Practice Essentials
Most people fully recover from minor corneal abrasions without permanent eye damage. However, deeper scratches can lead to corneal infections, corneal erosion, or scarring of the cornea. If not treated properly, these complications can result in long-term vision problems. Any unusual symptoms, including a recurrence of pain following healing, should be reported to your eye doctor.
Background
Corneal abrasion is probably the most common eye injury and perhaps one of the most neglected. It occurs because of a disruption in the integrity of the corneal epithelium or because the corneal surface is scraped away or denuded as a result of physical external forces. Corneal epithelial abrasions can be small or large.

Corneal abrasions usually heal rapidly, without serious sequelae. Consequently, they often are considered of little consequence. However, deeper corneal involvement, infection, or poor healing may result in irregularity of the corneal epithelium or scar formation within the stroma.
Corneal abrasions occur in any situation that causes epithelial compromise. Examples include corneal or epithelial disease (eg, dry eye), superficial corneal injury or ocular injuries (eg, those due to foreign bodies), exposure to ultraviolet light, and contact lens wear (eg, daily disposable soft lenses, extended-wear soft lenses, gas-permeable lenses, hard polymethylmethacrylate lenses). [1] Spontaneous corneal abrasions may be associated with map-dot-fingerprint dystrophy or recurrent corneal erosion syndrome.
A traumatic corneal abrasion is the classic corneal abrasion in which mechanical trauma to the eye results in a defect in the epithelial surface. Common causes of traumatic corneal abrasions include the following [1] :
-
Fingernails
-
Animal paws
-
Pieces of paper or cardboard
-
Makeup applicators
-
Hand tools
-
Branches or leaves
-
Thermal burns and ultraviolet light burns
Foreign body–related abrasions are defects in the corneal epithelium that result from removal or spontaneous dislodgement of a corneal foreign body. Foreign body abrasions typically are caused by pieces of metal, wood, glass, plastic, fiberglass, or vegetable material that have become embedded in the cornea or adherent to the inner surface of the upper lid.
Contact lens–related abrasions are defects in the corneal epithelium that are left behind after the removal of an overworn, improperly fitting, or improperly cleaned contact lens. In these cases, the mechanical insult is not from external trauma but rather from a foreign body that may be associated with specific pathogens.
Spontaneous defects in the corneal epithelium may occur with no immediate antecedent injury or foreign body. Eyes that have suffered a previous traumatic abrasion or eyes that have an underlying abnormality of the corneal epithelium are prone to this problem.
The diagnosis of corneal abrasion can be confirmed with slitlamp examination and fluorescein instillation (see Workup). Prophylactic topical antibiotics are given in patients with abrasions from contact lenses, who are at increased risk for infected corneal ulcers, but many emergency physicians have stopped using these agents for minor injuries. Patching the eye is a traditional measure, but it is not supported by research and should not be performed in patients at high risk for eye infection. Pain relief is important. (See Treatment.)
For patient education information, see the Eye and Vision Center, as well as Corneal Abrasion; Foreign Body, Eye; and Eye Injuries.
Anatomy
The cornea is a transparent tissue over the anterior part of the eye that serves several purposes: protection, refraction, and filtration of some ultraviolet light. It has no blood vessels and receives nutrients through tears as well as from the aqueous humor. It has sensory innervation from the ophthalmic division of the trigeminal nerve.
The cornea is composed of the following 5 layers (anterior to posterior):
-
Corneal epithelium
-
Bowman layer
-
Corneal stroma
-
Descemet membrane
-
Corneal endothelium
Pathophysiology
A corneal abrasion is a defect in the surface of the cornea that is limited to the most superficial layer, the epithelium, and does not penetrate the Bowman membrane. In some cases, the bulbar conjunctiva is also involved. Corneal abrasions result from physical or chemical trauma. [1] Severe corneal injuries can also involve the deeper, thicker stromal layer; in this situation, the term partial-thickness corneal laceration may be used.
The conjunctival response to corneal wounding has been known since 1944, when Mann first observed that peripheral corneal abrasions heal by the sliding of limbal cells to cover the epithelial defect. [2] This response is split into 2 phases: (1) the response of the limbal epithelium, which is the source of the new corneal epithelial stem cells, and (2) the response of the conjunctival epithelium itself. [1]
Under normal circumstances, the limbal epithelium acts as a barrier and exerts an inhibitory growth pressure that prevents the migration of conjunctival epithelial cells onto the cornea. Like the rest of the surface of the body, the conjunctiva and the cornea are in a constant state of turnover. Corneal epithelial cells are continuously shed into the tear pool, and they are simultaneously replenished by cells moving centrally from the limbus and anteriorly from the basal layer of the epithelium.
Movement from the basal to superficial layers is relatively rapid, requiring 7-10 days. However, movement from the limbus to the center of the cornea is slow and may require months.
This normal physiologic process is exaggerated in the case of a corneal abrasion. During corneal healing of a lesion, corneal epithelial cells become flattened, spread, and move across the defect until they cover it completely. Cellular proliferation, which is independent of cell migration, begins approximately 24 hours after injury.
Stem cells from the limbus also respond by proliferating to give rise to daughter cells called transient amplifying cells. These cells migrate to heal the corneal defect and proliferate to replenish the wounded area. The observation of limbal pigment migrating onto the clear cornea provides additional evidence of this process.
The concept that the limbal cells form a barrier to conjunctival cells was supported further by the observation that rabbit eyes treated for 120 seconds with N -heptanal, which removed the corneal and conjunctival epithelium but left the limbal basal cells intact, resulted in healing of the corneal epithelium together with unvascularized corneas. However, when the entire limbal zone was surgically removed along with N -heptanal treatment, corneal vascularization and conjunctivalization was observed. [3]
Demonstration of the centripetal migration of limbal cells (marked by India ink) provided more direct evidence of this concept. These cells migrate in masses as a continuous, coherent sheet, with most cells retaining their positions relative to each other, much like the movement of a herd of cattle.
Rearrangement of intracellular actin filaments plays a role in movement. Cell migration can be inhibited by blocking polymerization of actin, indicating that actin filaments actively participate in the mechanism of cell motion. Some authors believe that conjunctival and limbal epithelial cells may contribute to the regeneration of corneal epithelium. Marked proliferative responses in the conjunctiva after a central corneal epithelium abrasion have been described.
Why the conjunctival epithelium should proliferate in response to a central corneal wound is unknown. One possibility is that the proliferation replenishes the number of goblet cells, which decreases by up to 50% after corneal wounding. However, proliferation occurs at high levels in the bulbar conjunctiva, which contains few if any goblet cells. The apparent decrease in cell number more likely is the result of mucin secretion rather than the actual loss of goblet cells.
Alternatively, conjunctival cells may migrate into the limbus or cornea to help replenish the wound area. No firm data suggest that conjunctival epithelium migrates onto the corneal surface in the presence of intact limbal epithelium. Lastly, healing of the corneal epithelial wound is not complete until the newly regenerated epithelium has firmly anchored itself to the underlying Bowman membrane.
Permanent anchoring units are not formed until the wound defect is covered completely. Epithelial cells migrate rapidly and develop strong, permanent adhesions within 1 week when the basement membrane is regularly formed and released during the cell migration process.
Although transient attachments are regularly formed and released during the cell migration process, formation of normal adhesions takes 6 weeks, according to Dua et al. [4] Tiny buds of corneal epithelium are present along the contact line between the normal corneal epithelium and the migrating conjunctival epithelium. These buds arise from the corneal epithelium, and normal corneal epithelium appears to replace the conjunctival epithelium by gradually pushing it toward the limbus.
The magnitude and extent of both the conjunctival and corneal regenerative responses to a corneal abrasion correlate with the size of the wound. Large epithelial defects were reported to induce a pronounced response in the rate of epithelial cell migration and mitosis at the limbus.
Insults caused by chemical injuries, Stevens-Johnson syndrome, and contact lens–induced keratopathy may result in limbal damage. These insults cause delayed healing of the cornea, recurrent epithelial erosions, corneal vascularization, and conjunctival epithelial ingrowth.
Role of the epithelial defect
A long-standing clinical observation is that bacterial corneal infections do not occur in patients with an intact, healthy epithelium. Bacterial keratitis can develop in 1 of the following 3 types of patients:
-
Those with trauma to the cornea
-
Those with epithelial defects due to intrinsic disease (eg, dry eye, exposure keratitis, neurotrophic keratitis, postinfectious persistent epithelial defects)
-
Those who wear contact lenses, especially extended-wear hydrophilic lenses
The common feature among the 3 groups is a defect in the corneal epithelium to which the bacteria must adhere to start the infection. Mechanisms underlying the development of epithelial defects in the first 2 groups are self-evident. In the third group, contact lenses may lead to epithelial injury in any of the following ways:
-
Injury by insertion or removal of the lens
-
Trauma from defects in or deposits on the lens
-
Lens-induced hypoxia
-
Chemical toxicity from contact-lens disinfectants
Defects in the epithelium need not be full thickness. Overnight wearing of soft lenses, which do not provide sufficient oxygen transmissibility to prevent hypoxia, causes superficial desquamation of epithelium and increases the propensity for abrasions and infections.
Corneal swelling induced by overnight wearing of contact lenses is the most important factor. The cornea normally swells 2-4% during sleep owing to hypotonicity of the nocturnal tear film. With a contact lens in place, overnight swelling increases to an average of 15%, and gross stromal edema can be present on awakening. In some patients, induced corneal swelling can be sufficient to cause corneal bullae, which may rupture, leading to epithelial defects.
Etiology
Potential causes of corneal abrasion include the following [1] :
-
Blowing dust, sand, or debris
-
Extended contact lens wear
-
Ocular foreign bodies embedded under an eyelid
-
Iatrogenic - Unconscious patients, accidental injury by healthcare workers, improper eyelid patching in patients with Bell palsy, and other neuropathies in which the eyelid cannot be closed voluntarily
-
Corneal foreign bodies - Objects difficult to see (eg, small glass fragments)
-
Thermal burns, such as cigarette and match burns
-
UV keratitis - History of exposure to electric arc welding or tanning beds without proper eye protection, history of prolonged exposure to bright sunlight without sunglasses (eg, snow blindness)
-
Eyelid margin injuries, avulsions, and malpositions
-
Punctal and canalicular lacerations
In persons with trachoma, the constant corneal trauma by aberrant lashes and inadequate tears can produce corneal erosions, ulceration, and scarring. These constitute the major pathway to blindness in trachoma.
Contact lens trauma
Contact lens–induced epithelial defects or direct trauma during lens insertion or removal can cause corneal abrasions.
Abrasions occur more frequently with rigid lenses than with other lenses, possibly because of their small diameter and the sharp corneal defects they cause. Rigid contact lenses can lead to relative corneal hypoxia, epithelial edema, and epithelial breakdown. Corneal abrasions due to soft lenses are observed most frequently with tight or extended-wear lenses. In these situations, acute epithelial hypoxia impairs attachment of the epithelium to the Bowman membrane.
The most common trauma is an inferior abrasion of the cornea caused by lens removal. Sometimes, the person's fingernail slices the contact lens and also the cornea. More often, the lens becomes slightly dehydrated at the end of the day because of insufficient blinking. The lens adheres to the cornea, removing the epithelium. This area may not heal well, especially if the epithelial cells are continually torn away. After the contact lens is removed, the patient may feel discomfort; however, no pain occurs when the lens is worn because it acts as a bandage. Patients who incompletely blink and those who work in a dry environment, read most of the day, or look at TV or computer screens should be warned about this complication.
A foreign body may become trapped under a contact lens and produce linear scratch marks on the cornea. The total irregularity of these wavy abrasions is the clue to this cause of injury.
A soft lens offers no protection against blunt trauma to the eye, but it does not pose any additional jeopardy in terms of eye trauma. For example, a soft lens does not adversely affect an eye injured by a fist or a ball. In industrial settings, a soft lens is not a substitute for safety glasses.
Rigid contact lenses may break or chip, causing punctate epithelial keratopathy.
Adverse corneal events, such as corneal abrasions, have been reported with techniques of overnight corneal reshaping with orthokeratology. Lang concluded that corneal compromise and poor compliance can cause adverse events with corneal reshaping. [7] The need for ongoing patient education is important in both children and adults who wear contact lenses.
Sports-related injury
Corneal abrasions can occur in almost all sports. They most frequently occur in young people.
In places where soccer is played frequently, impact with the soccer ball causes approximately one third of all sports-related eye injuries. Contrary to previous ophthalmologic teaching that balls larger than 4 inches in diameter rarely cause eye injury, 8.6-inch soccer balls cause most soccer-related eye injuries, both serious (eg, hyphema, vitreous hemorrhage, retinal tear, chorioretinal rupture, angle recession) and minor (eg, corneal abrasions, contusions). [8]
Approximately 1 in 10 college basketball players has an eye injury each year. Most basketball-related eye injuries are corneal abrasions caused by an opponent's finger or elbow striking the player's eye.
The incidence of severe eye injuries in wrestling is low. In a study at Michigan State University, 18.4% of wrestlers had eye injuries that were relatively mild (eg, lacerated eyebrows, corneal abrasions) and that left no permanent damage. [9] The average college team with 25 players and 2600 athlete exposures should expect 1-2 eye injuries each season, with a significant injury every 9-10 seasons. [10]
Although significant eye injuries are not a major risk in equestrian events other than polo, cross-country riders frequently have corneal abrasions from hitting tree branches overhanging the trail. Wearing spectacles with polycarbonate lenses provides adequate protection against this risk.
Although cross-country skiing causes fewer musculoskeletal injuries than alpine skiing, cross-country skiers are more likely than alpine skiers to have eye injuries, especially corneal abrasions from contact with tree twigs. [11] In addition, both cross-country and downhill skiers can have solar keratopathy (snow blindness) and injuries due to accidents with ski poles.
Eyelid surgery
In patients undergoing eyelid surgery, corneal abrasion can result from sutures inadvertently placed through the tarsus or conjunctival surface. After sutures are placed, the lid should be everted to check that they are not exposed.
The globe and cornea should be protected during lid dissection and suture placement. A contact lens corneal protector or lid plate can be used.
Anesthesia
General anesthesia is more likely to cause adverse systemic effects than local or ocular complications. Ocular problems that do occur are usually not serious and include corneal abrasion, chemical keratitis, hemorrhagic retinopathy, and retinal ischemia (rare).
The incidence of corneal abrasion due to general anesthesia is as high as 44%. Simple precautions, such as instilling a bland ointment or taping both pairs of eyelids closed in the case of nonocular surgery and the lids of the nonoperative eye in the case of ocular surgery, may prevent surface trauma produced by the surgical drape, anesthetic mask, or exposure and drying of the cornea. Decreased tear production under general anesthesia, proptosis, and a poor Bell phenomenon may worsen corneal exposure, requiring eyelid suturing in some susceptible patients.
Argon laser trabeculoplasty
Corneal abrasion is one of the complications of argon laser trabeculoplasty. Others include the following [12] :
-
Discomfort
-
Acutely elevated intraocular pressure (IOP)
-
Progressive visual field loss
-
Peripheral anterior synechiae
-
Iritis
-
Sector palsy of the pupillary sphincter
-
Corneal edema
-
Endothelial damage
-
Vasovagal reaction
Tonometry
The applanation instrument can cause corneal abrasion if the eye or tonometer moves during measurement. In addition, if the disinfectant solution (eg, alcohol) is not removed from the surface of the tonometer, it can cause a circular toxic keratitis where it touches the cornea.
The Schiøtz tonometer must be used in the supine position or in the sitting position with the head back far enough to be horizontal. An initial blink or avoidance reaction may occur as the patient sees the tonometer descending toward the eye. The metal plate of the tonometer or the plunger may abrade the cornea.
Epidemiology
United States statistics
Corneal abrasions are the most common eye injuries and are especially prevalent among people who wear contact lenses. Although corneal abrasions account for about 10% of eye-related emergency visits, the estimated incidence varies by population and depends on how they are defined and the activities involved in the mechanism of injury.
A sampling of diagnoses in the offices of family practice clinicians, internists, and pediatricians in the United States in 1985 found that eye complaints constituted 2% of all patient visits; traumatic conditions and foreign bodies were the reason for 8% of these visits. [13]
Workplace eye injuries cause significant yet avoidable (with protective eyewear) morbidity and lost productivity. In the United States, 65,000 work-related eye injuries and illnesses that cause missed time from work occur each year. [14]
A study of eye injuries in a major US automotive corporation found an annual incidence of 15 eye injuries per 1000 employees. Between July 1989 and June 1992, a total of 1983 work-related eye injuries occurred at 33 plants, with 86.7% of cases being superficial foreign bodies and corneal abrasions. [15] The eye injuries comprised 6% of total injuries. One third of eye injuries resulted in the inability of workers to resume normal duties for at least 1 day.
In another report, most patients with corneal foreign bodies did not take more than 1 day off work, and up to 30% sought treatment outside of working hours to avoid lost time from work.
International statistics
The incidence of nonpenetrating injuries to the eye, which includes corneal abrasions, is 1.57% per year. Corneal abrasions are common, accounting for 12-13% of new cases seen in 2 different eye emergency units in the United Kingdom. [16] They also are frequent presenting problems in general hospital emergency departments.
At a general hospital emergency department in the United Kingdom, 6% of all new cases were eye cases. Trauma accounted for 66% of these cases, or 4% of all cases; corneal abrasions or corneal or conjunctival foreign bodies accounted for 80% of eye trauma cases, or 3% of all cases.
Racial, sexual, and age-related differences in incidence
Rates of corneal abrasion are equal in all races. More males than females are treated for corneal abrasions.
The incidence of corneal abrasion is higher among people of working age. However, people of all ages can have a corneal abrasion. Automotive workers between the ages of 20 and 29 years had the highest incidence of eye injuries. [15]
Prognosis
The prognosis usually is excellent, with full recovery of vision if treatment is prompt; however, untreated corneal abrasions can lead to blinding corneal ulcers.
Some deep abrasions (eg, those involving the corneal stromal layer) in the central visual axis (ie, the main area of the cornea directly over the pupil) heal but leave a scar. In these instances, a permanent loss of visual acuity may result from corneal cloudiness or irregular corneal astigmatism.
Healing of minor abrasions is expected within 24-48 hours. Extensive or deep abrasions may require a week to heal.
Recurrent epithelial erosion sometimes occurs days to weeks after a healing of an abrasion caused by shearing injury (eg, from a fingernail, tree branch, or mascara brush). These erosions may be caused by damage to the basement membrane (to which the newly healed overlying cells do not adhere well) and subsequent slough due to mild hypoxia that occurs during sleep. Patients typically are awakened in the early morning by similar symptoms to those of a corneal abrasion. Ophthalmologic follow-up care and observation are indicated.
Significant morbidity is uncommon and mostly observed with infectious complications or allergies to medications used for treatment. Patients who are poorly nourished or who have compromised corneas are at particular risk. Close follow-up care is necessary, however, because of the ever-present danger of the abrasion progressing to an ulcer. Essentially all corneal ulcers begin with an abrasion.
Corneal abrasions associated with contact lenses can progress to pseudomonal or amebic keratitis and lead to further ocular damage (including perforation or corneal scarring) if not treated promptly. [17] Abrasions involving exposure to vegetable matter are at a high risk of becoming fungal ulcers.
Minor injuries may place substantial economic burdens on otherwise healthy people because of time lost from work or school. Foreign body sensation and pain can result in loss of productivity.
A large study showed that 32% of automobile workers with eye injuries were unable to resume their normal duties for at least 1 day. Unfortunately, only 25% of workers in this study were wearing eye protection at the time of injury. [15] In a retrospective review from Torino, Italy, ocular injuries, including corneal abrasions, were associated with significant morbidity. [18]
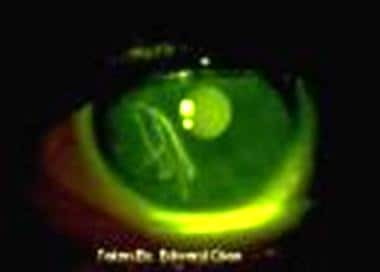
-
This corneal abrasion appears as a yellow-green area when stained with fluorescein and viewed with a blue light.
-
Corneal abrasion.
-
Large corneal abrasion.
-
Corneal keratitis and staining.
-
Corneal foreign body.
-
Corneal foreign body after removal.
-
Corneal foreign body with cobalt blue lighting showing abrasion.

