Background
Intradiskal (intradiscal) electrothermal therapy (IDET), or intradiskal electrothermal anuloplasty (IDEA), is a minimally invasive technique for the treatment of diskogenic low back pain. [1] IDET involves the percutaneous threading of a flexible catheter into the disk under fluoroscopic guidance. The catheter, composed of thermal resistive coil, heats the posterior anulus of the disk, causing contraction of collagen fibers and destruction of afferent nociceptors.
Initial clinical studies suggested that IDET might be effective in approximately 70% of patients with chronic unremitting low back pain. Physical function and quality of life outcomes in highly selected patients have improved. In that IDET is minimally invasive and has a low complication rate, it may offer advantages over surgery. [2, 3, 4] However, there remains a need for studies comparing its outcomes with those of fusion and chronic pain management. The initial reports of IDET require further validation in placebo-controlled randomized trials is needed. [5, 6]
The objectives of this article are to review published reports and present a general overview of IDET. More than 75,000 IDET procedures have been performed in the United States since 1998. The average cost of IDET is seven to eight times less than the average hospital cost of lumbar fusion surgery. [7]
Patient Selection
As with other interventional procedures, proper patient selection increases the chances of a favorable outcome. IDET should be considered in patients who have had diskogenic low back pain for more than 6 months and whose condition has not responded to conservative treatment. [8]
Ideal candidates are patients with a single affected disk as determined by magnetic resonance imaging (MRI) and diskography. Patients with the predominant complaint of axial pain with or without some nonradiating limp pain are suitable candidates. Patients with severe radicular symptoms due to a herniated disk or patients with severe spinal stenosis are not good candidates.
A severely collapsed disk (>50% loss of disk height) might not respond well to IDET, because of technical difficulties in catheter placement and the procedure's questionable effect on high-grade disk injury. Similarly, severely disrupted disk morphology as revealed by diskography may not respond well.
Patients older than 55 years may have lower success rates because of poorer healing. Cigarette smoking may affect anular collagen tissue and hinder adequate recovery following the procedure.
Ideal candidates for IDET meet the following conditions:
-
Preserved disk height (>50%)
-
Contained disk herniation
-
Axial pain greater than leg pain for 3-6 months
-
Posterior anular deficit
-
Motivated patient with no major psychological issues
-
No facet disease
-
Patient younger than 55 years
-
Failure to improve after at least 6 weeks of conservative treatment
-
Diskogenic pain confirmed by provocation diskography
Mechanism of Action
IDET is thought to decrease diskogenic pain through two different mechanisms, as follows:
-
Thermal modification of collagen fibers
-
Destruction of disk nociceptors
Breakage of heat-sensitive hydrogen bonds of the collagen fibers causes collagen contraction. With disk temperatures reaching 650°C, collagen may contract as much as 35% from its original size. The tightening of anular tissue may enhance the structural integrity of degenerated disk and repair the anular fissures. The process of disk restructuring (as shown by time courses of patients' pain relief) may take several months to reach its full extent.
IDET might also cause destruction of sensitized nociceptors in the anular wall. Denervation by thermal energy is used widely for peripheral and central nervous system (CNS) lesions and might contribute to partial initial pain relief following the IDET procedure.
Technical Aspects
The technique for approaching the disk in IDET is similar to the technique used for diskography.
After the skin is infiltrated with local anesthetic, a 17-gauge introducer needle is inserted into the disk under the guidance of oblique fluoroscopy.
Once the position of the needle in the nuclear cavity is established by anteroposterior and lateral fluoroscopic views, the thermal catheter is inserted through the needle. (See the images below.)
 Anteroposterior fluoroscopy view shows introducer needle in disk. Transpedicular approach was used to access disk.
Anteroposterior fluoroscopy view shows introducer needle in disk. Transpedicular approach was used to access disk.

A SpineCATH System thermal catheter may be used (Oratec Interventions, Menlo Park, CA). The catheter should be placed circumferentially around the inner surface of the posterior anulus. (See the images below.)
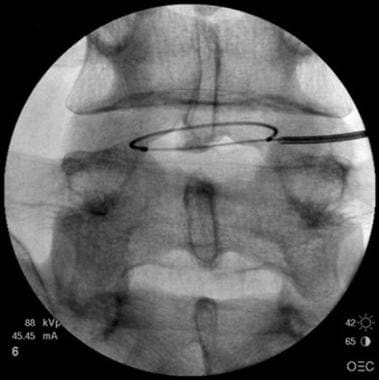 Anteroposterior fluoroscopy view shows catheter around inner surface of posterior anulus.
Anteroposterior fluoroscopy view shows catheter around inner surface of posterior anulus.
 Lateral fluoroscopy view shows catheter around inner surface of posterior anulus.
Lateral fluoroscopy view shows catheter around inner surface of posterior anulus.

Once the catheter is in satisfactory position, it is heated from 37°C to 65 °C. After the temperature has remained at 65° for 1 minute and the patient has not complained of excessive pain, the temperature is increased by 1°C every 30 seconds until it is between 80° and 90°C. The actual temperature of the anular tissue is as much as 15°C lower than the temperature of the catheter tip.
Comprehensive patient and cadaver temperature mapping studies have shown the safety of placing heating catheters within the disk tissue. In these studies, the temperature of the epidural space reached a maximum of 39.30°C when the catheter tip was heated to 90°C. In the same studies, the disk tissue reached a maximum temperature of 72°C and the outer anulus 46°C with catheter tip temperatures of 90°C.
Postprocedural Care
The practitioner must realize, and must point out to the patient, that recovery is gradual. During the first 7 days after the procedure, patients might experience a significant increase in pain. Significant pain relief may take 8-12 weeks. The healing process reaches its peak 4 months after the procedure. During that period, the patient must limit physical activity and follow a carefully structured rehabilitation program.
In general, patients should not return to any kind of heavy physical work during the first 4 months following the procedure. A gradual increase in daily activities is recommended. The patient should do only minimal sitting or standing during the first few days after treatment, and a corset should be worn during the first 6 weeks. Athletic activities can be resumed gradually starting 6 months after the IDET procedure.
The progression of activities after IDET is illustrated in the following sample rehabilitation program.
Activities in week 1 are as follows:
-
Walking allowed
-
Wear lumbosacral corset during all activities
-
Sit for only 35-45 minutes at a time
-
No lifting, twisting, bending, or driving
-
No work
-
No physical therapy
Activities in weeks 2-6 are as follows:
-
Wear lumbosacral corset during all activities
-
Increase sitting time as tolerated
-
Lift no more than 10 lb (~4.5 kg)
-
Driving allowed
-
No twisting or bending
-
Might return to light or sedentary work
-
No physical therapy
Activities in weeks 6-12 are as follows:
-
Lift no more than 25 lb (~11.4 kg)
-
No twisting or bending
-
Might start physical therapy, emphasizing lumbar stabilization program and biomechanics
Activities beyond week 12 are as follows:
-
Lift 25-50 lb (~11.4-22.7 kg)
-
Might return to full work
-
Continue physical therapy, emphasizing home exercise program
Review of Published Studies
The first published report of IDET was by Saal and Saal. In that study, a cohort of 25 patients was shown to have improved clinical outcomes 6 months after they underwent IDET. [9]
Karasek and Bogduk, in a case-controlled study, compared the outcomes of 35 patients treated with IDET with those of 17 patients who were unable to undergo IDET because of lack of insurance coverage. [10] The control group underwent a comprehensive, conservative regimen, which included physical therapy, strengthening, conditioning exercises, and education. This group was monitored for 3 months. The patients in the treatment group underwent IDET and were monitored for 1 year.
In the control group, only one patient had significant improvement 3 months after treatment, three had modest improvement, four had no improvement, and nine had worsening of their condition. [10] Visual Analog Scale (VAS) pain scores were not improved. Only one of the five patients who were working prior to starting the study returned to work. Analgesic use was not affected significantly.
In the IDET group, 32 of 36 patients had statistically significant decreases in VAS scores 12 months after treatment. [10] In the treatment group, 60% had at least a 50% reduction in pain; 23% experienced complete pain relief; and all patients returned to work or continued to work. Of the 19 patients who had at least 50% pain relief, 11 discontinued opioid medication and five continued opioids at lower doses.
Saal and Saal completed a prospective case series of patients with 1 year of follow-up. [11] Sixty-two patients were selected for IDET from a pool of 1116 patients with low back pain who did not respond to at least 6 months of aggressive conservative care. Outcomes were analyzed by using preprocedural and postprocedural VAS, Short Form (SF)-36, and return-to-work status. Of the 62 patients treated, 44 improved their VAS by a mean of 3 points. Physical function scores improved in 71% of the patients (mean change, 20). Bodily pain scores improved in 74% of the patients (mean change, 17.4), and 92% of the patients returned to work.
Shadid et al studied 145 consecutive patients referred for IDET after having positive diskography findings for diskogenic back pain. [12] Of these, 120 were available for follow-up (mean, 18 mo). The average duration of preprocedural symptoms was 39.8 months. Scores on a numerical rating scale and activity levels were monitored. Overall, approximately one third of patients improved, one third remained unchanged, and one third became worse. Fifty-five percent of the patients stated that they would not repeat the procedure.
Pauza et al performed a randomized, placebo-controlled trial of IDET in which patients in the IDET group displayed greater mean improvements in pain, disability, and depression. [13]
Animal studies have been reported. In one such study, posterolateral anular lesions were experimentally induced and allowed to mature for 12 weeks in the intervertebral disks of sheep. [14] IDET was performed in an attempt to denervate and repair the anular lesion. The histologic and immunohistochemical effects of IDET were studied. Vascular granulation tissue and posterior anular neoinnervation were observed in the experimentally induced posterolateral anular lesions.
IDET delivered at 90°C in the sheep consistently heated the posterior anulus and the nucleus to a temperature normally associated with coagulation of nociceptors and collagen contraction. [14] IDET did not denervate the posterior anular lesion. Thermal necrosis was observed within the inner anulus and adjacent nucleus from 6 weeks after IDET. The reported benefits from IDET appear to be related to factors other than denervation and repair.
IDET-induced stress concentrations in disks obtained from cadavers have been analyzed. [15] These studies revealed that IDET has a significant but inconsistent effect on compressive stresses within intervertebral disks. This may provide a partial explanation for the variable success of IDET.
A prospective study was conducted to evaluate improvements in pain and disability in worker's compensation patients with diskogenic low back pain who underwent treatment with the IDET procedure. [16] The study of 53 patients revealed that IDET can be a useful, safe, and cost-effective option in the management of carefully selected workers' compensation claimants who have diskogenic chronic low back pain.
A single-arm prospective clinical trial evaluated back pain severity, physical function, and quality-of-life (QoL) outcomes in 56 highly selected patients with lumbar diskogenic pain. [17] The patients were treated with IDET and monitored for an average of 20.5 ± 4.4 months. Various outcomes were assessed, including back pain severity by VAS; sitting, standing, and walking tolerances; and health-related QoL (measured with SF-36). Pain scores and functional tolerance improved, and seven of eight QoL domains improved significantly over baseline evaluations.
These results suggest that durable clinical improvements can be realized after IDET in highly selected patients who have mild disk degeneration, confirmatory imaging evidence of anular disruption, and concordant pain provocation by low-pressure diskography. [18]
Review of past literature indicates that most patients have reported improvement in symptoms following both spinal fusion and the IDET procedure. In early studies, the IDET procedure appeared to offer symptom amelioration sufficiently similar to that afforded by spinal fusion without the attendant complications. [19] However, some authors, on the basis of final outcome studies, consider IDET an antecedent rather than an alternative to spinal fusion. [20]
A systematic review by Helm et al found l level III (moderate) evidence that IDET is efficacious in the treatment of chronic refractory diskogenic pain. [21]
In a systematic review of intradiskal percutaneous minimally invasive procedures for chronic low back pain, Gelalis et al concluded that IDET, when performed in properly selected patients, may eliminate or delay the need for surgical intervention for an extended period, with few reported adverse effects. [22]
Complications
Complications due to IDET are infrequent. In a retrospective study, the complications of 1675 IDETs performed at five different spine centers were reviewed. [23] In the same study, data related to 35,000 SpineCATH intradiskal catheters from the medical device reports (MDRs) of the United States Food and Drug Administration (FDA) were analyzed. A total of six nerve root injuries were reported, all but one of them occurring at the time of disk puncture. Five of the six resolved completely, and one case was resolving. No cases of diskitis were reported.
Six cases of post-IDET disk herniation were reported at the treated level 2-12 months after treatment. Four resolved with nonoperative care, and two required disk excision. Nineteen cases of catheter breakage were reported. All were associated with repeated catheter manipulation that resulted in kinking. In 16 of these, the catheters were left in the disks; none of these cases was associated with patient morbidity. Eight cases of superficial skin burn at the needle puncture site were reported. A case of post-IDET bladder dysfunction was reported.
A fatal case of an unintentional dose of intrathecal cefazolin, which had been diluted in the nonionic contrast agent that was used to confirm needle placement, was reported. [24] Cefazolin should not be mixed with the contrast agent used to document initial needle placement during diskography.
-
Anteroposterior fluoroscopy view shows introducer needle in disk. Transpedicular approach was used to access disk.
-
Lateral fluoroscopy view shows introducer needle in disk.
-
Anteroposterior fluoroscopy view shows catheter around inner surface of posterior anulus.
-
Lateral fluoroscopy view shows catheter around inner surface of posterior anulus.
-
Axial fluoroscopy view shows catheter around inner surface of posterior anulus.







