Parke WW. Correlative anatomy of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988 Jul. 13(7):831-7. [QxMD MEDLINE Link].
McCormack BM, Weinstein PR. Cervical spondylosis. An update. West J Med. 1996 Jul-Aug. 165(1-2):43-51. [QxMD MEDLINE Link].
Wilkinson M. The morbid anatomy of cervical spondylosis and myelopathy. Brain. 1960 Dec. 83:589-617. [QxMD MEDLINE Link].
Hoff JT, Wilson CB. The pathophysiology of cervical spondylotic radiculopathy and myelopathy. Clin Neurosurg. 1977. 24:474-87. [QxMD MEDLINE Link].
Rosomoff HL, Fishbain D, Rosomoff RS. Chronic cervical pain: radiculopathy or brachialgia. Noninterventional treatment. Spine (Phila Pa 1976). 1992 Oct. 17(10 Suppl):S362-6. [QxMD MEDLINE Link].
Emery SE. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg. 2001 Nov-Dec. 9(6):376-88. [QxMD MEDLINE Link].
Fehlings MG, Skaf G. A review of the pathophysiology of cervical spondylotic myelopathy with insights for potential novel mechanisms drawn from traumatic spinal cord injury. Spine (Phila Pa 1976). 1998 Dec 15. 23(24):2730-7. [QxMD MEDLINE Link].
Young WF. Cervical spondylotic myelopathy: a common cause of spinal cord dysfunction in older persons. Am Fam Physician. 2000 Sep 1. 62(5):1064-70, 1073. [QxMD MEDLINE Link].
McCormick WE, Steinmetz MP, Benzel EC. Cervical spondylotic myelopathy: make the difficult diagnosis, then refer for surgery. Cleve Clin J Med. 2003 Oct. 70(10):899-904. [QxMD MEDLINE Link].
Young WF, Weaver M, Mishra B. Surgical outcome in patients with coexisting multiple sclerosis and spondylosis. Acta Neurol Scand. 1999 Aug. 100(2):84-7. [QxMD MEDLINE Link].
al-Mefty O, Harkey HL, Marawi I, et al. Experimental chronic compressive cervical myelopathy. J Neurosurg. 1993 Oct. 79(4):550-61. [QxMD MEDLINE Link].
Henderson FC, Geddes JF, Vaccaro AR, Woodard E, Berry KJ, Benzel EC. Stretch-associated injury in cervical spondylotic myelopathy: new concept and review. Neurosurgery. 2005 May. 56(5):1101-13; discussion 1101-13. [QxMD MEDLINE Link].
Moore AP, Blumhardt LD. A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Spinal Cord. 1997 Jun. 35(6):361-7. [QxMD MEDLINE Link].
Holt S, Yates PO. Cervical spondylosis and nerve root lesions. Incidence at routine necropsy. J Bone Joint Surg Br. 1966 Aug. 48(3):407-23. [QxMD MEDLINE Link].
Rahim KA, Stambough JL. Radiographic evaluation of the degenerative cervical spine. Orthop Clin North Am. 1992 Jul. 23(3):395-403. [QxMD MEDLINE Link].
Heller JG. The syndromes of degenerative cervical disease. Orthop Clin North Am. 1992 Jul. 23(3):381-94. [QxMD MEDLINE Link].
Ellenberg MR, Honet JC, Treanor WJ. Cervical radiculopathy. Arch Phys Med Rehabil. 1994 Mar. 75(3):342-52. [QxMD MEDLINE Link].
Stoffman MR, Roberts MS, King JT Jr. Cervical spondylotic myelopathy, depression, and anxiety: a cohort analysis of 89 patients. Neurosurgery. 2005 Aug. 57(2):307-13; discussion 307-13. [QxMD MEDLINE Link].
Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg. 1954 Nov. 11(6):546-77. [QxMD MEDLINE Link].
Kaye JJ, Dunn AW. Cervical spondylotic dysphagia. South Med J. 1977 May. 70(5):613-4. [QxMD MEDLINE Link].
Umerah BC, Mukherjee BK, Ibekwe O. Cervical spondylosis and dysphagia. J Laryngol Otol. 1981 Nov. 95(11):1179-83. [QxMD MEDLINE Link].
Sobol SM, Rigual NR. Anterolateral extrapharyngeal approach for cervical osteophyte-induced dysphagia. Literature review. Ann Otol Rhinol Laryngol. 1984 Sep-Oct. 93(5 Pt 1):498-504. [QxMD MEDLINE Link].
Farooqi NA, Doran M, Buxton N. Cervical osteophytes: a cause of potentially life-threatening laryngeal spasms. Case report. J Neurosurg Spine. 2006 May. 4(5):419-20. [QxMD MEDLINE Link].
Kanbay M, Selcuk H, Yilmaz U. Dysphagia caused by cervical osteophytes: a rare case. J Am Geriatr Soc. 2006 Jul. 54(7):1147-8. [QxMD MEDLINE Link].
Teresi LM, Lufkin RB, Reicher MA, et al. Asymptomatic degenerative disk disease and spondylosis of the cervical spine: MR imaging. Radiology. 1987 Jul. 164(1):83-8. [QxMD MEDLINE Link].
Brown BM, Schwartz RH, Frank E, Blank NK. Preoperative evaluation of cervical radiculopathy and myelopathy by surface-coil MR imaging. AJR Am J Roentgenol. 1988 Dec. 151(6):1205-12. [QxMD MEDLINE Link].
Alexander JT. Natural history and nonoperative management of cervical spondylosis. In: Menezes AH, Sonntag VKH, et al. Principles of Spinal Surgery. Vol 1. 1996:547-557.
Penning L, Wilmink JT, van Woerden HH, Knol E. CT myelographic findings in degenerative disorders of the cervical spine: clinical significance. AJR Am J Roentgenol. 1986 Apr. 146(4):793-801. [QxMD MEDLINE Link].
Yamazaki T, Suzuki K, Yanaka K, Matsumura A. Dynamic computed tomography myelography for the investigation of cervical degenerative disease. Neurol Med Chir (Tokyo). 2006 Apr. 46(4):210-5; discussion 215-6. [QxMD MEDLINE Link].
Song T, Chen WJ, Yang B, et al. Diffusion tensor imaging in the cervical spinal cord. Eur Spine J. 2011 Mar. 20(3):422-8. [QxMD MEDLINE Link].
Iwabuchi M, Kikuchi S, Sato K. Pathoanatomic investigation of cervical spondylotic myelopathy. Fukushima J Med Sci. 2004 Dec. 50(2):47-54. [QxMD MEDLINE Link].
Gore DR, Sepic SB, Gardner GM, Murray MP. Neck pain: a long-term follow-up of 205 patients. Spine (Phila Pa 1976). 1987 Jan-Feb. 12(1):1-5. [QxMD MEDLINE Link].
AGS Panel on Persistent Pain in Older Persons. The management of of persistent pain in older persons. J Am Geriatr Soc. 2002. 50(Suppl 6):S205-S224.
Swezey RL, Swezey AM, Warner K. Efficacy of home cervical traction therapy. Am J Phys Med Rehabil. 1999 Jan-Feb. 78(1):30-2. [QxMD MEDLINE Link].
Kaiser MG, Haid RW, Subach BR, Barnes B, Rodts GE Jr. Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft. Neurosurgery. Feb-2002. 50:229-236.
Baskin DS, Ryan P, Sonnta V, Westmark R, Wedmayer MA. A prospective, randomized, controlled cervical fusion study using recombinant human bone morphogentic protein-2 with the CORNERSTONE-SR allograft ring and the ATLANTIS anterior cervical plate. Spine. 2003. 28:1219-1225.
Rowland LP. Surgical treatment of cervical spondylotic myelopathy: time for a controlled trial. Neurology. 1992 Jan. 42(1):5-13. [QxMD MEDLINE Link].
Nurick S. The natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain. 1972. 95(1):101-8. [QxMD MEDLINE Link].
Fouyas IP, Statham PF, Sandercock PA. Cochrane review on the role of surgery in cervical spondylotic radiculomyelopathy. Spine (Phila Pa 1976). 2002 Apr 1. 27(7):736-47. [QxMD MEDLINE Link].
Kadanka Z, Mares M, Bednaník J, et al. Approaches to spondylotic cervical myelopathy: conservative versus surgical results in a 3-year follow-up study. Spine (Phila Pa 1976). 2002 Oct 15. 27(20):2205-10; discussion 2210-1. [QxMD MEDLINE Link].
Sampath P, Bendebba M, Davis JD, Ducker TB. Outcome of patients treated for cervical myelopathy. A prospective, multicenter study with independent clinical review. Spine (Phila Pa 1976). 2000 Mar 15. 25(6):670-6. [QxMD MEDLINE Link].
Ma X, Zhao XF, Zhao YB. [A clinical study on different decompression methods in cervical spondylosis]. Zhonghua Wai Ke Za Zhi. 2009 Apr 15. 47(8):607-9. [QxMD MEDLINE Link].
Lee JY, Sharan A, Baron EM, et al. Quantitative prediction of spinal cord drift after cervical laminectomy and arthrodesis. Spine (Phila Pa 1976). 2006 Jul 15. 31(16):1795-8. [QxMD MEDLINE Link].
Wang MY, Shah S, Green BA. Clinical outcomes following cervical laminoplasty for 204 patients with cervical spondylotic myelopathy. Surg Neurol. 2004 Dec. 62(6):487-92; discussion 492-3. [QxMD MEDLINE Link].
Kaminsky SB, Clark CR, Traynelis VC. Operative treatment of cervical spondylotic myelopathy and radiculopathy. A comparison of laminectomy and laminoplasty at five year average follow-up. Iowa Orthop J. 2004. 24:95-105. [QxMD MEDLINE Link].
Grob D. Surgery in the degenerative cervical spine. Spine (Phila Pa 1976). 1998 Dec 15. 23(24):2674-83. [QxMD MEDLINE Link].
Kumar VG, Rea GL, Mervis LJ, McGregor JM. Cervical spondylotic myelopathy: functional and radiographic long-term outcome after laminectomy and posterior fusion. Neurosurgery. 1999 Apr. 44(4):771-7; discussion 777-8. [QxMD MEDLINE Link].
Houten JK, Cooper PR. Laminectomy and posterior cervical plating for multilevel cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament: effects on cervical alignment, spinal cord compression, and neurological outcome. Neurosurgery. 2003 May. 52(5):1081-7; discussion 1087-8. [QxMD MEDLINE Link].
Huang RC, Girardi FP, Poynton AR, Cammisa Jr FP. Treatment of multilevel cervical spondylotic myeloradiculopathy with posterior decompression and fusion with lateral mass plate fixation and local bone graft. J Spinal Disord Tech. 2003 Apr. 16(2):123-9. [QxMD MEDLINE Link].
Chagas H, Domingues F, Aversa A, Vidal Fonseca AL, de Souza JM. Cervical spondylotic myelopathy: 10 years of prospective outcome analysis of anterior decompression and fusion. Surg Neurol. 2005. 64 Suppl 1:S1:30-5; discussion S1:35-6. [QxMD MEDLINE Link].
Chibbaro S, Benvenuti L, Carnesecchi S, et al. Anterior cervical corpectomy for cervical spondylotic myelopathy: experience and surgical results in a series of 70 consecutive patients. J Clin Neurosci. 2006 Feb. 13(2):233-8. [QxMD MEDLINE Link].
Macdonald RL, Fehlings MG, Tator CH, et al. Multilevel anterior cervical corpectomy and fibular allograft fusion for cervical myelopathy. J Neurosurg. 1997 Jun. 86(6):990-7. [QxMD MEDLINE Link].
Santiago P, Fessler RG. Minimally Invasive Surgery for the Management of cervical spondylosis. Neurosurgery. Jan-2007. 60:S1-160-165.
Heller JG, Sasso RC, Papadopoulos SM, et al. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976). 2009 Jan 15. 34(2):101-7. [QxMD MEDLINE Link].
Razack N, Greenberg J, Green BA. Surgery for cervical myelopathy in geriatric patients. Spinal Cord. 1998 Sep. 36(9):629-32. [QxMD MEDLINE Link].
Murphey F, Simmons JC, Brunson B. Chapter 2. Ruptured cervical discs, 1939 to 1972. Clin Neurosurg. 1973. 20:9-17. [QxMD MEDLINE Link].
Whitecloud TS 3rd, Seago RA. Cervical discogenic syndrome. Results of operative intervention in patients with positive discography. Spine (Phila Pa 1976). 1987 May. 12(4):313-6. [QxMD MEDLINE Link].
Bracken MB, Shepard MJ, Collins WF Jr, et al. Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study. J Neurosurg. 1992 Jan. 76(1):23-31. [QxMD MEDLINE Link].
Chesnut RM, Abitbol JJ, Garfin SR. Surgical management of cervical radiculopathy. Indication, techniques, and results. Orthop Clin North Am. 1992 Jul. 23(3):461-74. [QxMD MEDLINE Link].
Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999 Apr. 44(4):762-9; discussion 769-70. [QxMD MEDLINE Link].
Clarke E, Robinson PK. Cervical myelopathy: a complication of cervical spondylosis. Brain. 1956 Sep. 79(3):483-510. [QxMD MEDLINE Link].
Clements DH, O'Leary PF. Anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 1990 Oct. 15(10):1023-5. [QxMD MEDLINE Link].
Connor PM, Darden BV 2nd. Cervical discography complications and clinical efficacy. Spine (Phila Pa 1976). 1993 Oct 15. 18(14):2035-8. [QxMD MEDLINE Link].
Cull R, Whittle I. The nervous system. Munro J, Edwards CS. Macleod's Clinical Examination. 1995. 201-256.
Denno JJ, Meadows GR. Early diagnosis of cervical spondylotic myelopathy. A useful clinical sign. Spine (Phila Pa 1976). 1991 Dec. 16(12):1353-5. [QxMD MEDLINE Link].
Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R. Cervical radiculopathy. A review. Spine (Phila Pa 1976). 1986 Dec. 11(10):988-91. [QxMD MEDLINE Link].
Dillin W, Uppal GS. Analysis of medications used in the treatment of cervical disk degeneration. Orthop Clin North Am. 1992 Jul. 23(3):421-33. [QxMD MEDLINE Link].
Durufle A, Petrilli S, Le Guiet JL, et al. Cervical spondylotic myelopathy in athetoid cerebral palsy patients: about five cases. Joint Bone Spine. 2005 May. 72(3):270-4. [QxMD MEDLINE Link].
Ebara S, Yonenobu K, Fujiwara K, Yamashita K, Ono K. Myelopathy hand characterized by muscle wasting. A different type of myelopathy hand in patients with cervical spondylosis. Spine (Phila Pa 1976). 1988 Jul. 13(7):785-91. [QxMD MEDLINE Link].
Firooznia H, Ahn JH, Rafii M, Ragnarsson KT. Sudden quadriplegia after a minor trauma. The role of preexisting spinal stenosis. Surg Neurol. 1985 Feb. 23(2):165-8. [QxMD MEDLINE Link].
Goodridge AE, Feasby TE, Ebers GC, Brown WF, Rice GP. Hand wasting due to mid-cervical spinal cord compression. Can J Neurol Sci. 1987 Aug. 14(3):309-11. [QxMD MEDLINE Link].
Haerer AF. Examination in cases of suspected hysteria and malingering. DeJong's The Neurologic Examination. 5th ed. 1992. 744.
Haldeman S, Kohlbeck FJ, McGregor M. Risk factors and precipitating neck movements causing vertebrobasilar artery dissection after cervical trauma and spinal manipulation. Spine (Phila Pa 1976). 1999 Apr 15. 24(8):785-94. [QxMD MEDLINE Link].
Irvine DH, Foster JB, Newell DJ, Klukvin BN. Prevalence of cervical spondylosis in a general practice. Lancet. 1965 May 22. 14:1089-92. [QxMD MEDLINE Link].
Jumah KB, Nyame PK. Relationship between load carrying on the head and cervical spondylosis in Ghanaians. West Afr J Med. 1994 Jul-Sep. 13(3):181-2. [QxMD MEDLINE Link].
Kaiser JA, Holland BA. Imaging of the cervical spine. Spine (Phila Pa 1976). 1998 Dec 15. 23(24):2701-12. [QxMD MEDLINE Link].
LaBan MM, Taylor RS. Manipulation: an objective analysis of the literature. Orthop Clin North Am. 1992 Jul. 23(3):451-9. [QxMD MEDLINE Link].
Lam M. Headache. Adler SN, et al. A Pocket manual of Differential Diagnosis. 1994. 303-304.
LaRocca H. Cervical spondylotic myelopathy: natural history. Spine (Phila Pa 1976). 1988 Jul. 13(7):854-5. [QxMD MEDLINE Link].
Lees F, Turner J. Natural history and prognosis of cervical spondylosis. BMJ. 1963. 2:1603.
Nakano KK. Neck pain. Kelley WN, Harris ED, Ruddy S, Sledge CB. Textbook of Rheumatology. 1985. 471-490.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K. Myelopathy hand. New clinical signs of cervical cord damage. J Bone Joint Surg Br. 1987 Mar. 69(2):215-9. [QxMD MEDLINE Link].
Papadopoulos SM, Hoff JT. Anatomical treatment of cervical spondylosis. Clin Neurosurg. 1994. 41:270-85. [QxMD MEDLINE Link].
Phillips DG. Surgical treatment of myelopathy with cervical spondylosis. J Neurol Neurosurg Psychiatry. 1973 Oct. 36(5):879-84. [QxMD MEDLINE Link]. [Full Text].
Raynor RB, Pugh J, Shapiro I. Cervical facetectomy and its effect on spine strength. J Neurosurg. 1985 Aug. 63(2):278-82. [QxMD MEDLINE Link].
Robinson R, Smith G. Anterolateral cervical disc removal and interbody fusion for cervical disc syndrome. Bull Johns Hopkins Hosp. 1955. 96:223.
Saunders R. Corpectomy for cervical spondylotic myelopathy. Menezes AH, Sonntag VH, et al. Principles of Spinal Surgery. 1996. Vol. 1: 559-569.
Schellhas KP, Smith MD, Gundry CR, Pollei SR. Cervical discogenic pain. Prospective correlation of magnetic resonance imaging and discography in asymptomatic subjects and pain sufferers. Spine (Phila Pa 1976). 1996 Feb 1. 21(3):300-11; discussion 311-2. [QxMD MEDLINE Link].
Tan JC, Nordin M. Role of physical therapy in the treatment of cervical disk disease. Orthop Clin North Am. 1992 Jul. 23(3):435-49. [QxMD MEDLINE Link].
Verbiest H. Chapter 23. The management of cervical spondylosis. Clin Neurosurg. 1973. 20:262-94. [QxMD MEDLINE Link].
Viikari-Juntura E, Porras M, Laasonen EM. Validity of clinical tests in the diagnosis of root compression in cervical disc disease. Spine (Phila Pa 1976). 1989 Mar. 14(3):253-7. [QxMD MEDLINE Link].
Watson JC, Broaddus WC, Smith MM, Kubal WS. Hyperactive pectoralis reflex as an indicator of upper cervical spinal cord compression. Report of 15 cases. J Neurosurg. 1997 Jan. 86(1):159-61. [QxMD MEDLINE Link].
Yoo K, Origitano TC. Familial cervical spondylosis. Case report. J Neurosurg. 1998 Jul. 89(1):139-41. [QxMD MEDLINE Link].
Yoss RE, Corbin KB, Maccarty CS, Love JG. Significance of symptoms and signs in localization of involved root in cervical disk protrusion. Neurology. 1957 Oct. 7(10):673-83. [QxMD MEDLINE Link].
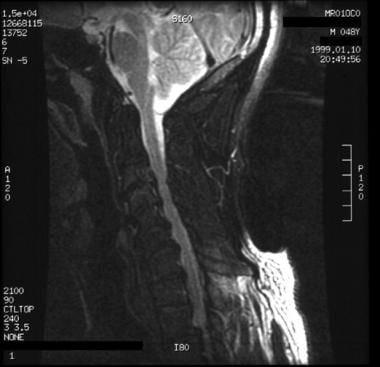 A 48-year-old man presented with neck pain and predominantly left-sided radicular symptoms in the arm. The patient's symptoms resolved with conservative therapy. T2-weighted sagittal MRI shows ventral osteophytosis, most prominent between C4 and C7, with reduction of the ventral cerebrospinal fluid sleeve.
A 48-year-old man presented with neck pain and predominantly left-sided radicular symptoms in the arm. The patient's symptoms resolved with conservative therapy. T2-weighted sagittal MRI shows ventral osteophytosis, most prominent between C4 and C7, with reduction of the ventral cerebrospinal fluid sleeve.
