be considered a true neuro-ophthalmic emergency.
Prompt initiation of treatment may prevent blindness and other potentially irreversible ischemic sequelae of GCA. [8] Corticosteroids are the mainstay of therapy. In steroid-resistant cases, drugs such as tocilizumab, cyclosporine, azathioprine, or methotrexate may be used as steroid-sparing agents. The typical patient with GCA remains on steroid therapy for roughly 2 years. (See Treatment and Medication.)
Pathophysiology
Giant cell arteritis (GCA) is primarily a disease of cell-mediated immunity, which is thought to arise as a maladaptive response to endothelial injury. Actinic damage to the temporal artery from chronic sun exposure has been proposed as one source of the injury. [9] The adventitia is the likely site of initial immunologic injury and is considered the immunological center of the disorder, while the intima and media are the histological center.
The primary inflammatory response involves the activation of dendritic cells in the adventitia of arteries by an unknown antigen, with production of chemokines that recruit CD4+T helper cells. Activated CD4+ T helper cells polarize into Th1 cells (producing interferon gamma) and Th17 cells (producing interleukin 17).
Interferon gamma causes endothelial cells and vascular smooth muscle to recruit more Th1 cells, CD8+ T cells, and monocytes.The monocytes differentiate into macrophages and the characteristic giant cells that produce growth factors, other interleukins and proteolytic enzymes that progressively narrow and obstruct the vessel wall. [10] The inflammation tends to occur in a segmental or patchy manner, although long portions of arteries may be involved. [11]
Systemic manifestations are likely related to the inflammatory process and cytokine elaboration. End-organ involvement relates to hyperplasia and occlusion of the arteries serving those organs.
Concentric intimal hyperplasia is an important underlying pathologic lesion in GCA. Intimal hyperplasia presumably occurs as a repair mechanism in response to injury of the blood vessel wall.
Platelet-derived growth factor (PDGF) is important in stimulating intimal hyperplasia. In GCA, PDGF derives from macrophages and giant cells, and this distinguishes GCA from other vasculopathies. In atherosclerotic disease, for example, PDGF is produced mostly by resident smooth muscle cells rather than monocytes.
Intimal macrophages also produce vascular endothelial growth factor (VEGF), which promotes intimal proliferation. Medial macrophages generate metalloproteinases, leading to the destruction of vascular elements, including the internal elastic lamina. [12] Adventitial macrophages produce interleukin-6, augmenting the inflammatory response. This results in inflammation with local vascular damage and intimal hyperplasia, leading to stenosis and occlusion. [13]
Cell adhesion molecules influence the pathogenesis, and endothelial cells play a pivotal role. Inflammation is an important process that influences the endothelium and causes neovascularization. This process occurs mainly at the intima-media junction and at the adventitial layer.
Adhesion molecules are far more intensely expressed on these neovessels than in the vessel lumen. Using immunochemical staining, Cid et al demonstrated that different adhesion molecules might regulate how leukocytes and endothelial cells interact in different temporal artery layers. [14]
A study by Maugeri et al showed that patients with GCA had increased expression of platelets expressing P-selectin, of platelet-Nph and platelet-Mo aggregates, and of Nph and Mo expressing tissue factor. [15] Activated platelets and white cells could cause vessel inflammation and thromboembolic events. [16]
Elastin
A cellular immune reaction to elastin has been implicated in the pathogenesis of GCA. [17] In support of the hypothesis that elastin is the inciting antigen, disease severity has been shown to correlate with the amount of elastic tissue within the vessels. [18] For example, intracranial arteries lack an internal elastic lamina, and GCA does not cause a widespread intracranial cerebral vasculitis.
This hypothesis also is supported by histopathologic findings of a disrupted, fragmented internal elastic lamina in affected vessels and the presence of characteristic giant cells, which may contain elastic fiber fragments, close to the internal elastic lamina. Along with elevated serum levels of neutrophil elastase, deposition of elastase along the damaged internal elastic lamina has been described.
Pattern of involvement
The superficial temporal artery is involved in most patients, providing a convenient biopsy site, but this is only the "tip of the iceberg." GCA commonly affects arteries in the following pattern:
-
Common, external, and internal carotid artery involvement is usually extracranial; rarely, proximal intracranial segments have been affected
-
Intraorbital branches, especially the posterior ciliary and ophthalmic arteries, are commonly affected
-
Vertebral arteries are involved as frequently as the superficial temporal arteries in fatal cases, although basilar artery involvement is rare
-
Vertebral arteritis is extracranial, but it may extend intracranially for roughly 5 mm beyond dural penetration
-
Subclavian, axillary, and proximal brachial arterial involvement produces a characteristic angiographic pattern of vasculitis, consisting of long, smooth, stenotic segments that alternate with nonstenotic segments and tapered occlusions
-
Involvement of the ascending aorta can lead to aortic rupture, and coronary arteritis may result in myocardial infarction (MI)
-
Pulmonary arterial involvement has also been described
-
Some veins may be affected occasionally
The most common cause of vision loss in GCA is anterior ischemic optic neuropathy (AION). This results from ischemia of the optic nerve head, which is supplied mainly by the posterior ciliary arteries.
Finally, numerous studies now suggest that GCA consists of various clinical subsets rather than one uniform disease. Variable expression of different cytokine profiles likely determines the clinical manifestations. Tumor necrosis factor (TNF) and, more recently, interleukin 6, have been recognized to play a major role in the pathophysiology of temporal arteritis. [21]
Relationship with polymyalgia rheumatica
A close relationship exists between GCA and polymyalgia rheumatica. [22, 23, 24] About 50% of patients with GCA have underlying polymyalgia rheumatica, and about 15% of individuals with polymyalgia rheumatica develop GCA. The precise nature of this association is poorly understood. Several authors have suggested that these 2 diseases are actually different stages of the same disease process.
Etiology
The exact etiology of giant cell arteritis (GCA) remains unknown. Despite increased understanding of the inflammatory cascade responsible for the disease process, the initial event that triggers the cascade remains uncertain. Genetic, environmental, and autoimmune factors have been identified.
Reports of familial aggregation, [25] association with the HLA-DR4 haplotype, and an apparent higher frequency of these conditions in northern Europe and in persons in the United States with similar ethnic backgrounds suggest a genetic or hereditary predisposition. GCA is less common among African Americans. A possible association between Toll-like receptor 4 gene polymorphism and susceptibility to biopsy-proven GCA has been found. [26]
Epidemiological observations, reports, and studies using DNA detection techniques have implicated Chlamydia pneumoniae, Mycoplasma pneumoniae, parvovirus B19, and varicella zoster as the impetus for the destructive inflammation. [27, 28, 29] Nevertheless, it is generally accepted that these infectious agents are only "innocent bystanders."
The immune system (both cellular and humoral) has been implicated in the pathogenesis of GCA. The granulomatous histopathology of GCA has suggested the presence of an antigen-driven disease with local T-cell and macrophage activation in or near elastic tissue in the arterial walls with an important role of the proinflammatory cytokines. [30, 31] It may begin as a foreign body giant cell attack on calcified internal elastic membrane in the arteries and on calcified atrophic parts of the aortic media.
Epidemiology
United States statistics
The reported incidence of GCA ranges from approximately 0.5 to 27 cases per 100,000 people aged 50 years or older. [16] The annual incidence is higher in northern areas of the United States.
A review from Olmsted County, Minnesota identified 125 cases over a period of 42 years, representing an average annual incidence rate of 17.8 cases per 100,000 population aged 50 years and older and a prevalence of persons with active or remitted GCA of 200 cases per 100,000 population aged 50 years or older. A regular cyclical pattern in incidence over 20 years was noted. [32]
International statistics
The prevalence of GCA depends heavily on the number of individuals aged 50 years or older; the mean age of onset is 75 years. Countries with a lower life expectancy have a lower prevalence. Incidence figures reporting biopsy-proven GCA may be lower than those that include clinically diagnosed cases of GCA.
The annual incidence in northern European countries has been reported to be more than 20 cases per 100,000 people over the age of 50 years. A United Kingdom study reported an incidence of 22 per 100,000 in that age group. [33] Scandinavian countries report the highest incidence of GCA—up to 32.4 per 100,000 individuals over the age of 50 years.
The annual incidence in southern European countries has been reported to be less than 12 cases per 100,000 people. In Lugo, Spain, the average annual incidence for the population aged 50 years and older was 10 cases per 100,000 people.
In Canada, the estimated incidence of biopsy-proven GCA for the population aged older than 50 years is 4.9 to 9.4 cases per 100,000 people. [34, 35] A series comprising all adult subjects undergoing autopsy at two hospitals in southern Sweden revealed arteritis in 1.6% of 889 cases, suggesting that GCA may be more common than is clinically apparent. [36]
The incidence of GCA in Saudi Arabia is probably less than in the United States and Western Europe. In 1998, Bosley and Riley reported only 4 positive biopsy results from 72 temporal artery biopsies performed over a 15-year period in Saudi patients. [37]
Racial differences in incidence
Although existing epidemiologic studies are limited because they have been performed on predominantly white populations, the results of these studies suggest that GCA primarily affects whites, specifically those of northern European descent. Scandinavians have the highest prevalence. GCA is less common in African Americans and Asians. [38] Although GCA had been considered less common among Hispanic persons, [39] recent evidence has challenged this notion.
Sexual and age-related differences in incidence
The female-to-male ratio in GCA is roughly 3.7:1. Smoking increases the risk 6-fold in women.
Age is the most important risk factor for GCA. The disease is rare in patients younger than 50 years. In those 50 years and older, the incidence increases with age, peaking in the seventh to eighth decade. The age range in one series of 166 biopsy-proven cases was 55-92 years. The median age of onset is 75 years. GCA is the most common systemic vasculitis affecting elderly patients.
Prognosis
With prompt, adequate therapy, full recovery is the rule. Symptoms from temporal arteritis improve within days of treatment. Corticosteroids can usually be tapered within the first 4-6 weeks and eventually discontinued. The reduced rate of neuro-ophthalmologic complications in recent years reflects improved recognition and treatment; blindness is now a rare complication.
Although the overall course of the disease is one of progressive improvement and eventual complete resolution, the clinical course is highly variable. The average duration of treatment is 2 years; however, some patients require treatment for 5 years or more. [17, 13] Morbidity from steroid therapy can be worse than that from the underlying disease, with the exception of blindness. Rarely, patients do not respond to steroid therapy or doses cannot be tapered. Cytotoxic or immunosuppressive drugs have been recommended in such cases, but more data are needed.
Restuccia et al reported that 73 of 131 patients (56%) with biopsy-proven transmural GCA maintained complete clinical remission without elevation of inflammatory markers for at least 1 year after the withdrawal of steroids. Normal hemoglobin levels were significantly positively associated with long-term remission, while polymyalgia at the time of GCA diagnosis was significantly negatively associated with long-term remission. [40]
In a study that included 35 patients with both polymyalgia rheumatic and temporal arteritis, Narváez and colleagues found that no clinical feature was associated with increased risk of relapse. However, they reported that multivariate analysis identified the following as significant risk factors associated with long duration of steroid therapy [41] :
-
Older age at diagnosis
-
Female sex
-
Higher baseline erythrocyte sedimentation rate
-
Lower daily corticosteroid dose
The prognosis for patients with untreated GCA is extremely poor. These patients may suffer blindness, or death from myocardial infarction, stroke, or dissecting aortic aneurysm. Ophthalmic complications are common and include visual disturbances, amaurosis fugax, diplopia, and blindness from involvement of the ophthalmic artery. Visual loss in GCA is often irreversible, but may be temporary; may be partial or complete; and may involve one or both eyes. Blindness usually occurs abruptly and painlessly. Ischemic optic neuropathy with eventual optic atrophy is the most common cause of visual loss and occurs in 15% of patients.
Vision damage that occurs before initiation of therapy is often irreversible, [42] especially in patients who have other ischemic complications. [43] In patients whose vision loss is initially unilateral, the second eye may become affected even after the initiation of treatment (possibly because those vessels have already been affected by arteritis) in 6-13% of patients. [44]
Progression of vision loss despite the initiation of high-dose corticosteroid therapy typically occurs within the first 5-6 days of treatment if therapy is going to fail. [45, 46] Risk factors for progressive visual loss despite steroid therapy include older age, elevated CRP level, and optic disc swelling. [47]
Nervous system alterations are found in as many as 30% of patients; 14% have either mononeuritis or polyneuropathy, and 7% have transient ischemic attacks or strokes. [48] Strokes from GCA may lead to multi-infarct dementia. Solans-Laqué et al report 7 patients with biopsy-proven GCA who presented with stroke or multi-infarct dementia. [49] Rare but serious complications include myocardial infarction (MI) and visceral organ ischemia (eg, small-bowel infarction). [50, 51, 19]
Complications of long-term steroid treatment that may occur in patients with GCA include the following:
-
Vertebral body compression fracture (26%)
-
Symptomatic steroid myopathy (11%)
-
Steroid psychosis (3%)
Mortality/morbidity
An observational cohort study using a United Kingdom primary care database found that GCA is associated with increased risks for MI, stroke, and peripheral vascular disease. The hazard ratios were 2.06 for MI, 1.28 for stroke, and 2.13 for peripheral vascular disease. Hazard ratios were more pronounced in the first month after the diagnosis of GCA. [52]
GCA leads to death by stroke or MI in roughly 2% of cases. As would be expected, the topographic extent and severity of the vasculitis is greater in fatal than in nonfatal cases. More difficult to quantify are the number of patients whose deaths are related directly or indirectly to chronic corticosteroid use and its attendant complications (eg, hip fracture).
A population-based cohort study from South Australia found that mortality rates in patients with biopsy-proven GCA were similar to those in the general population. Cardiovascular disease was the most common cause of death, followed by infection and cancer. An increased risk of death from infection was more common in the first year, which may be related to immunosuppression from higher doses of corticosteroids at that stage of the disease. [53]
The inflammatory process may weaken the aortic wall, leading to localized aneurysm formation, aortic annular dilatation, and aortic regurgitation. Narrowing or occlusion of the branch vessels of the thoracic aorta (clinically referred to as aortic arch syndrome) may be found in 9-14% of cases, producing symptoms similar to those of Takayasu arteritis (decreased upper extremity pulses and blood pressure, arm or leg claudication, Raynaud phenomenon, transient ischemic attacks, coronary ischemia, and abdominal angina).
Evans and colleagues reported aortic aneurysms occurring in 15% of patients at a median of 6 years after the initial diagnosis of GCA. Two thirds were thoracic aortic aneurysms, with the majority located in the ascending aorta. Almost 33% of patients developed symptomatic aortic regurgitation. Approximately 50% of patients with thoracic aortic aneurysms died suddenly from aortic dissection.
In very rare cases, GCA involves the central nervous system (CNS), producing abnormal mental status, seizures, or strokes. This is despite the fact that GCA for the most part affects only vessels with an elastica, which intradural blood vessels do not have. However, involvement of the aortic arch vessels, including the subclavian arteries, can lead to subclavian steal syndrome and brain ischemia.
Peripheral nerve involvement is rare in GCA. For unknown reasons, renal involvement is also rare.
Patient Education
Education is the most important step in helping the patient appreciate the clinical facets of this illness, the potential adverse effects of the therapy, and the need for monitoring. Patients who experienced visual loss prior to the initiation of therapy should be cautioned that despite therapy, the lost vision may not be regained.
Patients must be instructed about the risk of complications and symptomatic relapses. Advise patients to immediately consult a physician if they experience symptoms of transient blurring of vision because of the possibility of impending attacks of GCA or transient ischemic attack.
Patients must understand the importance of strictly adhering to their steroid dose schedule and the possible need for ancillary interventions, such as dietary restrictions, to reduce the incidence of steroid-related adverse effects. To avoid misunderstandings, inform patients and their families about vertebral compression fracture and other potential complications of steroid therapy that can occur even with proper therapy.
Patients should be informed that they carry a lifelong risk for the development of large-vessel disease, particularly aortic aneurysms. The need for long-term followup should be stressed.
For patient education information, see Temporal Arteritis.
-
Hematoxylin- and eosin-stained superficial temporal artery biopsy specimen, cross section. The hallmark histologic features of GCA shown here include intimal thickening with luminal stenosis, mononuclear inflammatory cell infiltrate with media invasion and necrosis, and giant cell formation in the media.
-
Lumbar angiogram showing stenosis and occlusion of femoral artery branches due to vasculitis.
-
Hematoxylin- and eosin-stained femoral artery branch, cross section, taken from a lower limb amputation specimen. Mononuclear cell invasion and necrosis in the media of this large artery can be observed. Extensive lower limb vasculitis from GCA resulted in ischemic necrosis of the lower limb, necessitating amputation.
-
Hematoxylin and eosin stain, low power. Temporal artery. Note the thrombosis in the lumen, intimal hyperplasia, and infiltration of the arterial wall muscular layers with inflammatory cells. A multinucleated giant cell is seen internal to the muscularis at the area of the internal elastic lamina (upper right).
-
Anterior ischemic optic neuropathy. Image courtesy of Richard Kho, MD, Q.C. Eye Center, Quezon City, Philippines.
-
Branch retinal vein occlusion in a patient with giant cell arteritis. Image courtesy of Manolette Roque, MD, Roque Eye Clinic, Manila, Philippines.
-
Central retinal artery occlusion (CRAO).
-
Prominent temporal artery is visible on the temple of a 76-year-old woman with temporal arteritis. Courtesy of ScienceSource (https://www.sciencesource.com/).







