Background
The oculomotor (third) cranial nerve plays an important role in the efferent visual system by controlling ipsilateral eye movements, pupil constriction, and upper eyelid elevation. Accordingly, damage to the third cranial nerve may cause diplopia, pupil mydriasis, and/or upper eyelid ptosis. The clinical manifestations of third cranial nerve dysfunction reflect its constituent parts. Outer parasympathetic fibers supply the ciliary muscles of the eye and the sphincter pupillae (sphincter muscles that cause pupillary constriction). The inner somatic fibers of the third cranial nerve supply the levator palpebrae superioris in the eyelid (controlling upper eyelid elevation), and four extraocular muscles that govern ocular motility (the superior, medial, and inferior recti muscles, and the inferior oblique muscle). [1, 2, 3, 4, 5] Classically, third cranial nerve impairment is associated with a “down and out” appearance of the ipsilateral eye (Figure 1). This eye position reflects the unopposed actions of depression and abduction of the globe, which are governed by superior oblique (innervated by the fourth cranial nerve) and lateral rectus (innervated by the sixth cranial nerve) muscles, respectively. Localizing an isolated third cranial nerve palsy, particularly one that causes a “down and out” position of the ipsilateral eye is relatively straightforward when there is complete involvement of the levator palpebrae superioris (causing complete ptosis), complete paralysis of innervated extraocular muscles, and complete pupillary mydriasis. In reality, however, third cranial nerve palsies are often incomplete and result in partial deficits that may be relatively subtle and easily overlooked (Figure 2). For this reason, it is imperative to carefully establish a good history and perform a thorough examination to localize third cranial nerve lesions, which may herald vision and life-threatening problems.
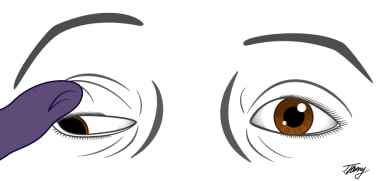 Illustration of a complete right oculomotor palsy demonstrating the classic "down and out" appearance, complete ptosis and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Illustration of a complete right oculomotor palsy demonstrating the classic "down and out" appearance, complete ptosis and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
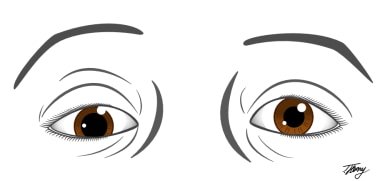 Illustration of a partial right oculomotor nerve palsy demonstrating incomplete ptosis, hypotropia and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Illustration of a partial right oculomotor nerve palsy demonstrating incomplete ptosis, hypotropia and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Pathophysiology
The third cranial nerve, alternatively known as the oculomotor nerve, has multiple important functions. Owing to its elegant anatomical organization and course, third cranial nerve deficits can be readily localised to specific site (nucleus, fascicular portion, cavernous sinus segment, or orbit), depending on the pattern of oculomotor dysfunction observed and associated clinical findings. Broadly speaking, nuclear third cranial nerve palsies may be isolated, or accompanied by other neurologic symptoms given the proximity of the oculomotor nucleus to other important structures in the midbrain tegmentum. [1, 2, 3, 4] The fascicular portion of the oculomotor nerve courses ventrally from the nucleus in the midbrain, crosses through the red nucleus near the corticospinal tract, and emerges from the medial aspect of the cerebral peduncle (Figure 3). [4] Its close proximity to other midbrain structures means that fascicular lesions often co-associate with neurological findings, in addition to oculomotor palsy. [4] The cisternal portion of the third cranial nerve travels in the subarachnoid space anterior to the midbrain after exiting between the superior cerebellar and posterior cerebral arteries (Figure 3). Here, it is vulnerable to compressive effects from vascular lesions, such as aneurysms (Figure 4). The oculomotor nerve runs through the lateral wall of the cavernous sinus. [4] Lesions of the cavernous sinus often produce third nerve palsies that are accompanied by one or more other neurologic findings including palsies of the fourth, fifth (first division), and sixth cranial nerves, with or without an associated Horner syndrome. [4] Finally, the oculomotor nerve enters the orbit through the superior orbital fissure adjacent to the fourth cranial nerve. Usually, the third cranial nerve branches into superior and inferior divisions within the posterior orbit, but, occasionally, divisional branching occurs in cavernous sinus. The superior division of the third cranial nerve innervates the levator palpebrae and the superior rectus muscles. The inferior division innervates all the other muscles innervated by the third nerve, and supplies the preganglionic parasympathetic fibers to the ciliary ganglion, which in turn innervate the iris sphincter. [4] As a general rule of thumb, orbital lesions may be associated with other clinical signs such as proptosis, which can help in the localization process. A more detailed description regarding how anatomical site of injury impacts third cranial nerve function is discussed in the sub-section ”Localizing Third Cranial Nerve Palsies: How Does Form Affect Function?”
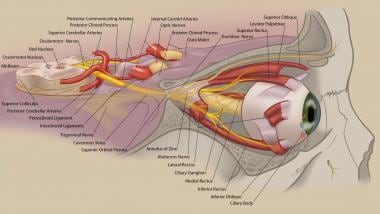 Anatomy of the oculomotor nerve. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Anatomy of the oculomotor nerve. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Epidemiology
Frequency
In a recent population-based cohort study by Fang and colleagues [6] , 145 cases of acquired third cranial nerve palsy diagnosed over a 37-year period in Olmsted County, Minnesota were assessed. The age- and sex-adjusted annual incidence of acquired third nerve palsy was 4.0 per 100 000. [6] Not surprisingly, the annual incidence was higher in older patients (aged greater than 60 years) relative to younger patients (12.5 vs 1.7 per 100 000; difference, 10.8 per 100 000; P < .001). [6] This observation likely reflected the higher predilection for microvascular ischemic third nerve cranial nerve palsies in older versus younger adults. [6] In this study, the most common causes of acquired third nerve palsy were presumed microvascular injury (42%), trauma (12%), compression (from neoplastic lesions) (11%), post-operative neurosurgical cases (10%), and aneurysmal compression (6%). [6] Notably, 10 patients (17%) with microvascular ischemic third nerve palsies had pupil involvement, whereas pupil involvement was seen in not all, but only 16 patients (64%) with compressive third nerve palsies. [6] The findings from Fang et al [6] bear careful consideration, because although compressive lesions had a higher likelihood of pupil involvement, pupil involvement did not exclude microvascular third nerve palsy; moreover, lack thereof did not rule out potentially life-threatening causes of compressive third nerve palsy.
Mortality/Morbidity
The morbidity and mortality caused by third cranial nerve palsies are intrinsically linked to etiology, the details of which are beyond the scope of this article.
That said, several important causes of mortality and morbidity presenting with evidence of oculomotor dysfunction include: subarachnoid hemorrhage from a ruptured aneurysm of the posterior communicating artery, meningitis, and infiltrative meningeal processes. [4]
Prognosis
The overall prognosis of any oculomotor palsy depends on the etiology. Post-traumatic, post-infectious, post-inflammatory, and ischemic oculomotor palsies may spontaneously recover to a variable degree. [4] Compressive lesions (including aneurysm or tumor) may also improve or resolve after appropriate surgical intervention. [4] Cause notwithstanding, patients with chronic and stable ptosis or ophthalmoplegia due to oculomotor nerve palsy may benefit from reconstructive lid or strabismus surgery over the course of their follow up. [4]
Patient Education
Patients should be informed regarding potentially life-threatening causes of an acquired third cranial nerve palsy, appropriately weighted to the context of their case. Accordingly, they should undergo appropriate evaluation and treatment of their third cranial nerve palsy in a manner that is tailored to their needs. Finally, patients should be provided information that facilitates a good understanding regarding the implications of their diagnosis and prognosis for recovery.
-
Illustration of a complete right oculomotor palsy demonstrating the classic "down and out" appearance, complete ptosis and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
-
Illustration of a partial right oculomotor nerve palsy demonstrating incomplete ptosis, hypotropia and mydriasis of the right eye. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
-
Anatomy of the oculomotor nerve. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
-
Illustration of common causes of an oculomotor nerve palsy. Courtesy of Tyler Henry, MD, Medical Illustrator (tylerhenrymd.com).
Tables
Symptom |
Clinical Relevance |
Nature of Diplopia (Binocular versus Monocular; Horizontal versus Vertical or Oblique) |
Binocular diplopia reflects ocular misalignment whereas monocular diplopia implicates an anterior segment issue, or retinal abnormality. Ask the patient to alternately occlude each eye to localize the nature of the diplopia. |
Directionality |
Third cranial nerve palsies can cause variable patterns of diplopia, and manifestations of horizontal and vertical misalignment will reflect to what extent elevation, adduction, and depression of the eye are impaired. Diplopia is typically worse in the gaze direction of weakest muscle action. |
Intermittent or Constant |
Intermittent diplopia may be gaze directional or reflect a breakdown of binocular fusional control. In the case of a neuromuscular junction mimicking a third cranial nerve palsy, the diplopia may be truly intermittent. |
Associated Symptoms (Pain and Other Systemic Complaints) |
Inflammatory and compressive causes of third cranial nerve palsy may be associated with pain, whereas microvascular ischemic lesions are less commonly painful. Patients older than 50 years may experience third cranial nerve palsies secondary to giant cell arteritis (GCA); therefore, asking about transient vision loss, headache, scalp pain, weight loss, muscle aches, and jaw claudication are important facets of the history to explore so as not to miss this vision-threatening/life threatening diagnosis. |
Onset |
Abrupt onset cranial third nerve palsies suggest a vascular etiology (pituitary apoplexy, subarachnoid hemorrhage) whereas compressive lesions may cause more insidious onset of deficits. |
Progression and Course |
Progressive worsening of third cranial nerve palsies may be seen with compressive lesions. Progressive improvement over weeks to months after acute onset symptomatology (diplopia) may implicate an ischemic cranial nerve palsy. |
Fatigue/Variability |
Prominent fatigue and variability with respect to ptosis and diplopia often implicate a neuromuscular junction abnormality in lieu of a third cranial nerve palsy. |
Other Neurological Manifestations |
Localizing brainstem findings such as a third cranial nerve palsy and contralateral weakness (Weber syndrome) can help localize a midbrain lesion such as stroke, whereas multiple cranial nerve palsies that are slowly progressive can implicate a chronic compressive lesion (aneurysm, meningioma) of the cavernous sinus. Multiple cranial nerve palsies with vision loss in the ipsilateral eye can implicate a lesion of the orbital apex. |
Co-morbidities |
Underlying diagnoses such as diabetes, pituitary macroadenomas, and multiple sclerosis can help localize the cause of third nerve palsies, when known. Systemic conditions such as Grave’s Disease can cause a restrictive orbitopathy which may mimic manifestations of a third cranial nerve palsy. |
Medications |
Some medications such as immune check point inhibitors (inflammatory), vaccinations (inflammatory), tumor necrosis factor alpha inhibitors (demyelinating), and bisphosphonates (inflammatory) may cause manifestations of third nerve palsies or, in the case of restrictive orbital lesions, mimic third nerve palsies. |
Prior Strabismus |
Patients with a prior history of strabismus with or without surgery might be interpreted to have an acquired third nerve palsy if they are symptomatic for loss of fusional control. |
Recurrence |
Patients with a history of what was previously called "ophthalmoplegic migraine" may experience recurrent painful stereotyped third cranial nerve palsies over time. |
Examination Finding |
Clinical Relevance |
Afferent Examination |
|
Visual Acuity |
Evidence of vision loss with a third cranial nerve palsy may implicate a common underlying mechanism such as papilledema, or localize lesions in the sellar region (pituitary apoplexy) or orbital apex. |
Pupils (Efferent and Afferent Functions) |
Evidence of anisocoria, with a mydriatic pupil or tonic pupil with light near dissociation ipsilateral to the third cranial nerve palsy will help localize the lesion; the presence of a concomitant ipsilateral relative afferent pupil defect may implicate a lesion of the orbital apex. |
Color Vision |
Color vision loss disproportionate to high contrast visual acuity deficits may implicate a third cranial nerve palsy and ipsilateral optic neuropathy. |
Fundus Examination |
Evidence of optic atrophy (compressive lesion) or optic disc edema (anterior ischemic optic neuropathy or papilledema) may help localize the lesion or mechanism causing the third cranial nerve palsy. |
Perimetry |
The presence of focal visual deficits ipsilateral to the third cranial nerve palsy might suggest an orbital apex syndrome, whereas enlarged blind spots might implicate raised intracranial pressure with papilledema. A bitemporal defect suggests a lesion of the sellar region (pituitary tumor) with cavernous sinus involvement. |
Efferent Examination |
|
Inspection |
Evidence of ptosis suggests a third cranial nerve palsy. Orbital signs such as proptosis and arterialized conjunctival vessels, might suggest an orbital process mimicking a third nerve palsy due to muscle restriction, including Grave’s Disease, orbital inflammation, orbital infiltration, or a carotid cavernous sinus fistula (CCF). |
Ocular Motility |
An isolated third cranial nerve palsy may cause variable ipsilateral involvement of the superior, inferior, and medial recti muscles and/or inferior oblique muscle. Multiple cranial nerve palsies might indicate lesions of the brainstem, cavernous sinus, skull base, or a more generalized peripheral nerve process such as Miller Fisher Syndrome. |
Aberrant Regeneration |
Signs of aberrant regeneration involving the lid, pupil, and muscles innervated by the third cranial nerve can be seen with chronic compressive lesions in the cavernous sinus, and in the setting of what has previously been called “ophthalmoplegic migraine”. |
Lid Function |
Ipsilateral ptosis is localizing for a third cranial nerve palsy. Weakness of eye closure can be seen with myasthenia gravis and in patients with multiple cranial neuropathies (ie, Miller Fisher Syndrome) |
Fatigue Testing |
Evidence of fatigability and variability (and Cogan’s lid twitch sign) on the examination suggests a neuromuscular junction abnormality. |
Ice Test |
After ice application, improvement of ptosis suggests a disorder of the neuromuscular junction as a possible mimic of a third cranial nerve palsy |
Other |
|
Blood Pressure |
Systemic hypertension may implicate vascular risk factors linked to microvascular ischemic third cranial nerve palsy. |
Syndrome |
Cranial Nerve Involved |
Clinical Pearl |
Cavernous Sinus Syndrome |
CNIII, CNIV, CNV1, CNV1, CNV2 (posterior), sympathetic innervation |
CNII spared |
Orbital Apex Syndrome |
CNII, CNIII, CNIV, CNV1, CNV2, CNVI |
|
Superior Orbital Fissure Syndrome |
CNIII, CNIV, CNV1, CNVI |
CNII spared, CNV2 spared |
Investigation |
Rationale |
Serological Testing |
|
Cell count with differential, hemoglobin AIC, serum sedimentation rate, c-reactive protein, free T3, free T4, TSH, prolactin, FSH, LH, free testosterone, lipid profile, IGF-1, morning cortisol, anti-acetylcholine receptor antibodies, anti-MuSK antibodies, serum lactate, connective tissue screen, genetic testing for mitochondrial disorders and oculopharyngeal muscular dystrophy. |
Serological tests are indicated for suspected cases of diabetic microvascular ischemic cranial nerve palsy, pituitary macroadenomas, giant cell arteritis, myasthenia mimics, and thyroid related eye disease. Chronic progressive external ophthalmoplegia and oculopharyngeal muscular dystrophy can be evaluated with specific genetic testing. |
Cerebrospinal Fluid Analysis |
|
CSF cell count with differential, glucose, protein, cytopathology, gram stain, viral cultures, fungal cultures, and opening pressure as indicated |
CSF analysis can help determine infectious (meningitis), inflammatory (cyto-albuminemic dissociation), malignant, and raised intracranial pressure mechanisms of third cranial nerve palsies. |
Imaging |
|
CT head, cranial and orbital MRI with gadolinium and gadolinium enhanced views, cranial MRI or CT angiography/venography, catheter angiography, CT scan of the chest, whole body PET imaging, orbital ultrasound |
CT imaging is needed acutely in the setting of ICH or hydrocephalus with raised intracranial pressure. CT or MRI with detailed vascular imaging can be used to localize lesions along the fascicle, in the cavernous sinus, in the region of the superior orbital fissure and orbital apices, and orbit. Orbital ultrasound can detect arterialized flow through the superior ophthalmic vein, and help localize cases of CCFs. CT imaging of the chest is needed to check for hilar lymphadenopathy in the case of sarcoid, and thymic hyperplasia/thymoma in suspected MG. Whole body PET CT is useful in detecting inflammatory conditions such as sarcoid and systemic diseases/neoplasms. |
Electrophysiology |
|
Nerve conduction studies (NCS), electromyography (EMG), repetitive nerve stimulation (RNS) studies and single fiber EMG. |
EMG/NCS/SF-EMG and RNS studies can be used to identify cases of neuromuscular junction abnormalities (myasthenia gravis) versus mitochondrial disorders and OPMD. |
Tissue Analysis |
|
Temporal artery biopsy, muscle biopsy, lesion biopsy (pituitary tumors, lesions of the parasellar space and cavernous sinus) |
TAB is needed to confirm a diagnosis of GCA, whereas characteristic findings on muscle biopsy will characterize underlying myopathies. |








