Background
Laser diskectomy (discectomy) is an outpatient procedure with one-step insertion of a needle into the disk space. Disk material is not removed; instead, nucleus pulposus is burned by the laser. Laser diskectomy is minimally invasive, cost-effective, [1] and free of postoperative pain syndromes, and it has come to be more widely used at various centers.
Chronic low back pain is one of the major chronic debilitating conditions involving tremendous loss of money, work, and quality time. Lasers are used in different fields of medicine and confer unique advantages. In the treatment of lumbar disk disease, they are useful and advantageous.
The rapid acceptance of minimally invasive surgery in the United States has occurred in many cases without statistical proof of its superiority over traditional methods. All members of the healthcare field see the need for valid outcome studies supporting the efficacy of new treatment techniques. Whether the benefits of laser spine surgery necessarily outweigh the risks remains controversial. [2] To gain wide acceptance, percutaneous laser disk decompression (PLDD) must be demonstrated statistically to be a safe and effective alternative treatment for lumbar disk herniation.
Epiduroscopic laser neural decompression is considered an effective treatment alternative for chronic refractory low-back or lower-extremity pain, including lumbar disk herniation, lumbar spinal stenosis, and failed back surgery syndrome that cannot be alleviated with existing noninvasive conservative treatment. [3, 4, 5]
PLDD performed with computed tomographic (CT) and fluoroscopic guidance appears to be a safe and cost-effective treatment for herniated intervertebral disks and is being used with increasing frequency. [6, 7] It is minimally invasive, can be performed in an outpatient setting, requires no general anesthesia, results in no scarring or spinal instability, shortens the rehabilitation time, is repeatable, and does not preclude open surgery should that become necessary. PLDD has also been performed with ultrasonographic (US) guidance for cervical disk herniation and pain. [8, 9]
Various laser wavelengths have been used, but there is no consensus as to which is most efficacious. [10] Good candidates for this procedure have a classic clinical syndrome and neuroimaging evidence.
In cases of ruptured posterior longitudinal ligament (ie, epidural leak of contrast medium in diskography), PLDD is not indicated. Indications for the operation first of all depend on the clinical symptoms, but the success of the operation depends on the diskographic findings.
Laser-assisted posterior cervical foraminotomy with diskectomy is an efficacious surgical option for treating lateral cervical disk herniation. The pinpoint accuracy of the laser scalpel facilitates sophisticated decompression within a limited surgical field and may reduce the risk of intraoperative bleeding and neural damage. [11]
Indications
This minimally invasive technique can be performed in patients who need surgical intervention for disk herniation (see the image below) with leg pain from radiculopathy. Patient selection and, especially, disk morphology are the two most important factors determining the choice of the technique.
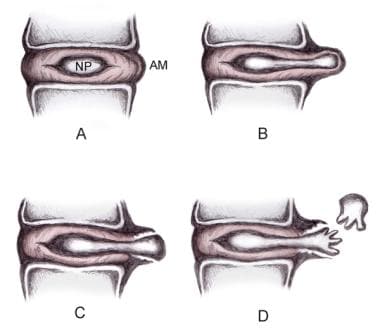 Disk herniation classification. (A) Normal disk anatomy demonstrating nucleus pulposus (NP) and anular margin (AM). (B) Disk protrusion, with NP penetrating asymmetrically through annular fibers but confined within AM. (C) Disk extrusion with NP extending beyond AM. (D) Disk sequestration, with nuclear fragment separated from extruded disk.
Disk herniation classification. (A) Normal disk anatomy demonstrating nucleus pulposus (NP) and anular margin (AM). (B) Disk protrusion, with NP penetrating asymmetrically through annular fibers but confined within AM. (C) Disk extrusion with NP extending beyond AM. (D) Disk sequestration, with nuclear fragment separated from extruded disk.
Criteria for inclusion are evolving. Although the optimal candidate, as previously described, is one who has an untreated single-level herniation with limited migration or sequestration of free fragments, a study from Ahn et al showed the procedure to be effective for recurrent disk herniations in some selected cases. [12] What has been unacceptable may, with modifications, become acceptable in the future. At this stage in the development of PLDD, it is advisable not to adopt a fixed position.
Contraindications
Exclusion criteria for this procedure include stenosis or facet hypertrophy and disk fragment, though a review from Knight et al described its use in foraminoplasty. [13] Relative contraindications are progressive neurologic deficit, involvement in workers' compensation cases, and previous surgery at the same disk level.
In general, the herniation must have continuity with the parent disk; rupture of the anulus is not a contraindication. All patients must be considered on an individual basis.
Technical Considerations
The aim of PLDD is to vaporize a small portion of the nucleus pulposus of an intervertebral disk, thereby reducing the volume of a diseased disk and the pressure within it.
A small amount of tissue is excised from the center or nuclear part of the disk, which is believed to exert an effect on a noncontiguous portion of nucleus that is protruding through the anulus fibrosus and abutting an exiting nerve root. First described by Hijikata in relation to the percutaneous diskectomy method, the central cavity created by the laser is believed to allow the nuclear protrusion to move back within the disk. [14] A small change in disk nucleus volume can exert disproportionately large changes on the disk.
Yonezawa et al first demonstrated significant alterations in intradiskal pressure in response to vertical load after neodymium (Nd):yttrium-aluminum-garnet (YAG) laser treatment. [15] Their study also reported the equivalence of laser to aggressive manual curettage. Choy and Altman reported a greater than 50% reduction of intradiskal pressure in response to load following treatment with 1000 J of Nd:YAG laser energy. [16] Prodoehl et al reported similar results using 1200 J from the holmium (Ho):YAG laser.
No specimen is available to weigh after laser diskectomy; therefore, the amount of disk removed can only be approximated. By calculating the geometry of the laser tract, Choy and Altman estimated that 1000 J of Nd:YAG laser energy vaporized 98.52 mg of disk. [16] Lane et al, who compared the effectiveness of 1200 J each of carbon dioxide, argon, and Ho:YAG laser energy, reported that Ho:YAG was superior, ablating 2.4 g of disk tissue.
By comparison, a clinical trial of automated percutaneous diskectomy reported removal of 2-7 g of disk tissue with a suction cutting device. Quigley's group compared an automated device, Nd:YAG laser, and Ho:YAG laser and clearly demonstrated the superiority of the automated device in removing the greatest mass of tissue. [17]
Outcomes
Laser diskectomy has been used for many years; however, there is a paucity of randomized clinical trials. On the basis of US Preventive Services Task Force criteria, the indicated level of evidence for lumbar PLDD has been limited with respect tor short- and long-term relief.
Reviews by Singh et al and Manchikanti et al revealed limited evidence for lumbar PLDD. Automated percutaneous mechanical lumbar diskectomy may provide appropriate relief in properly selected patients with contained lumbar disk herniation. [18, 19]
An extensive experience was published by Choy and Ascher, who used an Nd:YAG laser. [20] They observed 333 patients for a mean duration of 26 months. The success rate was 78.4% (as measured by a good or fair response) according to MacNab.
Siebert reported on his first 100 patients treated with Nd:YAG. [21] The success rate was 78% at a mean follow-up point of 17 months.
Davis reported an 85% success rate with the potassium titanyl phosphate (KTP) laser, with success defined as minimal discomfort and the ability to return to gainful employment (follow-up duration was not specified). [22]
Yeung reported preliminary assessment of more than 1000 patients whose herniated lumbar disks were treated with a KTP laser. The reported success rate (good or excellent results) was 84%. No specifics were supplied. [23]
Sherk et al used a Ho:YAG laser in a comparison of laser diskectomy and conservative treatment. [24, 25] No differences were noted between treatment and control groups. They concluded that laser diskectomy is a safe procedure that appears to be effective in relieving symptoms in some patients. The author uses a Ho:YAG laser, with a success rate of approximately 80% (comparable to those of other investigators).
In another study from India by Agarwal, Ho:LADD (laser-assisted disk decompression) was found to be a very cost-effective and minimally invasive procedure with patient mobilization immediately after the surgery. [26]
According to Kramer, the best clinical results were found in diskographic stages 7 and 8. [27] In cases of epidural leak of contrast medium and in cases of total degeneration, the clinical results were significantly poor (stages 6 and 9).
The literature includes more than 20 well-documented cases of erectile dysfunction caused by spinal cord disk herniation. PLDD is a minimally invasive procedure that that can be used to treat such herniation.
Singh et al reviewed 38 research reports published between 1986 and 2005 for intradiskal disease therapy classification, surgical intervention, and treatment outcomes (neurologic status, pain scores, and ambulation). Their results revealed that the surgical literature on the management of intradiskal disease continues to be limited, and arthrodesis continues to be the primary treatment modality in most patients. [28] Newer treatment options, including laser diskectomy, have shown promising results with regard to symptomatic relief and early return to function.
Provocative diskography is recommended prior to the PLDD. Besides diskectomy, laser has been used by Knight et al for endoscopic foraminoplasty as well. [13]
Ishiwata et al performed a study on magnetic resonance imaging (MRI)-guided PLDD for lumbar disk herniation. They suggested that the middle zone in the targeted disk space seems to be a favorable target to obtain better clinical outcomes. [29]
In a Cochrane database review by Gibson et al, microdiskectomy yielded results broadly comparable to those of open diskectomy. [30] Surgical diskectomy for carefully selected patients with sciatica due to lumbar disk prolapse provides faster relief from the acute attack than conservative management. The evidence on other minimally invasive techniques is less clear (with the exception of chemonucleolysis using chymopapain, which is no longer widely available).
In a study done in the Netherlands by Schenk et al on routine management of lumbar disk herniation, minimally invasive techniques were expected to be less effective, with higher recurrence rates but less postoperative low back pain. [31] Most surgeons allowed early mobilization but appeared to give conservative advice in resumption of work.
Brouwer et al performed a randomized, controlled trial comparing PLDD with conventional treatment for lumbar disk herniation. [32] In terms of the primary outcome (Roland-Morris Disability Questionnaire), they found a strategy of PLDD, followed by surgery if needed, to be noninferior to surgery at 1 year.
In a retrospective review examining results in 65 patients who underwent percutaneous lumbar laser diskectomy, Patel et al documented a reduction in the average visual analogue scale (VAS) pain score at 2 weeks after the procedure (from 7.6 to 3.7); the VAS score remained below the preprocedural level at 6 weeks (4.3), 3-6 months (4.1), and 12 months (4.2). [33] Neuritis occurred in four cases (two of which were treated pharmacologically) and resolved in all four.
-
Disk herniation classification. (A) Normal disk anatomy demonstrating nucleus pulposus (NP) and anular margin (AM). (B) Disk protrusion, with NP penetrating asymmetrically through annular fibers but confined within AM. (C) Disk extrusion with NP extending beyond AM. (D) Disk sequestration, with nuclear fragment separated from extruded disk.





