Practice Essentials
Dry eye disease (DED), also known as dry eye syndrome (DES), keratoconjunctivitis sicca (KCS), and keratitis sicca, is a multifactorial disease of the ocular surface due to a loss of homeostasis of the tear film. It often results in ocular symptoms and visual disturbance due to underlying tear film instability, ocular suface inflammation and damage, and neuorsensory abnormalities. [1, 2] Dry eye disease is a common form of ocular surface disease (OSD) and may overlap with other causes of OSD, such as limbal steam cell insufficiency and ocular graft-versus-host disease. [3]
The ocular surface is an integrated anatomical unit consisting of 7 key interactive and interdependent components: the tear film, the lacrimal and accessory lacrimal apparatus, the nasolacrimal drainage system, the eyelids, the bulbar and tarsal conjunctiva, cranial nerve V, and cranial nerve VII. [4] Abnormalities or deficiencies in any of the 7 ocular surface components may worsen dry eye disease, yet promise opportunities for effective therapeutic intervention.
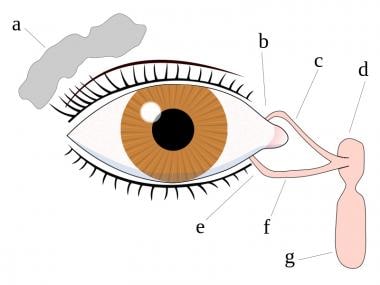 Eye tear system anatomy: a. tear gland / lacrimal gland, b. superior lacrimal punctum, c. superior lacrimal canal, d. tear sac / lacrimal sac, e. inferior lacrimal punctum, f. inferior lacrimal canal, g. nasolacrimal canal.
Eye tear system anatomy: a. tear gland / lacrimal gland, b. superior lacrimal punctum, c. superior lacrimal canal, d. tear sac / lacrimal sac, e. inferior lacrimal punctum, f. inferior lacrimal canal, g. nasolacrimal canal.
Dry eye disease may be subdivided into two non-mutually exclusive types as follows [2] :
Alternatively, dry eye disease can also be subdivided into disease associated with Sjögren syndrome (SS) and disease not associated with SS (non-SS KCS). [1]
Signs and symptoms
While diagnosis of DED does not require for any specific symptom to be present, the following are the most common complaints associated with dry eye disease [1] :
-
Foreign-body, burning, itching, gritty or sandy sensation
-
Hyperemia
-
Mucoid discharge
-
Ocular irritation
-
Excessive tearing (secondary to reflex secretion)
-
Photophobia
-
Blurry vision that may improve with blinking
See Clinical Presentation for more detail.
Diagnosis
Studies that may be used for diagnosis include the following [1] :
-
Vital staining of corneal and conjunctival epithelium with fluorescein, lissamine green, or rose bengal
-
Measurement of tear film osmolarity
-
Detection of ocular surface matrix metalloproteinase 9 (MMP-9)
-
Measurement of tear breakup time (TBUT)
-
The Schirmer test
-
Tear meniscus height
-
Quantification of tear components through analysis of tear proteins
-
Tear meniscometry
-
Impression cytology to monitor progression of ocular surface changes
-
Meibography
-
Tear film interferometry
Additional tests that may be used in a research workup include the following [1] :
-
The tear stability analysis system (TSAS)
-
The tear function index (TFI; Liverpool modification)
-
The tear ferning test (TFT)
Criteria for a diagnosis of dry eye disease associated with Sjögren syndrome (SS) include the following [1] :
-
Abnormally low Schirmer test result
-
Objective evidence of low salivary flow
-
Biopsy-proven lymphocytic infiltration of the labial salivary glands
-
Dysfunction of the immune system, as manifested by the presence of serum autoantibodies (eg, antinuclear antibody [ANA], rheumatoid factor [RF], and anti-Ro [SS-A] and anti-La [SS-B] antibodies)
See Workup for more detail.
Management
Early detection and aggressive treatment of dry eye disease, or keratoconjunctivitis sicca (KCS), may help prevent corneal ulcers and scarring.
Pharmacologic therapy
Lubricating supplements are the medications most commonly used to treat dry eye disease. Agents that have been used to treat dry eye disease include the following [1] :
-
Artificial tear substitutes
-
Gels, emulsions, and ointments
-
Topical or systemic omega-3 fatty acids: Omega-3 fatty acids inhibit the synthesis of lipid mediators and block the production of interleukin (IL)–1 and tumor necrosis factor alpha (TNF-α)
-
Topical or systemic tetracyclines
-
Cholinergic nasal spray such as varenicline nasal spray
-
Topical hyaluronic acid, which also is approved in Japan [12]
-
Autologous or umbilical cord serum
-
Amniotic membrane extract eye drops
-
Eye-platelet rich plasma (E-PRP) drops [13]
-
Systemic immunosuppressants
Various other pharmacologic agents are currently being investigated, including oral lactoferrin, topical lubricin, topical lacritin, and topical thymosin β-4. [14]
In-office procedures
Several in-office procedures are available for the treatment of dry eye disease, including the following [1] :
-
Vectored thermal pulsation (LipiFlow)
-
Meibomian gland probing (Maskin probe or hyfrecator probe)
-
Meibomian gland liquefaction and expression (MiBo ThermoFlo, TearCare System)
-
Intense pulsed light therapy
-
Intranasal tear neurostimulator (TrueTear)
-
Lid-margin scrubbing (BlephEx)
Therapeutic eyewear
Specially made glasses known as moisture chamber spectacles, which wrap around the eyes to retain moisture and protect against irritants, may be helpful in some cases of dry eye disease. Therapeutic contact lenses also may be helpful.
Surgical intervention
Punctal plugs, to achieve either partial or complete punctal occlusion with or without cautery, often are used in the treatment of dry eye disease. [1] Available types include the following:
-
Absorbable plugs
-
Nonabsorbable plugs
-
Thermoplastic plugs
-
Hydrogel plugs
Other advanced or surgical options include the following:
-
Lateral tarsorrhaphy - Temporary tarsorrhaphy (50%) is indicated in patients with exposure keratitis after facial or trigeminal nerve lesions that give rise to dry eye disease secondary to loss of corneal sensation
-
Lid malposition repair (ectropion/entropion repair)
-
Conjunctival flap
-
Conjunctivoplasty - Excision of symptomatic conjunctivochalasis
-
Surgical cautery occlusion of the lacrimal drainage system
-
Mucous membrane grafting
-
Salivary gland duct transposition
-
Limbal stem cell transplantation
-
Amniotic membrane transplantation or amniotic membrane contact lens therapy (eg, ProKera, AmbioDisk)
-
Prosthetic replacement of the ocular surface ecosystem (PROSE) lens therapy
See Treatment and Medication for more detail.
Background
Although dry eye disease may result purely from aqueous tear deficiency or be purely evaporative, it usually is of mixed etiology.
Patients with ADDE may be further differentiated into those with dry eye disease associated with Sjögren syndrome (SS) and those with dry eye disease not associated with SS (non-SS KCS). It is estimated that 10% of patients with ADDE have Sjogren syndrome. Patients are considered to have SS-associated dry eye disease if they have concomitant xerostomia or connective tissue disease (CTD). SS-associated dry eye disease itself is subclassified as either primary SS or secondary SS. Patients with primary SS meet the diagnostic criteria for Sjögren syndrome but do not meet diagnostic criteria for other CTD. Patients with secondary SS have Sjögren-type symptoms that develop in the setting of a diagnosed CTD, most commonly rheumatoid arthritis, systemic lupus erythematosus, psoriatic arthritis, and systemic sclerosis (scleroderma). Patients with SS-related dry eye disease often have more visual difficulty but also have less severe ocular discmofort compared with patients with non-SS KCS. [15] The diagnosis of SS in patients with dry eye patients often is delayed or remains undiagnosed in many patients.
Dry eye disease most frequently is found in women, specifically those who are postmenopausal, are pregnant, are taking oral contraceptives, or are on hormone replacement therapy (especially estrogen-only pills). The common denominator is a decrease in androgens, from either reduced ovarian function (in postmenopausal women) or increased levels of the sex hormone–binding globulin (in women who are pregnant or are taking birth control pills).
Meibomian gland dysfunction is a key component of evaporative dry eye disease, with a growing awareness among clinicians of the key role played by surface lipids. In Lemp et al’s cohort of 224 subjects with dry eye disease, 86% demonstrated signs of meibomian gland dysfunction based on an objective, composite, disease severity scale. The proportion of subjects exhibiting signs of evaporative dry eye resulting from meibomian gland dysfunction far outweighs that of subjects with pure aqueous deficiency dry eye in that general clinic-based patient cohort. [16]
Dry eye disease essentially is a clinical diagnosis made by combining information obtained from the history and physical examination by performing one or more tests to lend some objectivity to the diagnosis. No single test is sufficiently specific to permit an absolute diagnosis of dry eye disease, and the entire clinical context is needed to make an appropriate treatment recommendation.
Early detection and aggressive treatment of dry eye disease may help prevent corneal ulcers and scarring, as well as improve quality of life metrics. Treatment depends on the level of severity and may include medications, eye protection devices, and surgical interventions. The frequency of follow-up care depends on the severity of the signs and symptoms. Environment-related issues that may exacerbate dry eye disease should be discussed; alternatives may be needed.
Anatomy
The tear film covers the normal ocular surface that protects the cornea. The previous model of a 3-layer model of lipid, aqueous, and mucin layer now has been replaced with a 2-phase model of the tear film as described below [17] :
-
A superficial thin lipid layer (42nm) - This layer is produced by the meibomian glands and the sebaceous gland of Zeis, and its principal function is to retard tear evaporation and to assist in uniform tear spreading [18]
-
A mucoaqueous layer (3 µm) - This layer has 2 components - the aqueous component and the mucin component. The aqeous component is secreted by the main lacrimal gland (reflex tearing) and accessory lacrimal glands of Krause and Wolfring (basic tearing). The mucin component is secreted by conjunctival goblet cells and associates itself with ocular surface via its loose attachments to the glycocalyx of the microplicae of the epithelium. The hydrophilic quality of the secreted mucin and membrane-spanning mucins, which are expressed by conjunctival and corneal epithelium cells, also help spread the tear film across the ocular surface. The mucoaqueous layer primarily serves a lubricating function, and ensures an even and spontaneous distribution of the tear film across the ocular surface. It also provides an antimicrobial defense and transmits oxygen to the avascular corneal epithelium.
The lipid layer acts as a surfactant, constitutes an aqueous barrier, retards evaporation of the underlying aqueous layer, and provides a smooth optical surface. It may also act as a barrier against foreign particles, and it may possess some antimicrobial properties.
Because the meibomian glands are holocrine in nature, the secretions contain both polar lipids (aqueous-lipid interface) and nonpolar lipids (air-tear interface), as well as proteinaceous material. All of these are held together by ionic bonds, hydrogen bonds, and van der Waals forces. The secretions are subject to neuronal (parasympathetic, sympathetic, and sensory sources), hormonal (androgen and estrogen receptors), and vascular regulation. Evaporative loss is predominantly due to meibomian gland dysfunction (MGD).
The aqueous component of the mucoaqueous layer includes about 60 different proteins, electrolytes, and water from the lacrimal gland, conjunctiva, and meibomian gland. Lysozyme, the most abundant (20-40% of total protein) and most alkaline of the tear proteins, is a glycolytic enzyme capable of breaking down bacterial cell walls. Lactoferrin has antibacterial and antioxidant functions, and epidermal growth factor (EGF) helps maintain the normal ocular surface and promote corneal wound healing. Other components include albumin, transferrin, immunoglobulin A (IgA), immunoglobulin M (IgM), and immunoglobulin G (IgG).
The secretion of the lacrimal gland is controlled by a neural reflex arc, with afferent nerves (trigeminal sensory fibers) in the cornea and the conjunctiva passing to the pons (superior salivary nucleus), from which efferent fibers pass in the nervus intermedius to the pterygopalatine ganglion and postganglionic sympathetic and parasympathetic nerves terminating in the lacrimal glands.
The glycocalyx of the corneal epithelium contains the transmembrane mucins (glycosylated glycoproteins present in the glycocalyx) MUC1, MUC4, and MUC16. These membrane mucins interact with soluble, secreted, gel-forming mucins produced by the goblet cells (MUC5AC) and also with others, such as MUC2. The lacrimal gland also secretes MUC7 into the tear film.
These soluble mucins move about freely in the tear film, a process facilitated by blinking and electrostatic repulsion from the negatively charged transmembrane mucins. Soluble mucins also function as cleanup proteins by picking up dirt, debris, and pathogens, holding fluids because of their hydrophilic nature, and harboring defense molecules produced by the lacrimal gland.
Transmembrane mucins prevent pathogen adherence and entrance. They also provide a smooth lubricating surface, allowing lid epithelia to glide over corneal epithelia with minimal friction during blinking and other eye movements. It has been suggested that the mucins are mixed throughout the aqueous layer of tears owing to their hydrophilic nature and, being soluble, move freely within this layer.
Pathophysiology
Tear hyperosmolarity and instabiliy are the principal components of the primary drivers of dry eye disease. [2] The 2 major types of DED, aqueous deficient dry eyes (ADDE) and evaporative dry eyes (EDE), can both be related to tear hyperosmolarity and instability.
-
In EDE, tear film lipid deficiency from meibomian gland dysfunction results in excessive evaporation of the tear film. This leads to tear hyperosmolarity in the presence of normal lacrimal function.
-
In ADDE, reduced tear secretion from the lacrimal glands due to lacrimal gland damage (for exmaple, in Sjögren disease) leads to the hyperosmolarity of the tear film despite a normal evaporation rate of the tear film.
Both EDE and ADDE often co-exist and contribute to the mixed type of dry eye disease. Tear hyperosmolarity, which is present in both EDE and ADDE, eventually enters into a vicious cycle that leads to chronic inflammation, loss of conjunctival goblet cells, ocular surface damage, and self-perpetuating disease. [19]
Proinflammatory Activity
Various proinflammatory cytokines that may cause cellular destruction, including interleukin (IL)–1, IL-6, IL-8, TGF-β, tumor necrosis factor alpha (TNF-α), and chemokine ligand 5 (CCL5 or RANTES), are altered in patients with dry eye disease. IL-1β and TNF-α, which are present in the tears of patients with dry eye disease, cause the release of opioids that bind to opioid receptors on neural membranes and inhibit neurotransmitter release through production of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB).
IL-2 also binds to the delta opioid receptor and inhibits cAMP production and neuronal function. This loss of neuronal function diminishes normal neuronal tone, leading to sensory isolation of the lacrimal gland and eventual atrophy.
Proinflammatory neurotransmitters, such as substance P and calcitonin gene–related peptide (CGRP), are released, and these substances recruit and activate local lymphocytes. Studies suggest that dry eye severity is directly correlated with nerve growth factor (NGF) levels and inversely correlated with CGRP and neuropeptide Y (NPY) tear levels.
NGF tear levels point to a direct relation with conjunctival hyperemia and fluorescein staining results, suggesting that tear levels of NGF are more closely connected to corneal epithelial damage, perhaps as a reflection of attempted compensatory repair responses, and that the decreased tear levels of NPY and CGRP in dry eye disease are linked to impaired lacrimal function. [20] In one study, elevated NGF tear levels were decreased by giving 0.1% prednisolone. [21]
Substance P also acts via the nuclear factor of activated T cells (NF-AT) and through the NF-κB signaling pathway. This leads to expression of intercellular adhesion molecule 1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1), adhesion molecules that promote lymphocyte homing and chemotaxis to sites of inflammation.
Inflammatory cytokines, in addition to inhibiting neural function, also may convert androgens into estrogens, resulting in meibomian gland dysfunction. An increased rate of apoptosis also is seen in conjunctival and lacrimal acinar cells, perhaps owing to the cytokine cascade. Elevated levels of tissue-degrading enzymes called matrix metalloproteinases (MMPs) also are present in the epithelial cells.
Mucin deficiency
Mucin-synthesizing genes representing both transmembrane mucins and goblet cell–secreted soluble mucins have been isolated and designated MUC1 through MUC17. Their roles in hydration and stabilization of the tear film are being investigated in patients with KCS. Particularly significant is MUC5AC, which is expressed by stratified squamous cells of the conjunctiva and whose product is the predominant component of the mucous layer of tears. A defect in this and other mucin genes may be a factor in the development of dry eye disease.
Besides dry eye disease, other conditions may eventually lead to loss of goblet cells, including ocular cicatricial pemphigoid, Stevens-Johnson syndrome, and vitamin A deficiency. These conditions may lead to drying and eventual keratinization of the ocular epithelium. Both classes of mucins are decreased in these diseases, and, on a molecular level, mucin gene expression, translation, and posttranslational processing are altered.
Mucin deficiency leads to poor wetting of the corneal surface with subsequent desiccation and epithelial damage, even in the presence of adequate aqueous tear production.
Reduced tear protein production
Normal production of tear proteins, such as lysozyme, lactoferrin, lipocalin, and phospholipase A2, is decreased in dry eye disease.
Lipocalins, previously known as tear-specific prealbumin, are inducible lipid-binding proteins produced by the lacrimal glands and are present in the mucous layer. They lower the surface tension of normal tears, which provides stability to the tear film and also explains the increase in surface tension seen in dry eye disease characterized by lacrimal gland deficiency. Lipocalin deficiency can lead to precipitation in the tear film, forming the characteristic mucous strands seen in patients with dry eye symptoms.
Sex Hormone Deficiency
Androgens are believed to be trophic for the lacrimal and meibomian glands. They exert potent anti-inflammatory activity via production of transforming growth factor–beta (TGF-β), suppressing lymphocytic infiltration.
Both androgen and estrogen receptors are located in the lacrimal and meibomian glands. At menopause, a decrease in circulating sex hormones occurs, possibly affecting the functional and secretory aspect of the lacrimal gland. Initial interest in this area centered on evaluating estrogen or progesterone deficiency, and was done to explain the link between dry eye disease and menopause whereas subsequent research has tended to focus more on androgens (specifically, testosterone) or metabolites of androgens. [22, 23] A 2017 randomized, controlled trial of 46 androgen-deficient patients showed that those treated with androgen replacement had statistically significant improvements in tear breakup time, corneal staining, Schirmer scores, and Ocular Surface Disease Index (OSDI) scores at 4 weeks compared with those receiving placebo. [24]
In meibomian gland dysfunction, androgen deficiency results in loss of the lipid layer—specifically, loss of triglycerides, cholesterol, monounsaturated essential fatty acids such as oleic acid, and polar lipids, including phosphatidylethanolamine and sphingomyelin. Loss of polar lipids, which are present at the aqueous-tear interface, exacerbates evaporative tear loss, and loss of unsaturated fatty acids raises the melting point of meibomian gland secretions, or meibum, leading to thicker, more viscous secretions that obstruct ductules and cause stagnation of secretions.
Patients on antiandrogenic therapy for prostate disease also have increased viscosity of meibum, decreased tear breakup time (TBUT), and increased tear film debris, all of which indicate a deficient or abnormal tear film.
SS-Associated Dry Eye Disease (Primary or Secondary)
SS-associated dry eye disease leads to a chronic inflammatory state, with the production of autoantibodies, including antinuclear antibody (ANA), rheumatoid factor (RF), fodrin (a cytoskeletal protein), the muscarinic M3 receptor, or SS-specific antibodies (eg, anti-RO [SS-A] and anti-LA [SS-B]); inflammatory cytokine release; and focal lymphocytic infiltration of the lacrimal and salivary gland, with glandular degeneration and induction of apoptosis in the conjunctiva and lacrimal glands. The lymphocytic infiltrates consist mainly of CD4+ T cells but also B cells.
This results in dysfunction of the lacrimal gland with reduced tear production, as well as loss of response to nerve stimulation and less reflex tearing. Active T-lymphocytic infiltrate in the conjunctiva has also been reported in non-SS dry eye disease.
Etiology
The International Dry Eye WorkShop II (DEWS II) classifies dry eye disease as the following 2 major subtypes:
-
Aqueous deficient dry eye (ADDE)
-
Evaporative dry eye (EDE)
Etiology: Aqueous Deficient Dry Eye (ADDE)
Causes of deficient aqueous production can further be classified as related or unrelated to SS.
Non-Sjögren syndrome
Primary lacrimal gland deficiencies that may impair aqueous production include the following:
-
Idiopathic
-
Age-related dry eye
-
Congenital alacrima (eg, Riley-Day syndrome)
-
Familial dysautonomia
Secondary lacrimal gland deficiencies that may impair aqueous production include the following:
-
Lacrimal gland infiltration
-
Sarcoidosis
-
Lymphoma
-
AIDS
-
Amyloidosis
-
Hemochromatosis
-
Lacrimal gland infectious diseases
-
HIV diffuse infiltrative lymphadenopathy syndrome
-
Trachoma
-
Systemic vitamin A deficiency (xerophthalmia) – Malnutrition, fat-free diets, intestinal malabsorption from inflammatory bowel disease, bowel resection, or chronic alcoholism
-
Lacrimal gland ablation
-
Lacrimal gland denervation
-
IgG-4 disease with ocular involvement
Lacrimal obstructive diseases that may impair aqueous production include the following:
-
Trachoma
-
Ocular cicatricial pemphigoid
-
Stevens-Johnson syndrome/toxic epidermal necrolysis
-
Chemical and thermal burns
-
Endocrine imbalance
-
Post-irradiation fibrosis
-
Ocular graft-versus-host disease
Medications that may impair aqueous production include the following:
-
Antihistamines
-
Beta blockers
-
Phenothiazines
-
Atropine
-
Oral contraceptives
-
Anxiolytics
-
Antiparkinsonian agents
-
Diuretics
-
Anticholinergics
-
Antiarrhythmics
-
Topical preservatives in eye drops (eg, benzalkonium chloride [BAK], thimerosal)
-
Topical anesthetics
-
Isotretinoin
The following conditions may lead to reflex hyposecretion:
-
Neurotrophic keratitis – Cranial nerve (CN) V/ganglion section/injection/compression
-
Corneal surgery - Limbal incision (eg, extracapsular cataract extraction), keratoplasty, and refractive surgery
-
Infective - Herpes simplex keratitis and herpes zoster ophthalmicus
-
Topical agents - Topical anesthesia
-
Systemic medications – Beta blockers and atropine-like drugs
-
Chronic contact lens wear
-
Diabetes
-
Aging
-
Trichloroethylene toxicity
-
CN VII damage
Sjögren syndrome
Primary SS has no associated CTD.
Secondary SS may be associated with any of the following CTDs:
-
Rheumatoid arthritis
-
Systemic lupus erythematosus
-
Progressive systemic sclerosis (scleroderma)
-
Psoriatic arthritis
-
Primary biliary cirrhosis
-
Interstitial nephritis
-
Polymyositis
-
Dermatomyositis
-
Granulomatosis with polyangiitis (formerly Wegener granulomatosis)
-
Polyarteritis nodosa
-
Hashimoto thyroiditis
-
Lymphocytic interstitial pneumonitis
-
Idiopathic thrombocytopenic purpura
-
Hypergammaglobulinemia
-
Waldenstrom macroglobulinemia
Etiology: Evaporative Dry Eye (EDE)
Intrinsic causes
Meibomian gland disease may involve a reduced number of functioning glands, as in congenital deficiency or acquired meibomian gland dysfunction, or complete gland replacement, as in distichiasis, lymphedema-distichiasis syndrome, or metaplasia. Meibomian gland dysfunction may be divided into 3 subtypes, as follows:
-
Hypersecretory - Meibomian seborrhea
-
Hyposecretory - Isotretinoin therapy
-
Obstructive - This may be simple, primary, or secondary to local disease (eg, anterior blepharitis), systemic disease (eg, acne rosacea, seborrheic dermatitis, atopy, ichthyosis, or psoriasis), syndromes (eg, anhidrotic ectodermal dysplasia, ectrodactyly syndrome, or Turner syndrome), or systemic toxicity (eg, 13- cis retinoic acid or polychlorinated biphenyls); or it may be cicatricial, primary or secondary to local disease (eg, chemical burns, trachoma, pemphigoid, erythema multiforme, acne rosacea, vernal keratoconjunctivitis [VKC], or atopic keratoconjunctivitis [AKC])
Evaporative loss may result from a low blink rate caused by the following:
-
Physiologic phenomenon, such as may occur during performance of tasks that require concentration (eg, working at a computer or a microscope)
-
Extrapyramidal disorder, such as Parkinson disease (decreasing dopaminergic neuron pool)
Evaporative loss may result from the following disorders of eyelid aperture and eyelid-globe congruity:
-
Exposure (eg, craniosynostosis, proptosis, exophthalmos, lagaophthalmos, and high myopia)
-
Lid palsy
-
Eyelid malposition (eg, ectropion, entropion, floppy eyelid syndrome)
-
Lid margin abnormality (eg, lid margin coloboma)
In addition, the actions of drugs such as isotretinoin may lead to evaporative loss.
Extrinsic causes
Vitamin A deficiency may cause dry eye as a consequence of the following:
-
Development disorder of goblet cells
-
Lacrimal acinar damage
Other extrinsic causes of dry eye are as follows:
-
Topical drugs and preservatives that cause surface epithelial cell damage
-
Contact lens wear
-
Ocular surface disease (eg, atopic keratoconjunctivitis, chronic anterior blepharitis, chronic conjunctivitis, ocular cicatricial pemphigoid, Stevens-Johnson syndrome)
Epidemiology
Dry eye disease is very common in the United States, affecting a significant percentage of the population, especially those older than 50 years. Prevalence estimates range from 10-30%. An estimated 3.23 million women and 1.68 million men aged 50 years and older are affected. [25, 26] The prevalence of dry eye disease also is increasing among young adults aged 18-34 years, mostly owing to increased use of soft contact lenses and frequent smartphone and computer usage. [27]
Dry eye disease is one of the most common reasons for a patient to seek eye care. [28] Furthermore, its widespread prevalence has created a significant socioeconomic burden on the United States healthcare system. Lost productivity through missed work days, the rising cost of treatment, and the social and emotional stressors encountered by patients with dry eye disease are notable. [29]
As a consequence of the demographic pressure created by an aging population, meibomian gland dysfunction is expected to increase in prevalence and thus to impose a growing burden on ophthalmologic practices. [30] Development of thoughtful, effective strategies that involve the underlying mechanism of meibomian gland dysfunction is critical to the effective, patient-satisfying functioning of every ophthalmologist’s practice.
The reported frequency of dry eye in other countries closely parallels that in the United States.
Dry eye is more common in women. [25] Dry eye disease associated with SS is believed to affect 1-2% of the population, and 90% of those affected are women. Data on race and ethnicity in dry eye disease are limited, but the frequency and the clinical diagnosis of dry eye appear to be greater in the Hispanic and Asian populations than in whites.
Prognosis
The prognosis of dry eye disease varies depending on the severity of the condition. Most patients have mild-to-moderate cases that can be treated symptomatically with lubricants, often providing adequate relief of symptoms. More severe cases may require surgical management such as punctal occlusion or correcting eyelid malposition. In general, the prognosis for visual acuity in patients with dry eye disease is good. Patients with SS or prolonged untreated dry eye represent a subgroup with a worse prognosis, requiring a longer course of treatment.
Dry eye may be complicated by sterile or infectious corneal ulceration, particularly in patients with SS. Ulcers are typically circular central or paracentral corneal lesions that are smaller than 3 mm in diameter. Occasionally, corneal perforation may occur. In rare cases, sterile or infectious corneal ulceration in dry eye disease can cause blindness. This risk is markedly increased with contact lens use, particularly with overnight wear.
Punctate epithelial defects (PEDs) may be present. Significant punctate epitheliopathy can lead to corneal erosions, both sterile and infectious corneal ulceration, corneal neovascularization, corneal scarring, corneal thinning, and even corneal perforation.`
Patient Education
A wide variety of educational materials is available for patients with dry eye disease, particularly online. For patients with SS, regular dental examinations are important because dry mouth or xerostomia, a component of SS, significantly increases the risk for dental problems. Women should receive regular checkups from their gynecologists.
Patients with SS can obtain up-to-date information from the Sjögren’s Syndrome Foundation, 6707 Democracy Boulevard, Suite 325, Bethesda, MD 20817; (301) 530-4420 or (800) 475-6473; fax, (301) 530-4415.
For patient education information, see the Eye and Vision Center, as well as Dry Eye Syndrome, Pink Eye, How to Instill Your Eyedrops, and Sjögren’s Syndrome. Other resources include the National Eye Insitute Fact page about dry eyes and the Sjögren Foundation. See also the following topics:
-
Eye tear system anatomy: a. tear gland / lacrimal gland, b. superior lacrimal punctum, c. superior lacrimal canal, d. tear sac / lacrimal sac, e. inferior lacrimal punctum, f. inferior lacrimal canal, g. nasolacrimal canal.
Tables
Variable |
Dry Eye Severity Level |
|||
1 |
2 |
3 |
4 (must have signs and symptoms) |
|
Discomfort (severity and frequency) |
Mild, episodic; occurs under environmental stress |
Moderate, episodic or chronic; occurs with or without stress |
Severe, frequent, or constant; occurs without stress |
Severe or disabling, constant |
Visual symptoms |
None or episodic mild fatigue |
Annoying or activity-limiting, episodic |
Annoying, chronic, or constant; activity-limiting |
Constant and possibly disabling |
Conjunctival injection |
None to mild |
None to mild |
+/– |
+/++ |
Conjunctival staining |
None to mild |
Variable |
Moderate to marked |
Marked |
Corneal staining (severity and location) |
None to mild |
Variable |
Marked central |
Severe punctate erosions |
Corneal and tear signs |
None to mild |
Mild debris, decreased meniscus |
Filamentary keratitis, mucus clumping, increased tear debris |
Filamentary keratitis, mucus clumping, increased tear debris, ulceration |
Lid and meibomian glands |
MGD variably present |
MGD variably present |
MGD frequent |
Trichiasis, keratinization, symblepharon |
Tear breakup time |
Variable |
≤ 10 s |
≤ 5 s |
Immediate |
Schirmer score |
Variable |
≤ 10 mm/5 min |
≤ 5 mm/5 min |
≤ 2 mm/5 min |
MGD=meibomian gland dysfunction. |
||||





