Ozgur O, Kaufman EJ. Ectropion. StatPearls. 2023 Jan. [QxMD MEDLINE Link]. [Full Text].
Gupta B, Parmar B, Raina J, Chawla JS. Acute idiopathic bilateral lower lid ectropion. Indian J Ophthalmol. 2006 Sep. 54(3):212-4. [QxMD MEDLINE Link].
Damasceno RW, Osaki MH, Dantas PE, Belfort R Jr. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly population. Ophthal Plast Reconstr Surg. 2011 Sep-Oct. 27(5):317-20. [QxMD MEDLINE Link].
Balogun BG, Adekoya BJ, Balogun MM, Ngwu RV, Oworu O. Ectropion and entropioin in sub-Saharan Africa: how do we difer?. Ann Afr Med. Oct-Dec/2013. 12:193-6.
Fezza JP. Nonsurgical treatment of cicatricial ectropion with hyaluronic acid filler. Plast Reconstr Surg. 2008 Mar. 121(3):1009-14. [QxMD MEDLINE Link].
Schrom T, Habermann A. Temporary ectropion therapy by adhesive taping: a case study. Head Face Med. 2008 Jul 21. 4:12. [QxMD MEDLINE Link]. [Full Text].
Dobson R. Antiviral drugs should not be used to treat Bell's palsy, Cochrane analysis concludes. BMJ. 2009 Oct 7. 339:b4086. [QxMD MEDLINE Link].
Criglow BG, Choate KA, Milstone LM. Topical tazarotene for the treatment of ectropion in ichthyosis. JAMA Dermatol. May 2013. 149:598-600.
Romero R, Sanchez-Orgaz M, Granados M, Arbizu A, Castano A, Romero A. Use of hyaluronic acid gel in the management of cicatricial ectropion: results and complications. Orbit. 2013 Dec. 32(6):362-5. [QxMD MEDLINE Link].
Bedran EG, Pereira MV, Bernardes TF. Ectropion. Semin Ophthalmol. 2010 May. 25(3):59-65. [QxMD MEDLINE Link].
Berry-Brincat A, Burns J, Sampath R. Inverting sutures for tarsal ectropion (the leicester modified suture technique). Ophthal Plast Reconstr Surg. 2013 Sep. 29(5):400-2. [QxMD MEDLINE Link].
Xue CY, Dai HY, Li L, Wang YC, Yang C, Li JH, et al. Reconstruction of Lower Eyelid Retraction or Ectropion Using a Paranasal Flap. Aesthetic Plast Surg. 2012 Jan 25. [QxMD MEDLINE Link].
Czyz CN, Wulc AE, Ryu CL, Foster JA, Edmonson BC. Caruncular fixation in medial canthal tendon repair: the minimally invasive purse string suture for tendinous laxity and medial ectropion. Ophthal Plast Reconstr Surg. 2015 Jan-Feb. 31 (1):34-7. [QxMD MEDLINE Link].
Genther DJ, Kim LR, Loyo MD, Boahene KD. Transposed Corrugator Supercilii Muscle-Tendon Unit Flap for Contralateral Paralytic Medial Ectropion Repair. JAMA Facial Plast Surg. 2016 Mar 17. [QxMD MEDLINE Link].
Azuma R, Aoki S, Aizawa T, Kuwabara M, Kiyosawa T. The vertical orbicularis oculi muscle turn-over procedure for the correction of paralytic ectropion of the lower eyelid. Arch Plast Surg. 2018 Mar. 45 (2):135-139. [QxMD MEDLINE Link].
Osborne SF, Eidsness RB, Carroll SC, Rosser PM. The use of fibrin tissue glue in the repair of cicatricial ectropion of the lower eyelid. Ophthal Plast Reconstr Surg. 2010 Nov-Dec. 26(6):409-12. [QxMD MEDLINE Link].
Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol. 1979 Nov. 97(11):2192-6. [QxMD MEDLINE Link].
Bashour M, Harvey J. Causes of involutional ectropion and entropion--age-related tarsal changes are the key. Ophthal Plast Reconstr Surg. 2000 Mar. 16(2):131-41. [QxMD MEDLINE Link].
Ben Simon GJ, Molina M, Schwarcz RM, McCann JD, Goldberg RA. External (subciliary) vs internal (transconjunctival) involutional entropion repair. Am J Ophthalmol. 2005 Mar. 139(3):482-7. [QxMD MEDLINE Link].
Bergeron CM, Moe KS. The evaluation and treatment of lower eyelid paralysis. Facial Plast Surg. 2008 May. 24(2):231-41. [QxMD MEDLINE Link].
Caviggioli F, Klinger F, Villani F, Fossati C, Vinci V, Klinger M. Correction of cicatricial ectropion by autologous fat graft. Aesthetic Plast Surg. 2008 May. 32(3):555-7. [QxMD MEDLINE Link].
Chang L, Olver J. A useful augmented lateral tarsal strip tarsorraphy for paralytic ectropion. Ophthalmology. 2006. 113:84-91.
Cook BE Jr, Bartley GB, Pittelkow MR. Ophthalmic abnormalities in patients with cutaneous T-cell lymphoma. Ophthalmology. 1999 Jul. 106(7):1339-44. [QxMD MEDLINE Link].
Frankfort BJ, Garibaldi DC. Periocular cutaneous toxicity and cicatricial ectropion: a potential class effect of antineoplastic agents that inhibit EGFR signaling. Ophthal Plast Reconstr Surg. 2007 Nov-Dec. 23(6):496-7. [QxMD MEDLINE Link].
Hedge V, Robinson R, Dean F, Mulvihill HA, Ahluwalia H. Drug-induced ectropion: what is best practice?. Ophthalmology. 2007. 114:362-6.
Hintschich C. Correction of entropion and ectropion. Dev Ophthalmol. 2008. 41:85-102. [QxMD MEDLINE Link].
Isawumi MA, Adeoti CO, Umar IO, Oluwatimilehin IO, Raji RA. Congenital bilateral eversion of the eyelids. J Pediatr Ophthalmol Strabismus. 2008 Nov-Dec. 45(6):371-3. [QxMD MEDLINE Link].
Jordan DR, Anderson RL. The lateral tarsal strip revisited. The enhanced tarsal strip. Arch Ophthalmol. 1989 Apr. 107(4):604-6. [QxMD MEDLINE Link].
Jordan DR, Bawazeer AM, Pelletier CR. Severe congenital ectropion secondary to lamellar ichthyosis. Can J Ophthalmol. 1998 Feb. 33(1):30-1. [QxMD MEDLINE Link].
Koh S, Hosohata J, Tano Y. Bilateral upper eyelid ectropion associated with blepharospasm. Br J Ophthalmol. 2006 Nov. 90(11):1437-8. [QxMD MEDLINE Link].
Manku K, Leong JK, Ghabrial R. Cicatricial ectropion: repair with myocutaneous flaps and canthopexy. Clin Experiment Ophthalmol. 2006 Sep-Oct. 34(7):677-81. [QxMD MEDLINE Link].
Monaco G, Franceschin S, Cacioppo V, Simonetta S, Ratiglia R. Congenital iris ectropion associated with juvenile glaucoma. J Pediatr Ophthalmol Strabismus. 2009 Jan-Feb. 46(1):35-7. [QxMD MEDLINE Link].
Nowinski TS, Anderson RL. The medial spindle procedure for involutional medial ectropion. Arch Ophthalmol. 1985 Nov. 103(11):1750-3. [QxMD MEDLINE Link].
Oh SR, Korn BS, Kikkawa DO. Orbitomalar suspension wth combined single drill hole canthoplasty. Ophthal Plast Reconstr Surg. Sept 2013. 29:357-60.
Perez-Dieste JM, Catroviejo-Bolbar M. Eyelid ectropion caused by glasses. Mechanical centurion syndrome. Arch Soc Esp Oftalmol. February 2013. 88:80-2.
[Guideline] Salinas RA, Alvarez G, Daly F, Ferreira J. Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2010. (3):CD001942. [QxMD MEDLINE Link].
Smith B. The "lazy-T" correction of ectropion of the lower punctum. Arch Ophthalmol. 1976 Jul. 94(7):1149-50. [QxMD MEDLINE Link].
Tse DT, Kronish JW, Buus D. Surgical correction of lower-eyelid tarsal ectropion by reinsertion of the retractors. Arch Ophthalmol. 1991 Mar. 109(3):427-31. [QxMD MEDLINE Link].
Uthoff D, Gorney M, Teichmann C. Cicatricial ectropion in ichthyosis: a novel approach to treatment. Ophthal Plast Reconstr Surg. 1994 Jun. 10(2):92-5. [QxMD MEDLINE Link].

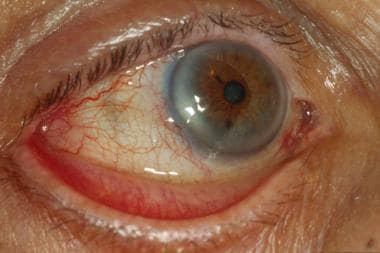 Complete (tarsal) paralytic ectropion in a patient with an ipsilateral parotid tumor.
Complete (tarsal) paralytic ectropion in a patient with an ipsilateral parotid tumor.

