Structure of the Extraocular Muscles
Extraocular muscles differ histologically from most other skeletal muscles in that they are made up of 2 different types of muscle cells. Each muscle cell is composed of groups of myofibrils called sarcomeres. Fibrillenstruktur (or fast-twitch) muscle fibrils generate fast eye movements and are composed of well-defined myofibrils with well-developed sarcomeres. Felderstruktur muscle fibrils generate slow or tonic eye movements and are composed of poorly defined myofibrils with poorly developed sarcomeres. [1, 2, 3]
Cholinergic motor neurons supply both types of muscle fibers. The innervation to fibrillenstruktur fibrils is thick and heavily myelinated, with a single (en plaque) neuromuscular junction, whereas the innervation to felderstruktur fibrils is thin, with multiple grapelike clusters of neuromuscular junctions.
Rectus Muscles
Horizontal rectus muscles
Medial and lateral rectus muscles originate from the annulus of Zinn. They travel anteriorly along the orbital walls, inserting 5.5 mm and 6.9 mm from the limbus, respectively. (See the image below.)
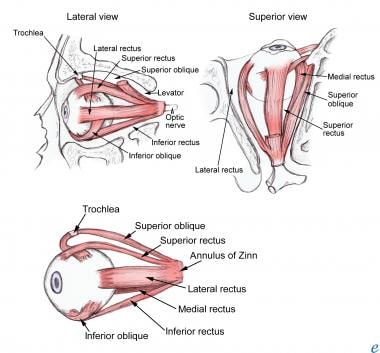 Extraocular muscle anatomy.
Extraocular muscle anatomy.
Vertical rectus muscles
Superior and inferior rectus muscles also originate from the annulus of Zinn. They travel anteriorly and laterally at an angle of 23º with the visual axis of the eye in primary position. They insert 7.7 mm and 6.5 mm from the limbus, respectively.
Insertion relationships
A working knowledge of the relationships between the insertions of the rectus muscles is essential to performing effective strabismus surgery. [4, 5, 6]
The tendon of the medial rectus muscle inserts 5.5 mm posterior to the limbus along the medial aspect of the globe. Next most posterior in its insertion is the inferior rectus, which inserts 6.5 mm posterior to the inferior limbus. Continuing counterclockwise around the globe, the lateral rectus inserts 6.9 mm posterior to the lateral limbus, and the superior rectus inserts 7.7 mm posterior from the superior limbus. An imaginary line connecting these insertion points creates a configuration known as the spiral of Tillaux.
Oblique Muscles
The superior oblique muscle originates from the orbital apex above the annulus of Zinn and passes anteriorly along the superomedial orbital wall. The tendon of the superior oblique muscle passes through the trochlea (which is located nasally at the superior orbital rim) and is reflected inferiorly, posteriorly, and laterally at an angle of 51º to the visual axis with the eye in primary position. The tendon passes beneath the superior rectus muscle before inserting posterior to the equator on the superior and lateral aspect of the globe.
The inferior oblique muscle originates from the maxillary bone behind the lacrimal fossa, slightly posterior to the orbital rim. It passes posteriorly and laterally in the orbit, forming an angle of 51º with the visual axis of the eye in primary position, before passing beneath the inferior rectus muscle and inserting posterior to the equator on the inferior and lateral aspect of the globe.
Nerves of the Extraocular Muscles
The upper division of the oculomotor nerve (cranial nerve [CN] III) innervates the superior rectus and the levator palpebrae superioris muscles. The lower division of CN III innervates the inferior rectus, medial rectus, and inferior oblique muscles. The nerve to the inferior oblique muscle enters the muscle laterally at the junction of the inferior oblique and inferior rectus muscles.
The trochlear nerve (CN IV) innervates the superior oblique muscle, entering it approximately one third of the distance from the origin to the trochlea. The abducens nerve (CN VI) innervates the lateral rectus muscle.
The parasympathetic innervation to the pupillary sphincter and ciliary muscle travels with the nerve to the inferior oblique muscle. The parasympathetics may be injured during inferior oblique surgery or orbital floor surgery. [1] All other nerves enter their respective muscle at the junction of the posterior one third and anterior two thirds of the muscle. (See also Extraocular Muscle Actions.)
Blood Supply of the Extraocular Muscles
The eye's major blood supply comes from the ophthalmic artery. The lateral muscular branch of the ophthalmic artery supplies the lateral rectus, superior rectus, and superior oblique muscles. The medial muscular branch supplies the inferior rectus, medial rectus, and inferior oblique muscles.
Medial and lateral muscular branches of the artery give rise to 7 anterior ciliary vessels, which travel with the 4 rectus muscles to provide circulation for the anterior segment of the eye. Each rectus muscle has 2 anterior ciliary vessels, except for the lateral rectus muscle, which has 1 vessel. These vessels pass anteriorly to the episclera and supply the anterior segment of the eye, including the sclera, limbus, and conjunctiva.
Orbital Connections of the Extraocular Muscles
A complex system of connective tissue links the extraocular muscles and contributes to ocular stability and alignment. The Tenon capsule is an envelope of connective tissue that covers the globe from the optic nerve to its fusion with the conjunctiva, approximately 3 mm posterior to the limbus. It prevents contact between intraconal orbital fat and the sclera. All 6 extraocular muscles penetrate anteriorly through sleeves or slits in the Tenon capsule en route to their insertion onto the globe.
Each rectus muscle also has a surrounding fascial sheath that covers the muscle from its origin to its insertion. Each muscle sheath is connected by a fibrous extension to the adjacent muscle sheaths, thereby forming the intermuscular septum. The intermuscular septum, which begins at the orbital apex, passes anteriorly to its fusion with the Tenon capsule, approximately 3 mm posterior to the limbus.
-
Extraocular muscle anatomy.