Background
Recurrent corneal erosion (RCE) syndrome is a condition that is characterized by a disturbance at the level of the corneal epithelial basement membrane, resulting in defective adhesions and recurrent breakdowns of the epithelium.
RCE syndrome may occur secondary to corneal injury or spontaneously. In the latter case, some predisposing factor, such as diabetes or a corneal dystrophy, may be the underlying cause. Management of RCE syndrome is usually aimed at regenerating or repairing the epithelial basement membrane to restore the adhesion between the epithelium and the anterior stroma.
Corneal erosions are perhaps one of the most common and neglected ocular disorders. Some of these cases occur after ocular trauma, but most of them occur spontaneously. Painful RCE syndrome, whether due to trauma or to anterior basement membrane dystrophy (Cogan dystrophy or map-dot-fingerprint dystrophy), results from abnormalities in the epithelial basement membrane.
Manifestation
Recurrent corneal erosions and epithelial basement membrane dystrophy are usually bilateral and are characterized by various patterns of dots, parallel lines that mimic fingerprints, and patterns that resemble maps, which appear in the epithelium. Individual microcysts may be oval, oblong, or comma-shaped and rarely appear alone but usually are associated with map and fingerprint patterns. On the other hand, the map and fingerprint patterns appear without dots or individual microcysts.
Map and fingerprint alterations of the corneal epithelium are not rare and can be found in asymptomatic individuals without prior history of trauma or ocular disease. Literature suggests that these epithelial changes are more common than previously recognized. They frequently are seen in conditions involving corneal edema, such as near a healing cataract surgery incision, or in the center of the cornea associated with Fuchs corneal dystrophy.
Clinical manifestations of Fuchs dystrophy
Three stages of Fuchs endothelial dystrophy are recognized. The 3 stages usually evolve gradually over a period of 25 years, and, like other corneal dystrophies, they usually are bilateral but asymmetric.
The first stage is the onset of cornea guttata, usually in the fourth decade of life. Subjective symptoms rarely occur until the fifth or sixth decade. During the asymptomatic phase, endothelial guttata and pigment dusting can be seen by slit lamp examination of the central corneal endothelium and by specular reflection. The guttate excrescences can become more numerous and confluent so that individual guttata are lost completely in the beaten-metal appearance of the endothelial surface. The central cornea is involved first, and, as the disease progresses, it spreads toward the periphery.
In the second phase of the disease, blurred vision, glare, and halos around lights develop because of incipient corneal edema in the stroma and epithelium. Epithelial edema can be seen as small droplets (bedewing) on retroillumination with the slit lamp. Epithelial microcysts coalesce to form bullae, which produce varying amounts of pain when they burst; hence, the name bullous keratopathy. Striae form in the Descemet membrane as the cornea thickens posteriorly due to stromal swelling. The arc of the Descemet membrane from limbus to limbus is shortened, causing wrinkles in the Descemet membrane called striae. The microcystic epithelial vesicles may break, causing foreign body sensations and severe pain with more extensive corneal epithelial disruption.
In the third stage, recurrent corneal erosions, microbial ulceration, and persistent pain may occur. Corneal sensitivity usually is reduced.
Pathophysiology
The 2 categories of corneal abrasions are as follows: superficial (those not involving the Bowman layer) and deep (those that penetrate the Bowman layer but do not rupture the Descemet membrane). Corneal abrasions may result from foreign bodies, contact lenses, chemicals, fingernails, hair brushes, tree branches, and dust.
The cornea has remarkable healing properties. The epithelium adjacent to any insult expands in size to fill in the defect, usually within 24-48 hours. Lesions that are purely epithelial often heal quickly and completely without scarring. Lesions that extend below the Bowman layer are more likely to leave a permanent scar.
The epithelial healing process begins when basal epithelial cells undergo mitosis, producing new cells that occupy fresh wounds. Basal cells adhere the epithelium to the stroma in 2 ways: they secrete the basement membrane, and they contain hemidesmosomes, which are essentially linchpins that protrude through the posterior surface of basal cells and into the stroma; each is held in place by an anchoring fibril. Any disruption to basal cell production makes the eye more prone to recurrent erosion.
Recurrent corneal erosions occur because there is a defect in the epithelial basement membrane and in hemidesmosomes formation, resulting in epithelial loss, microcysts, and bullae.
Recurrent corneal erosions occurring after injury or any corneal insult result because of improper or inadequate healing of the basement membrane, either because the basal epithelial cells fail to produce proper basement membrane complexes to attach to the Bowman layer and stroma or because of faulty basement membrane adherence.
A traumatic cause has a better eventual prognosis for full recovery than does the spontaneous form. In the case of spontaneous corneal erosions, the underlying disease process may be an epithelial basement membrane corneal dystrophy. Studies with the electron microscope have shown that during recurrent corneal erosion episodes, there is separation of the anchoring system at the level of the epithelial cell membrane or below the level of the anchoring plaques. Normal and degenerate polymorphonuclear leucocytes (PMNs) were found within and between the epithelial cells and within the anchoring layer. The degenerate PMNs may secrete metalloproteinases that cleave the Bowman layer below the anchoring system.
Epidemiology
Frequency
United States
Recurrent corneal erosions are quite frequent in developing countries where lack of proper nutrition plays a significant role in the health of the cornea. Moreover, they are more frequent in patients with the predisposing factors and in those patients that have associated skin problems (see Causes).
Mortality/Morbidity
The tendency for epithelial basement membrane dystrophy, recurrent erosion, or both is probably hereditary, with variable penetrance. If corneal erosions are inherited, the pattern is dominant; however, most corneal erosions are acquired. In a study by Laibson, it has been found that 6% of the patients treated for a variety of other ocular conditions and diseases also demonstrated map, dot, and fingerprint changes in the epithelium. [1]
A recurrent corneal erosion is most likely to develop in a person who has had a previous corneal abrasion that was very sharp, clean, and linear, like that from a paper cut. Because the cut is so sharp, without ragged edges, it is less likely to stick down tightly to the underlying basement membrane. Those who have an abnormal structure to the corneal epithelium (called map-dot-fingerprint dystrophy) are at a much greater risk for poor healing following a corneal abrasion and, thus, can develop a recurrent corneal erosion.
Just as it is nearly impossible to see a corneal abrasion with the naked eye, the same is true for a recurrent corneal erosion. The time course is most important. In a recurrent corneal erosion, the patient can remember having had a corneal abrasion relatively recently (usually within the past 3–10 d) and then most often when first opening the eye in the morning.
Sex
Recurrent corneal erosions usually are seen as a bilateral problem occurring somewhat more frequently in females than in males. The epithelium may show a slipped-rug appearance; filaments are often seen. The recurrent erosions may occur over multiple sites on the cornea, a situation different from traumatic erosions.
Age
Recurrent corneal erosions and epithelial basement membrane dystrophy occur in adults, usually after the fourth decade of life. However, there are studies that have associated recurrent corneal erosions with juvenile Alport syndrome, which is an X-linked condition that also presents with anterior lenticonus and retinal flecks, as well as renal complications. Certain anterior corneal dystrophies, such as Reis-Bücklers, and lattice dystrophies can cause painful recurrent erosions in children.
Prognosis
Overall, the prognosis is very good to excellent with proper attention. Unless there is an ongoing underlying corneal disease, most patients will ultimately heal completely and not have any more episodes; however, the healing process may take years.
While most patients respond to medical treatment, surgical treatment in the form of anterior stromal puncture (especially in localized posttraumatic erosions), epithelial debridement, diamond burr polishing of the Bowman layer, or excimer laser phototherapeutic keratectomy have excellent success rates, and they should not be used as last resort but rather a next step in the treatment regimen.
Patient Education
Patients should be instructed to take very good care of their eyes. Once corneal erosion develops, although it can be treated, there is no guarantee that it will not recur. Therefore, patients should always wear protective sunglasses when the sun is out and always use lubricating eye drops.
Precautionary measures for patients with recurrent corneal erosion associated with epithelial basement membrane dystrophy include the following:
-
Avoidance of rubbing the eyes through the eyelids
-
Liberal use of ointment medications at bedtime during an erosion episode
-
Sometimes these measures must be performed for several months after resolution of the episode.
Educate patients on how to open the eyes upon awakening (see Deterrence/Prevention).
-
Corneal abrasion.
-
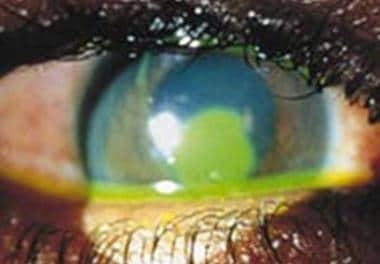
Recurrent corneal erosion.
-
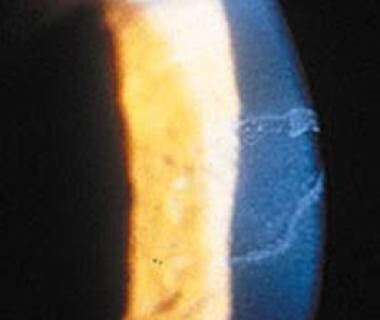
Recurrent erosion with fluorescein in an area of staining.
-
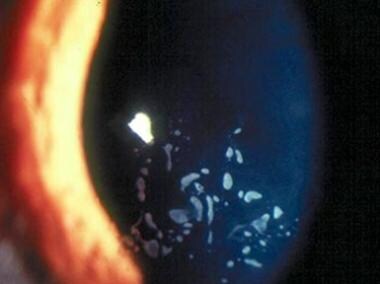
Map-dot-fingerprint dystrophy.
-
Stromal puncture seen with fluorescein.
-
Direct view with a slit lamp.
-
Debriding of the epithelium. Poorly adherent epithelium with a second layer of basement membrane.
-
Granular dystrophy before phototherapeutic keratectomy.
-
Granular dystrophy after photorefractive keratectomy.

