Overview
Alzheimer disease (AD) is the most common progressive degenerative form of dementia, strongly associated with advancing age. [1, 2] Although AD is strongly associated with advancing age, it should not be considered a normal aging process. Instead, AD is characterized by the continuous progression of the symptoms and associated neuropathological changes. Almost all adultswith Down syndrome (DS) develop neuropathological AD changes by 40 years of age. [3] The leading cause of death in individuals with DS is AD and its complications. [4]
DS was recognized as a unique form of developmental disability in 1866 by Dr. John Landon Down, and early aging was already identified by 1876. [5] In 1948, G.A Jervis reported the dementia course and neuropathological changes in DS were similar to AD in individuals without DS. [3] (Jervis 1948) Further research has confirmed premature aging and clinical deterioration, and the presence of neuropathological changes in AD.
Individuals with DS or trisomy 21 develop a clinical syndrome of dementia with clinical and neuropathologic characteristics almost identical to those of AD as described in individuals without DS. [6]
Accelerated aging in DS is not confined to the central nervous system (CNS) and occurs in various other systems. [7, 8] The recognition that DS is associated with trisomy 21 helped in understanding the genetic basis of this association.
The neuropathology of AD in persons with DS closely resembles that of AD in persons without DS. [9, 10, 11, 12, 13] Autopsy studies in persons with DS showed that almost all had brain lesions meeting the criteria for AD. [14, 15]
However, these changes are superimposed in individuals with reduced brain volume, especially in the hippocampus, and other developmental abnormalities, such as reduced dendritic arborizations, decreased number of spines, spine atrophy, and abnormalities of spine orientation in pyramidal neurons. This form of AD is not an exact biologic model or a replica of the AD seen in individuals without DS. Therefore, although conclusions from research studies may be interchangeable, AD in persons with DS should be considered different from AD without DS.
Clinical differences have been observed, mainly in the early age of onset of AD in individuals with DS. These patients present with clinical symptoms in their late 40s or early 50s. [16, 17, 9, 18, 19]
A longitudinal study [20] that followed babies with DS from age six weeks up to age 45 years found that the mean IQ in verbal and nonverbal tasks changed little between ages 21 and 45 years. However, in this study, tests for dementia given to persons older than 30 years showed some performance decline from 40 to 45 years.
Besides age, other studies have also shown some clinical differences that might be unique to persons with DS.
One study compared the clinical findings in individuals with DS and dementia with those with dementia and intellectual disabilities. The study reported that patients with DS had a higher prevalence of mood changes, overactivity, auditory hallucinations, disturbed sleep, and less aggression due to other etiologies. [21, 22, 23]
Temple and Konstantareas found that persons with DS and AD have less severe psychotic behaviors, fewer hallucinations, and fewer delusions and were more likely to engage in physical movements than those with AD only. In this study, 66% of the persons with AD and without DS were taking rivastigmine or donepezil, and only 26% of persons with AD and DS were on those medications. The differences observed might have been related more to the use of the medications than to the disease itself. [24]
The prognosis is poor as no treatment is available for the primary disease. AD is responsible for the sharp decline in survival in persons with DS older than 45 years. Only about 25% of persons with DS live more than 60 years, and most have AD.
Pathophysiology/Risk Factors
Although Alzheimer disease (AD) is more frequent in individuals with Down syndrome (DS), the main contributing factor is unknown. All recognized mutations for AD are associated with increased deposition of amyloid-beta (Abeta), a peptide fragment comprising 39–43 amino acids that derive from the catabolism of the amyloid precursor protein (APP) molecule. The discovery that the APP gene is on the 21st chromosome [25] led to the hypothesis that the early and universal development of AD pathology is due to a third copy of the APP gene. Nonetheless, many steps in the amyloid cascade hypothesis remain unproven.
The Abeta peptide was reported in the brains of children with DS as young as eight years, and the deposits increase with age. Interestingly, despite the extensive deposits in the brain, there is no linear correlation with AD. There is a gap between abnormal brain pathology and the early signs of AD, suggesting that other factors (genetic or environmental) may play an essential role in AD development.
Chromosomal abnormalities
Approximately 95% of individuals with DS have trisomy 21. In around 4%, there is a translocation of critical regions of chromosome 21, which are attached to chromosomes 14, 21, or 22. In a small percentage of cases (< 1%), DS is the result of a mosaic, with some but not all cells being trisomic. Even though there is a triplication of the whole chromosome, probably only a tiny portion is critical for developing DS neuropathology and clinical features in a complex phenotype-genotype relationship. [26]
The presence of an extra chromosome and the overexpression of the genes located in that chromosome are considered the main reason for developing DS characteristic signs and symptoms and probably plays a vital role in developing AD in individuals with DS. Overexpression of genes with a consequent increase in the activity leads to increased production of end products, which can be toxic for the individual. However, determining which genes are responsible for AD development in DS is not accessible due to the number of genes in chromosome 21 (233 coding genes, 299 long non-coding genes, and 29 microRNA). [27] Besides, clinical expressions of a gene are dependent on several factors, such as the number of copies of the gene, environmental context, and so on. [28] These variations in the expression of the genes' activities in the development of AD in DS may explain the variations in the development of neuropathology and dementia in DS.
Several genes that might play a role in AD development are found on chromosome 21. The APP and cytoplasmic enzyme superoxide dismutase (SOD-1) genes regulate potentially toxic metabolites, the reactive oxygen species (ROSs) resulting from the normal metabolism of oxygen (O2). These ROSs include free radicals (superoxide anions, nitric oxide, hydroxyl radical) and other non-radical metabolites (eg, hydrogen peroxide) whose accumulation may result in cell death. [29, 7]
The excess activity of SOD-1 in various cells is not limited to the brain but is also observed in erythrocytes, B cells, T cells, and fibroblasts. This increased activity accumulates hydrogen peroxide (H2O2), which may reach toxic levels and cause neuronal death observed in DS and carcinogenesis and the impairment of immune functions.
In most instances, trisomy 21, the result of a failure of the pair of chromosomes to separate, is of maternal origin. Interestingly, there is a 4x higher incidence of AD in younger mothers (< 35 years) who give birth to a child with DS compared with mothers > 35 years. This pattern was not reported in the fathers and parents of children with other intellectual disabilities. [30]
Case studies of adults with DS and atypical karyotypes, including translocations, partial trisomies, and varying degrees of mosaicism, showed improved survival and decreased risk of AD when the atypical karyotype is associated with a reduction of the APP gene dose. [31]
Sex differences and estrogen
AD seems to occur more frequently in women than in men. However, this issue is not well studied in persons with DS. Still, some studies suggest that this might also be the case in females with DS, suggesting that reductions in estrogen following menopause can contribute to the cascade of pathological processes leading to AD. [32]
APP overexpression
The overexpression of the APP gene might be related to the overproduction of the significant protein observed in the senile plaque, the Abeta (1-42) peptide, which is considered to be one of the critical factors leading to the development of the pathology of DS with AD. The cleavage of the APP generates Abeta peptide by beta- and gamma-secretase enzymes.
In addition, the supporting role of APP triplication, a regular extra copy of APP in the absence of trisomy 21, is associated with a rare, early form of familial AD (the dup-APP). In this condition, the triplication present varies in size. Still, only one APP triplication is enough for the development of the syndrome, which is very similar in clinical presentation and pathology, barring a few differences, to AD in DS. [33]
According to a large UK series, duplication of APP, but not the prion protein (PRNP) gene, is a significant cause of early-onset dementia. [34]
APP locus duplication causes autosomal dominant early-onset AD with cerebral amyloid angiopathy. [35] APP may be active early in life since there are reports of increased deposits of Abeta 42 amyloid in the brain of fetuses with trisomy 21. [36] Still, the significant accumulation does not occur until the second or third decade, suggesting that maybe there is a more efficient clearance mechanism in early life. Indeed, further studies on the role of APP and other factors that modulate APP expression would enhance our understanding of AD in DS and non-DS populations. [37]
Beta site APP-cleaving enzyme 1 (BACE1), the most important beta-secretase in vivo, is elevated in persons with DS and may play a role in accumulating beta-amyloid. [38]
Another important factor could be the apolipoprotein E (APOE) epsilon four allele, which is also associated with a higher risk of beta-amyloid deposit and early onset of AD in DS. However, the APOE epsilon two alleles may play a protective role since it is associated with a decrease in amyloid deposition.
Tau protein
Genes in chromosome 21 regulate this intracellular protein found in the neurofibrillary tangles (NFT). The overexpression of these genes may explain the increase in tau protein found in the cortex of persons with DS. [39]
Neurofilament light chain (NfL)
NfL is a scaffolding cytoskeleton protein found in the myelinated subcortical axons. Elevated levels of NfL signify axonal damage. A study conducted on 100 individuals with DS reported a gradual increase of NfL with age, rapidly rising after 40 years. Few other studies have reported increased levels of NfL in AD with DS compared to the control group. Based on rapid isolation, the cost-effective and minimally invasive biomarker NfL can be used as a diagnostic and prognostic tool. [40, 41, 42]
Total cholesterol
Higher total cholesterol levels might be associated with an increased risk of AD in DS, mainly in APOE ϵ four. In addition, the lipid transporter ATP-binding cassette G1(ABCG1) present in chromosome 21 may be related to AD development in DS. If this is true, statins may help prevent AD in DS.
The effect of total cholesterol and statins was evaluated in 123 Caucasian adults with DS. [43] In this study, participants with TC > or = 200mg/dL had twice as much risk of developing AD than subjects with lower TC. However, in those individuals taking statins, the risk of developing AD was less than half that of participants with higher TC levels who did not use statins. This result suggests a beneficial effect of statins; however, there is not enough information to indicate the use of statins to prevent AD in individuals with DS. [44]
Apolipoprotein E
The gene regulating the apolipoprotein E is considered a significant risk factor in the presence of AD in persons without DS. This gene, which has three variants (epsilon 2, epsilon 3, epsilon 4), is involved in several functions, including cholesterol transport, lipid metabolism, and metabolism of beta-amyloid protein in the brain.
In patients without DS, the APOE ϵ four alleles are associated with an increased risk of AD, and the ϵ e2 allele may be protective. [45, 46, 47] Among patients with DS, several studies have demonstrated that the ϵ e2 allele may be protective. Data suggesting that the e4 allele increases risk in patients with DS are less compelling than the data supporting increased risk for patients without DS. [48]
Oxidative stress hypothesis
The accumulation of ROSs resulting from mitochondrial dysfunction in persons with DS leads to abnormal lipid peroxidation metabolism that could lead to structural damage to membranes and the generation of more toxic products. In addition, ROS-related activity also leads to DNA damage.
All these findings lead to the concept that oxidative stress, defined as the lack of balance between the production and the removal of ROSs, might play an essential role in the development of AD in persons with DS; however, oxidative stress alone does not explain the whole process. [29]
The result of this theory was usage of antioxidants as a therapeutic tool in the treatment and prevention of AD and AD in DS. However, this therapy proved to be ineffective. [49]
An alternative hypothesis for the amyloid cascade suggests that increased oxidative stress, secondary to pathogenic factors, increases Abeta, which behaves as a redox sensor. Abeta acting as a redox sensor in this alternative hypothesis attenuates oxidative stress. If this proves to be accurate, oxidative-induced Abeta might be a brain protector. [50]
Brain developmental abnormalities
Several studies have shown anatomic and chemical differences between individuals with DS and the brains of people without DS. [51, 48] Postmortem examinations showed indications of growth retardation in the brains of persons with DS. Among other differences, the brains of individuals with DS showed lower weight, reduced number and depth of cerebral sulci, narrowness of the superior temporal gyrus, and a smaller cerebellum and frontal and temporal lobes. [52]
Microscopic studies have shown the presence of developmental abnormalities, such as reduced dendritic arborizations and irregularities in the size and orientation of spines in pyramidal neurons. These abnormalities have been seen in infancy and even in fetal life. [13, 53] These early changes might contribute to the early onset of AD in persons with DS. In that sense, AD in persons with DS is not a perfect model for understanding AD in persons without DS.
Several genes in chromosome 21 play an essential role in the brain's neurodevelopment and may be responsible for the abnormalities observed in DS. However, how these changes result in AD in DS is not clear.
Cognitive reserve hypothesis
Epidemiologic and brain imaging studies of patients with AD without DS have indicated that patients with limited education or diminished baseline cognitive abilities are at increased risk for AD. These data have led to the cognitive reserve hypothesis, suggesting that patients with better baseline cognitive abilities can tolerate more AD pathology and neuronal loss than patients with worse baseline cognitive abilities. Because most patients with DS have intellectual disability and limited baseline cognitive ability, the cognitive reserve hypothesis would suggest that patients with DS are at increased risk for developing AD.
Initially, this was mostly a quantitative concept. Simply having more neurons with more connections, for example, will allow the individual to tolerate more brain pathology before showing symptoms. A more modern explanation of cognitive reserve suggests that higher cognitive abilities enable the brain to have a better compensatory system. In that sense, the cognitive reserve is more related to brain function than the size or number of neurons. [54]
Studies in persons with AD but not DS suggest that the risk of AD is 2.2 times higher in individuals with less than eight years of education and for those working occupations that require lower skill levels. Interestingly enough, the same studies also suggest that the decline is faster in those with supposedly higher cognitive reserve when the disease starts. [54]
Following this line of reasoning, we could assume that individuals with DS who function at a lower cognitive level should have a higher risk for AD. However, there is no evidence supporting this assumption, and in fact, there is some evidence against it. [55]
Epidemiology
Several studies document that most individuals with Down syndrome (DS) develop Alzheimer Disease (AD). [18, 19] This is unrelated to the degree of intellectual disability. Every 1 in 700 births in the United States is reported to be affected by DS. [56] As a result of research and better clinical management, persons with DS can reach 50 years of age. In the 1920s, the life span of children born with DS was nine years; in the 1960s, it increased to 30 years; in 1993, it reached 55 years, and in 2020, it reached 60 years. [57, 58, 59] In 1996, California reported a life expectancy of a 1-year-old child with DS and profound intellectual disability was 43 years and increased to 55 years in those with the mild-to-moderate degree of intellectual disability. [60] The prevalence of AD in DS is estimated to be about 13.3%, with 55 years at disease onset. [61, 62]
In the author's experience at Wrentham Developmental Center, a facility for persons with an intellectual and developmental disability, the average age of persons with DS at the time of death was 61 years. (range, 47–70 y). Thus, a strong trend is that the frequency of individuals with DS and AD is likely to increase.
Fortunately, in the last two decades, the special needs of older adults with developmental delay, especially those with DS, have gained recognition. Even though early workers in the field presented the issue of aging in developmental delay in the 1960s, [63] the first full session on "The Aging Mentally Retarded” was presented at the 12th Congress on Gerontology, in Germany, in 1981. [64]
Age and trisomy 21 are the most important factors in disease development. Neuropathologic findings related to AD are described in all DS individuals older than 35 years. Early clinical signs and symptoms are observed from the fifth decade to the sixth decade. The mean age at the time of clinical diagnosis is 51 ± 6 years. Most persons with DS may develop AD by age 60–70 years; however, some may remain free of clinical indications of dementia into the late 70s. [7] Several studies described a subset of individuals with full trisomy 21 who do not appear to develop AD, even in old age. [65, 66]
The percentage of people with DS and AD varies in some epidemiologic studies presented. A review of these studies showed that 10–25% of patients had AD when aged 40–49 years, 20–50% had AD when aged 50–59 years, and 60–75% had AD when older than 60 years. In one study, all patients with DS who were older than 70 years had AD. [19]
A cross-sectional study of adults with DS found that the biomarkers followed an anticipated pattern of changes for more than two decades, showing that AD has a prolonged preclinical phase. The study found elevated CSF Aβ1-42/1-40 and plasma NFL levels by 28–30 years. In the fourth decade of life, amyloid PET uptake, 18F-fluorodeoxygenase PET, and CSF p-tau changes are identified, accompanied by hippocampal atrophy and cognitive changes developing during the fifth decade. By the median ages of 50.2 and 53.7 years, prodromal AD and dementia were diagnosed, and the prevalence of symptomatic AD increased to 90–100% by the seventh decade of life. Preventive therapies might benefit these populations based on the similarities between sporadic and autosomal dominant AD and adults with DS. [4]
It is unclear if dementia is more common in persons with a developmental disability when individuals with DS are excluded. A longitudinal study by Strydom et al. [67] evaluated the incidence of dementia in 222 adults older than 60 years (mean age, 68.8 y; standard deviation, SD 7.5; range, 60–94 y) with developmental disabilities but excluded individuals with DS. In this study, the incidence of dementia was five times higher than in individuals without a developmental disability. Other studies on non-DS developmental disability are also in agreement regarding the higher incidence of dementia in a person with a developmental disability. [68, 69]
However, other reports that also excluded persons with DS do not find differences. [70, 71] In addition, when persons with DS were excluded, [72] 1994 autopsy findings in individuals with intellectual disability confirmed that the incidence of AD is the same as in individuals without intellectual disability.
In summary, these and other epidemiological studies indicate that the high frequency of AD in persons with DS is unique, not related to the developmental disability but related to the cause of the DS, and most likely associated with the presence of an extra chromosome 21.
Additional demographic features
No clear geographic distribution exists; a similar clinical picture has been described in other countries. No documentation exists that race influences prevalence.
In patients without DS, the influence of sex on the incidence and prevalence of AD remains controversial. Some, but not all, studies suggest that the prevalence is higher in women than in men. Few studies have evaluated the influence of sex on AD in patients with DS, and the results have been contradictory. [51]
Some indications exist that the onset of dementia is related to early menopause in women with DS. Therefore, it might suggest some role for estrogen in developing AD in women with DS; however, this possibility is not sufficient to offer hormone therapy in this population. [22, 73, 74] There is also an indication that men with DS have an earlier onset of AD than women with DS do [7] ; this suggests that other associated hormonal changes might also be necessary.
Clinical Presentation
This progressive neurodegenerative disorder affects multiple central nervous system (CNS) components. The clinical signs and symptoms express continuous progressive neuronal dysfunction and death. [66, 75, 76]
The most common symptoms seen in individuals with Down syndrome (DS) and Alzheimer disease (AD) are the inability to perform existing skills, memory loss, personality changes, and executive function impairments. [77]
One of the most sensitive and specific symptoms of AD in people without DS is a decline in the patient's ability to perform cognitive tasks related to employment, shopping, or household finance. When individuals with DS are employed or performing complex tasks with a certain degree of personal autonomy, noticing early signs of the disease might not be difficult. Because most individuals with DS have intellectual disability, a history of declining, high-level premorbid cognitive abilities is usually difficult to document. For this reason, approximately 1–2 years elapse between the early signs of the disease and the confirmation of the diagnosis. [17, 51]
Early disease stage
In the author's research, the first symptoms, most often identified retrospectively, are typically observed when the patient is aged 50 years (range, 36–62.5 y), and the diagnosis is confirmed at age 52.6 years (range 37–62 y). However, others have reported early signs of intellectual deterioration in adults in their 40s. [78] Death occurs at a mean age of 60.11 years (range, 46.7–69.8 y). The author's research has also shown that the duration of the disorder from first symptoms to death is 9.10 years (range, 6.9–11.10 y), and the period from diagnosis to death is 8.2 years (range, 5–12.4 y).
The main symptoms are confusion, disorientation, and wandering. Unfortunately, these early signs are not recognized and are commonly misdiagnosed in most instances.
Longitudinal studies showed progressive cognitive decline and slight memory loss as early symptoms associated with deficits in the visuospatial organization. [75, 76] For example, a modified version of the Cued Recall Test [75] showed a high degree of sensitivity (94.7%) and specificity (93.9%) and a high positive predictive value for AD in DS (81.9%)
Behavioral changes in early-stage disease
Deficits and variability in selective attention tests (ie, the ability to stay focused on a particular stimulus, disregarding other stimuli) might be subtle early signs of AD. [79]
In the early stage of the disease, behavioral changes are the most common sign; these changes are usually considered an exaggeration of the long-standing behavioral trait (eg, refusal to follow specific orders or to do chores at home may be perceived as stubbornness).
Because the early changes are subtle, only those familiar with the individual would recognize them (including a change in daily routine, sleeping or eating habits, inability to make clothing decisions, getting lost in typical environments, and failure to remember the names of familiar people). One potential early sign of AD in highly functional DS individuals is the inability to perform job duties.
As the disease progresses, there is an increase in maladaptive behaviors such as aggression, unjustified fears, sleep problems, and inadequate social behaviors. [80]
Visual deficiencies in early-stage disease
Impairment in visual perception as a consequence of central processing dysfunction has been described in the early stage of AD in individuals with DS, who have a relatively high level of intelligence.
Central processing dysfunction is more difficult to delineate in patients with DS who have severe intellectual disability.
These central changes are magnified by peripheral visual disorders (eg, cataracts, myopia, astigmatism), which are frequently present in individuals with DS.
The visual deficiencies may be responsible for individuals getting lost in familiar environments, not performing activities requiring visuomotor coordination, increased frequency of accidents and falls, and difficulty learning new tasks.
Impaired learning ability is usually present in the early stages of the disease but is challenging to demonstrate in people with a moderate or more severe degree of intellectual disability.
Other indications of early deterioration include loss of language and other communication skills, impairment of social and adaptive skills, and progressive loss of activities of daily living (ADLs) (eg, personal hygiene, dining skills, and bathroom skills).
Middle disease stage
In the middle stage, the ability to perform ADLs markedly deteriorates. The patient may depend totally on others for dressing, eating, walking, and toilet needs. Communication skills are reduced markedly; speech and language, if present, are not used efficiently. Behavioral problems are exaggerated, psychotic behavior may be displayed, and social activities are reduced to a minimum.
Advanced disease stage
In the advanced stage, patients are almost vegetative, totally dependent on others, and interact minimally with the environment.
Motor disorders
Motor disorders become apparent in the middle and advanced stages of the disease. They include a progressive gait disorder and, in some patients, a parkinsonian syndrome. The patient is confined to bed in advanced stages with marked rigidity and little voluntary movement.
Eating/swallowing disorders
Eating disorders with progressive dysphagia and frequent choking may be observed initially but are more evident in the middle stage. [81] Aspiration pneumonia is a frequent complication. Changes in the diet and type of food may help alleviate dysphagia. However, in some patients, gastrostomy or jejunostomy tubes might be necessary to permit enteral feeding.
Epileptic seizures
Current evidence suggests that epileptic seizures of the tonic-clonic type have been described. These occur approximately 2.4 years (range, 7 mo–6.1 y) after the disease presents. Usually, generalized tonic-clonic seizures are infrequent; if present, they can be controlled with antiepileptic medication.
Myoclonic seizures occur more frequently than tonic-clonic seizures. The myoclonus may be stimulus-sensitive and induced by light or a simple touch. In the advanced stages, myoclonic seizures may constantly be present. It has been described as late-onset myoclonic epilepsy in DS [82] or senile myoclonic epilepsy. [83]
-
Communication/speech disorder: Early indication of the impairment was observed after an average of 1.4 years (range, 0–4 y; 0 implies the presence of symptoms at the time of first evaluation), and total loss of function occurred approximately 4.5 years (range, 2.5–6.8 y) after confirmation of diagnosis
-
ADLs: Early indication of failure was observed at an average of 5 months (range, 0–1.8 y), and total loss of function occurred 4.5 years (range, 1.5–6.5 y) after confirmation of the diagnosis
-
Ambulation: Early signs of deterioration were observed after 1.1 years (range, 0–3.7 y), and total loss of ambulation occurred 4.6 years (range, 2.5–7.4 y) after confirmation of the diagnosis
-
Leisure activities: Early indications of deterioration were observed after ten months (range 0–2.9 y), and total loss of the ability to participate in leisure activities was seen after an average of 4.1 years (range 1.5–6.5 y)
Illustrative case
A male born in 1930 was admitted to an institution for individuals with intellectual disability in 1939. He died in the institution in 1991, and the diagnosis of DS was confirmed by chromosomal analysis. The following is the author's account of disease evolution in this individual, who was observed from disease onset and demonstrated the complexity of the medical issues involved.
Clinical presentation before the beginning of AD was as follows:
-
The patient had no behavioral problems and was pleasant and congenial
-
The patient followed simple commands and understood simple orders
-
The patient walked independently and also was independent in ADLs
-
The patient consumed a regular diet
-
The patient performed housework and showered well
-
The patient had good leisure skills and an active social program, participated in dances and outdoor trips, and sang with the radio
-
The patient understood that he had to leave the building when a fire alarm sounded
-
The patient's score on the Vineland Adaptive Behavior Scale in 1975, at the age of 45 years, was 4.9 years; this remained the same when he was aged 49 years
The following is a yearly description of the patient's symptoms as he developed AD:
-
1981 (51 y) - The patient's first symptoms were disorientation, confusion, and behavior changes; he refused to accept that the program activity in which he was involved was over. He refused to return to his residence and was found wandering the grounds crying and yelling in a state of confusion.
-
1982 (52 y) - The patient showed increased forgetfulness and had emotional problems and periods of agitation manifested by verbal outbursts and throwing of objects
-
1983 (53 y) - The patient needed consistent prompting to perform ADLs; he was still capable of showering and changing clothes daily; leisure skills were unchanged; he exhibited three incidents of major aggression and agitation; his score on the Vineland Adaptive Behavior Scale decreased to 3 years
-
1984 (54 y) - The patient demonstrated poor participation in social activities as a consequence of frequent sleeping; ADLs required increased assistance, although he remained independent; a choking episode was observed
-
1985 (55 y) - Regression steadily continued; disorientation, confusion, wandering, forgetfulness, and sleeping increased; the patient's behavior deteriorated; he would undress in the dining room and at work; ADLs also regressed, and he needed more help though remaining independent; he frequently was found wandering outside his residence and unable to find his way; occasionally, he could not find his bedroom; the score on the Vineland Adaptive Behavior Scale decreased to 2.1 years
-
1986 (56 y) - The patient exhibited photomyoclonic response; he had myoclonic seizures and difficulty walking; ADLs regressed further; he still could eat and drink but had to be reminded constantly to do so; he was transferred to a safer and more restrictive environment
-
1987 (57 y) - Generalized tonic-clonic seizures appeared; the patient became aggressive, and his gait deteriorated markedly, though he was still able to walk; he occasionally needed a wheelchair; he fed himself using adaptive equipment; toilet training was scheduled, but a few accidents occurred
-
1988 (58 y) - The patient became lethargic; inappropriate behavior became frequent; he no longer was able to walk independently or feed himself; he frequently lost sphincter control; he could not tolerate bus rides into the community; he still enjoyed music and expressed pleasure by smiling and laughing
-
1989 (59 y) - The patient developed aspiration pneumonia and was dependent on ADLs; he required a wheelchair, and his social interaction became very poor; he developed urinary incontinence
-
1990 (60 y) - The patient suffered from frequent bouts of pneumonia; he no longer was able to swallow and was fed through a nasogastric tube; a feeding tube (percutaneous endoscopic gastronomy) was placed; incontinence necessitated the use of diapers; he had minimal interaction with his surroundings and slept most of the time; occasionally, he conveyed pleasure and displeasure by laughing or crying
-
1991 (61 y) - The patient showed minimal response to environmental stimulation and slept most of the time
Etiology of AD in DS
For patients with or without Down syndrome (DS), age is the most critical risk factor for Alzheimer disease (AD) (see also Risk Factors). A few case studies suggest that persons with DS and atypical karyotypes (eg, partial trisomies, mosaicism, or translocations) may have a lower risk of AD than patients with full trisomy. [45] Other chromosome 21 genes, such as the gene coding for superoxide dismutase-1 (SOD-1), may be involved. The increased activity of this enzyme may result in increased production of hydroxy radicals, which may accelerate disease progression. SOD-1 activity has been reported to be increased in people with DS. [48]
Small head circumference, a small brain, a low level of intelligence, and a history of head trauma have also been related to a higher incidence of AD. However, none of these factors has been evaluated in individuals with DS.
Factors that may decrease (eg, a Mediterranean diet or an active lifestyle) or increase (eg, cardiac and cerebrovascular disease or a small head circumference) the risk of AD in patients without DS has not been fully evaluated in patients with DS. [84, 85, 86]
Risk factors for sporadic and autosomal dominant AD are discussed in greater detail elsewhere (see Alzheimer Disease).
Differential Diagnosis and Other Considerations
The differential diagnosis of Alzheimer disease (AD) in patients with Down syndrome (DS) includes the following:
Special concerns
The term mild cognitive impairment (MCI) is used to describe a state of cognitive decline representing a transition between normal cognition and dementia. This state is characterized by impairment in memory and other cognitive functions, as demonstrated by standardized neuropsychological tests. A substantial percentage of patients with the amnestic form of MCI progress to AD within four years of diagnosis. The lack of adequate normative data for memory in DS in different age groups makes the concept of MCI impossible to operationalize in individuals with DS.
The term pseudodementia is used to describe reversible cognitive impairment associated with the psychiatric disease—usually depression. With treatment and amelioration of the psychiatric illness, cognition returns to baseline. However, in patients without DS, many patients who develop AD have symptoms of depression in the early stages of the disease, and the depression itself can impair cognitive function.
Treatment of depression (usually with selective serotonin reuptake inhibitors [SSRIs]) often improves mood and sometimes cognition. However, over the following 24–36 months, progressive cognitive impairment, not necessarily accompanied by mood disturbances, becomes apparent. Unfortunately, data are not available on depression in patients with DS and AD.
Hypothyroidism, observed in almost 30% of individuals with DS, may simulate dementia. Hypothyroidism is frequently present in people with DS and AD; however, treatment with hormone replacement does not change the course of the underlying disease.
Vitamin B-12 deficiency has been reported in several individuals with DS and AD; however, replacement therapy does not change the evolution of the underlying disease.
Although vitamin E helps in reducing oxidative stress, it doesn’t delay the natural course of disease progression.
Individuals with AD and DS present with multiple comorbidities compared to adults with DS without AD. In addition, the frequency of comorbidities increases as the AD becomes more severe. The comorbidities expected are epileptic seizures, lung diseases (mostly aspiration pneumonia), depression, visual and hearing impairment, lack of mobility, and tube feedings.
Other problems to be considered include the following:
-
Depression and other psychiatric disorders
-
Dementia in Parkinson's disease
-
Dementia in progressive supranuclear palsy
-
Multi-infarct dementia
Imaging studies help exclude other causes of dementia, including subdural collections, tumors, and multiple infarcts. Once the diagnosis is established, repeat imaging is indicated when the course of progression is inconsistent with AD (eg, when very rapid deterioration is observed). The dementia screening tests marketed to consumers are of questionable usefulness in persons without DS and of no value in patients with DS. [87]
Laboratory Studies
The workup for Alzheimer disease (AD) in patients with Down syndrome (DS) is no different from that recommended for patients with dementia who do not have DS. Treatable forms of dementia must be excluded.
Laboratory studies include the following:
-
Liver function tests
-
Renal function tests
-
Electrolytes
-
Blood glucose
-
Complete blood count (CBC)
-
Folic acid
-
Vitamin B-12
-
Possibly tests for syphilis and HIV (among patients without DS, these tests are not recommended as part of routine evaluation and should be ordered only when clinically indicated)
-
Thyroid-stimulating hormone (TSH) and thyroxine (T-4) levels (these are likely to be abnormal because of the high incidence of immune-dependent hypothyroidism in patients with DS) [88]
Although the APOE epsilon 4 allele is associated with an increased risk of AD, its use as a diagnostic tool in patients without DS is generally not recommended. There is no role for this testing in patients with DS.
Lumbar puncture is indicated in the evaluation of dementia without DS when conditions could be diagnosed by examination of cerebrospinal fluid (CSF), such as fungal meningitis are reasonable diagnostic possibilities. Most of the time, lumbar puncture is rarely performed to evaluate dementia. These same criteria should be used when the lumbar puncture is considered in patients with dementia and DS. (see Biomarkers).
MRI/CT scans are almost always indicated in the diagnostic workup of persons with dementia, mainly to rule out other pathologies.
Despite many neuroradiological advancements, the radiological evaluation of the brain is not enough to diagnose AD. However, crucial information is provided by the new advances in neuroradiology.
Biomarkers potentially useful for early diagnosis
Biomarkers, physical signs, or lab tests consistently associated with a particular disease help confirm the diagnosis, monitor the condition, evaluate treatment efficacy, and facilitate early intervention to delay disease progression.
Unfortunately, at present, there are no reliable biomarkers helpful in diagnosing AD and DS, nor are there good predictors of disease progression or treatment response. However, potential biomarkers have been and continue to be investigated.
Tau protein and beta-amyloid(1-42) (Abeta42) peptide levels in CSF might help differentiate AD from other dementias. Low Abeta42 and high tau protein levels might be associated with a higher risk of AD. [89, 90]
Abeta42, total tau protein, and tau phosphorylated at position threonine 181 (P-tau) levels in CSF have sensitivity and specificity enough to allow AD identification compared with cognitively normal elderly persons. In addition, these biomarkers can recognize patients with mild cognitive impairment (MCI) who progressed to AD and those who did not. However, repeated lumbar punctures to monitor the improvement of a potential treatment limited the utility of these markers as front-line screeners.
Plasma levels of beta-amyloid (1-42) (Abeta42) were higher in persons with DS and dementia than in persons with DS and no AD. [7] Also, higher levels of Abeta42 peptide in non-demented persons with DS were also predictors of dementia and increased mortality. Beta-amyloid 1-40 did not show any correlation. [91] At present, they are not considered to be routinely indicated for the evaluation of persons with DS and potential AD. [90]
Blood biomarkers might be more efficient and cost-effective than CSF biomarkers or radiological tests. However, there are several difficulties in finding the more appropriate ones. [92] Although many biomarkers have minor diagnostic potential, plasma NfL is minimally invasive and cost-effective; it can be used for diagnosing AD in DS. [42]
Numerous research studies are being conducted to standardize biomarker levels, to use them as both diagnostic and prognostic tools. The Alzheimer’s Biomarkers Consortium-Down Syndrome (ABC-DS) is a clinical trial currently working to track AD biomarkers (Aβ, tau, CSF biomarkers, neuroimaging, neuropathology) along with cognitive and functional measures in more than 400 individuals with DS. [93, 94]
The Horizon 21 Down Syndrome Consortium is a large, ongoing, longitudinal study with more than1000 individuals with DS on biomarkers of AD-related cognitive and clinical changes from various research groups. These groups include the London Down Syndrome Consortium [LonDownS] and the Cambridge Dementia in Down’s Syndrome [DiDS] cohort), Netherlands (the Rotterdam Down syndrome study), Germany (AD21 study group, Munich), France (TriAL21 for Lejeune Institute, Paris), and Spain (the Down Alzheimer Barcelona Neuroimaging Initiative (DABNI). [42, 94]
The Alzheimer’s Clinical Trial Consortium - Down Syndrome (ACTC-DS) is an NIH-funded study conducting its first research on Trial Ready-Cohort - Down syndrome (TRC-DS). TRC-DS will longitudinally follow 120 individuals with DS, without dementia, using fluid biomarkers, neuroimaging, and cognitive testing. ABC-DS and Horizon 21 projects are secondary prevention trials; ACTC-DS will invest its expertise in developing new therapies for AD in individuals with DS. [42, 94]
Telomere shortening
Telomeres are sequencing of DNA at the end of the chromosome that get shorter with the cell division and, indirectly, are a measure of cell aging. Shortening of the telomere has been reported in AD patients without DS. Lymphocytes have shown shortened telomeres. A similar association has been reported in persons with DS and dementia. [95] Telomere shortening may be a biological marker of dementia status, but more research is needed.
Brain CT Scan
Studies that used computed tomography (CT) to compare young individuals who had Down syndrome (DS) (19–34 y) compared with healthy individuals without DS found no significant differences between the two groups concerning white- or gray-matter volumes or ventricular volumes. [96]
Quantitative studies with CT scanning and magnetic resonance imaging (MRI) demonstrated that young adults with DS have no ventricular dilatation, atrophy, and consistent malformation that could explain the intellectual disability. However, small brain size was reported consistently. It is probably an expression of small stature and a small cranial vault. [96]
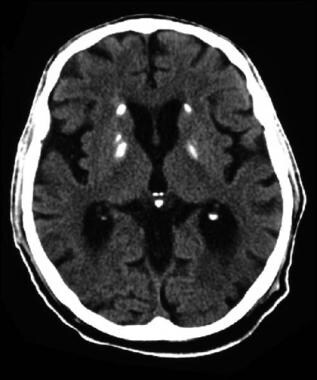
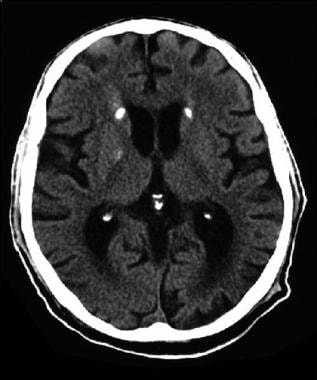
Bilateral symmetric basal ganglia calcification is a frequent finding in people with DS (see the images below); it is more prevalent in this population than in the general population. However, its relationship with the clinical presentation of Alzheimer disease (AD) in DS is unclear.
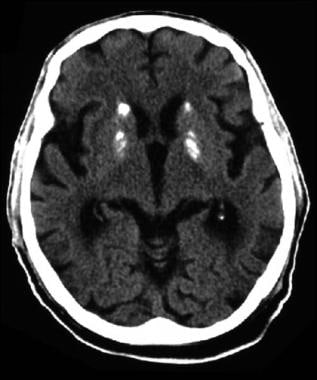 CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
 CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
 CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
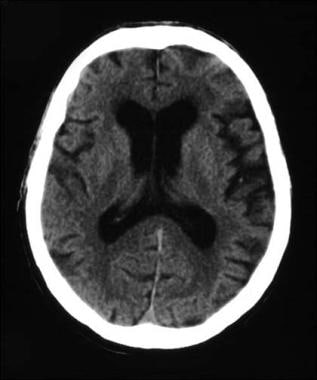
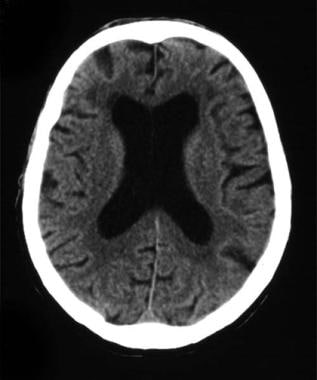
The results were different when people with DS and cognitive deficiencies were compared with individuals who did not have cognitive deficiencies. In individuals with DS and cognitive deficiencies, cerebral atrophy and ventricular enlargement that suggested brain atrophy were reported consistently (see the images below).
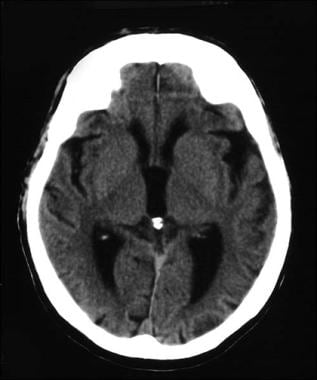 CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
 CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
 CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
In advanced cases, atrophy was generalized. However, regional differences can exist with greater involvement of the temporal horns. The relation between enlargement of the temporal horns of the lateral ventricles and dementia in elderly DS patients has been a consistent feature.
Brain MRI
Magnetic resonance imaging (MRI) studies have documented several developmental findings in persons with Down syndrome (DS), including the following:
-
Reduction in the whole brain volume (including cerebellum) and in the gray and white matter of the brain
-
Reduction in the volume of the hippocampus
-
Focal decrease in the volume of the frontal and occipital lobes
-
Relative preservation of the temporal lobe with decreased planumtemporale and the superior temporal gyrus volume
MRI studies might show a decrease in the volume structures of the temporal lobe (eg, the hippocampus and the adjacent medial temporal lobe) in persons with DS who do not have dementia. Significant atrophy of the corpus callosum, an indication of neocortical atrophy (more evident in the splenium), has also been demonstrated in persons with DS before the development of Alzheimer disease (AD).
Grey matter changes are identified even before the symptoms of dementia develop. [97] The reduction of grey matter volume is correlated with amyloid accumulation. It is hypothesized that amyloid accumulation leads to atrophy and worsens over time in dementia. [98]
MRI findings in symptomatic individuals are similar to those of computed tomography (CT) and reveal progressive atrophy of the brain with enlargement of the ventricular system.
MRI volumetric analysis of selective brain areas involving 19 adults with DS and AD and 39 adults with DS without AD found smaller volumes bilaterally in the hippocampus and caudate, right amygdala, putamen, and a larger volume of left peripheral CSF in individuals with DS and AD. This study suggests that significant medial temporal and striated volume reductions may be a reliable AD marker in individuals with DS. [99] However, age-related reduced volume in frontal, temporal, and parietal lobes, as well as an increased volume of peripheral CSF, have also been described in individuals with DS without clinical indications of dementia. [100]
These observations are in agreement with prior studies reporting cerebral atrophy and ventricular enlargement, suggesting brain atrophy in individuals with DS when cognitive deficiencies were present, [96] or when regional differences with more involvement of the temporal horns were reported. [101]
Diffusion tensor imaging (DTI) is an advanced MRI technique that is non-invasive and helps evaluate white matter's (WM) microstructural properties. DTI measures the rate and direction of water molecules diffusion in neural tissue. DTI has been used extensively to study brain aging and disease states such as AD.
Fractional anisotropy (FA) measures white matter changes and is expressed as 0, representing poor white matter integrity, or 1, representing good white matter integrity. A study involving 25 individuals with DS, ten of whom had AD, showed lower FA values, mainly in frontal lobe circuits, in adults with DS compared with controls. Furthermore, in individuals with DS, the abnormalities in the white matter were also associated with decreased performance in frontal executive functions with no cognitive decline. [102] These findings may help us understand why frontal-dependent behavioral and executive function changes are among the earliest signs of AD.
Fenoll et al. reported a reduction in WM integrity and WM degeneration is not accelerated in non-dementia individuals with DS as DTI sensitivity might be limited during the early stages. [103] More research studies are needed to understand the relationship between the DTI parameters and WM changes seen in this population.
These observations summarize that CT/MRI studies in individuals with AD and DS consistently demonstrate abnormalities, even in the early stages of the disease; however, this might not be enough to establish the diagnosis of dementia, and clinical correlation is always needed. In addition, serial CTs and/or MRIs might be required to differentiate older persons with DS who have dementia from those who do not. In addition, CT/MRI is beneficial to rule out other causes of neurological deterioration.
Other Studies
Positron emission tomography
Positron emission tomography (PET) is not considered a routine test for Alzheimer disease (AD) in individuals with Down syndrome (DS). Schapiro et al. found that PET did not demonstrate any difference between healthy people with DS and individuals without intellectual disability. [104]
Studies with xenon-133 inhalation technique, which evaluates cortical cerebral blood flow, showed no abnormalities in young, healthy people with DS. Significant differences were observed in individuals with DS and dementia; the greatest reduction occurred in the parietal-temporal association neocortex. [96] In addition, errors in the interpretation of PET scans occur, with a tendency to overdiagnose dementia. [105]
Even though there are limitations in the use of this technique, amyloid PET imaging offers a quantitative and qualitative method to measure β-amyloid deposition in the brain. Deposition of β-amyloid has been reported in studies using carbon 11-labeled Pittsburgh Compound B ([(11)C]PiB), [18F] florbetapir, and [18F] florbetaben PET imaging. [106, 107, 108, 109, 110]
In general, these studies agree that an increase of β-amyloid in the brain is age correlated and precedes the development of cognitive changes by many years. The usefulness of these studies in diagnosing AD is questionable since findings are also present in non-demented individuals. However, in the event of the development of anti-amyloid treatments, these tests might prove to be helpful.
Electroencephalography
Patients with DS have a high baseline prevalence of seizures, and the prevalence increases further as patients develop AD. Therefore, it is prudent to obtain an electroencephalogram (EEG) in the baseline evaluation of a patient with DS and dementia. However, this test does not help diagnose dementia since no specific patterns correlate with dementia. There is deterioration in the background activities as dementia progresses, with an increased slowing in the whole brain and loss of typical structures. In addition, at one point in the disease, the EEG may show epileptic form activity.
Adults with DS can have decreased amplitude of alpha waves similar to AD adults. Salem et al. reported a reduced frequency of theta-1 waves in AD adults with DS compared to individuals with DS. The most common form of epilepsy seen is senile myoclonic, which progresses to non-epileptic myoclonus in later stages of dementia. Further research on EEG combined with neuroimaging would help understand dementia progression. [111, 98]
Retinal imaging
Retinal imaging by optical coherence tomography is an upcoming neuroimaging mode to study dementia. In individuals with AD, this technique showed a decrease in retinal thickness and macular volume, correlating with cognitive decline. AB accumulation is noted in both lenses and retinal cells in individuals with DS. However, more studies are needed to understand the relationship between amyloid accumulation and cognitive decline in DS. [97, 98]
Dementia Scale and Questionnaire
The diagnosis of dementia still is based primarily on clinical history and examination. Generally, the diagnostic methods used for testing persons without developmental disabilities, (eg, Mini-Mental Status Examination [MMSE] or similar) are unreliable for diagnosing dementia in persons with developmental disabilities. Additionally, standard neuropsychological tests cannot evaluate many people with developmental disabilities.
There is no universally accepted protocol for diagnosing individuals with intellectual disabilities. Guidelines for diagnosing dementia, with around 90% accuracy in individuals without developmental disabilities, have been published by different associations. [112, 113, 114, 115, 116]
An evidence-based guideline released by The Global Down Syndrome Foundation Medical Care Guidelines for Adults with Down Syndrome Workgroup recommends screening for Alzheimer-type dementia from 40 years of age. Other recommendations include managing the risk factors of cardiovascular disease and stroke prevention, obesity screening, and secondary causes of osteoporosis evaluation. Although this guideline provides guidance to adults with DS, further research and studies are needed for high-quality evidence. [117]
However, these diagnostic tests are difficult to apply in persons with developmental disabilities, and several other tests have been designed that are more appropriate. Generally, these tests emphasize a change in function as measured by a decline in activities of daily living (ADLs), such as eating, dressing, and bathing. [118] The use and the validity of these instruments have been extensively discussed. [119]
Some tools that have proved to be very useful [120] are the Dementia Scale for Down Syndrome (DSDS), [121, 122] which was specifically designed to be used in individuals with DS, and the Dementia Questionnaire for Mentally Retarded Persons. [123]
The DSDS was developed to detect cognitive deficiencies mostly in persons at the lower end of the cognitive scale; even though the test specifically refers to DS, it could be used in any person with a moderate-to-severe degree of intellectual disability. The DSDS and the Dementia Questionnaire for Mentally Retarded Persons can differentiate, with high specificity and especially high sensitivity, between persons with DS who have AD and those who do not. [120] There are no significant differences between the two tests.
Also potentially useful are part I of the American Association on Mental Deficiency Adaptive Behavior Scale (ABS), the Reiss Screen for Maladaptive Behavior, [124] and the IBR Evaluation of Mental Status (IBREMS).
However, in current practice, there is no single battery of tests that can determine the presence of dementia in individuals with developmental disabilities with one single administration. [118] One serious problem in assessing cognitive decline in persons with developmental disabilities is that they already had at least a mild-to-moderate degree of cognitive deficiency before they developed AD. [120] Also, persons with poor education or low-to-moderate cognitive level can be wrongly diagnosed with cognitive decline because of poor performance on the standard tests. [125]
Despite these limitations, several tools are available that may help to document the diagnosis of dementia in individuals with DS. Because the diagnosis of AD is based on the demonstration of a functional decline, a baseline observation of the individual's cognitive abilities is very important. Sometimes this information can be found in the patient's medical and school records, from family observations, or through direct observation of the patient participating in supervised adult activities. Tests that use caregivers as a source of information may be more reliable than tests directly involving the individual. [118]
Alzheimer Functional Assessment Tool
A simple tool for evaluating the clinical progression of Alzheimer disease (AD), developed by the Alzheimer team at the Wrentham Developmental Center in Massachusetts, is the Alzheimer Functional Assessment Tool. This tool was designed to record critical information on the status of patients with AD and assist in making decisions concerning the patient's program and residential placement. The information needed to complete the assessment can be obtained by interviewing relatives or caregivers.
Interview the staff on all shifts that work directly with the patient, and find out the patient's behavior and overall activities of daily living (ADLs). The "description of skills" section describes the patient's abilities (including skills, problems, and other considerations). Perform this assessment at the time of AD diagnosis and every six months or with a significant change in status.
The Alzheimer Functional Assessment Tool is appropriate for the follow-up care of individuals with Down syndrome (DS) and AD. A decline in functions documented in the tool can be used as a diagnostic test; however, the device was not intended to be used for diagnostic purposes and has never been validated as a diagnostic test. Serial use of this tool can also help evaluate medications' effects and determine the support needed for these patients.
The Alzheimer Functional Assessment Tool includes the following information:
-
Date
-
Name
-
Activities of daily living
-
Description of skills
-
Toileting
-
Dining
-
Walking/motor
-
Bathing
-
Dressing
-
Personal/oral hygiene
-
Environmental awareness
Scoring for Alzheimer Functional Assessment Tool
Each of the following assessments is preceded by the number representing the progression of the individual's deterioration. We recommend an evaluation every six months and change the plan of care as needed based on disease progression.
Toileting
Toileting is measured by the following:
- Can use the bathroom in familiar and unfamiliar environments independently
- Goes to the toilet independently or asks staff to assist; may need reminders to use toilet paper and wash hands
- Has occasional toileting accidents; needs a verbal reminder
- Needs staff to take to the bathroom on a schedule; remains continent 90% of the time
- Needs staff to take to the bathroom on a schedule; remains continent 50% of the time or less
- No bowel or bladder control; may require frequent changing or special clothing (eg, pads, diapers)
Dining
Dining measurement includes the following:
- Can prepare simple food, eg, sandwich, toast); can set the table and clean up after meal; uses knife and fork to cut food; may or may not use adaptive equipment to eat independently
- Can use fork and spoon to eat independently but needs food to be cut
- Eats independently with the help of adaptive equipment
- Can use fork and spoon to eat independently but may need occasional prompts to start or continue eating; may finger feed; needs food to be cut
- Needs physical assistance to complete the meal
- Develops swallowing problems; needs change in consistency of food or thick drinks
- Completely dependent; may need specialized feeding program
Walking/motor
Ambulation measurement includes the following:
- Independent ambulation; able to walk steadily; able to start, stop, and change direction without falling; able to walk fast or run; ascends and descends stairs; capable of leaving premises without assistance
- Independent ambulation for short distances; walk up and down the stairs 1 step at a time by holding rails; able to leave premises without assistance
- Independent but cannot negotiate stairs; unable to leave premises without assistance
- Can walk without support but requires supervision; may be unsteady; requires supportive measures at times
- Needs assistance (another person to hold, walker) to walk; "cruises" around using structures such as furniture and walls as support; unable to leave premises independently
- Needs wheelchair but can move independently
- Needs an adapted wheelchair and cannot move independently; needs to be pushed
Bathing
Bathing ability is measured by the following:
- Can independently carry out an appropriate bathing routine (disrobing, washing, drying, and dressing)
- Can carry out an appropriate bathing routine with occasional reminders to do a step or wash more thoroughly
- Needs verbal prompts to initiate and/or complete some steps in the bathing process (due to subtle confusion and/or fear); continuous staff supervision at shower time not necessary; may use toiletries inappropriately
- Requires continuous staff supervision at shower time to ensure complete bathing and safety (eg, problems due to confusion and/or fear); hand-over-hand assistance may be necessary at times; alternatives to showering or a specialized program may be recommended due to fear of showering; safe use of hot and cold water needs to be monitored
- Primarily passive during bathing; requires some form of assistance for all steps; may be able to stand and move a body part when given a verbal or touch cue; fear of water may be present
- Physically and cognitively unable to participate actively in the bathing process; may respond to stimulation during bathing with vocalizations or changes in facial expressions
Dressing (skills and appropriate dress)
Dressing skills are identified as follows:
- Dresses independently or with physical assistance due to handicap; can choose appropriate clothing (for weather or activity of the day) and cares for own clothing (eg, places dirty clothes in the hamper, hangs clothing, stores properly)
- Occasionally needs reminders to dress appropriately ("It's cold out today") and to care for clothes ("Remember where your dirty socks go?")
- Dresses with minimal assistance or verbal prompts
- Dresses inappropriately for the weather (layers clothing and/or puts clothing on inappropriately); may undress at an inappropriate time and/or place; may benefit from adaptive clothing to retain dressing skills; does not attempt to care for own clothing
- Needs assistance in dressing (50% or more of task) and may be resistive; may assist when compliant (eg, puts an arm through sleeve)
- Lies passively during dressing; does not respond to dressing or undressing
Personal/oral hygiene (hair brushing, teeth brushing, sanitary pad, shaving)
Hygiene maintenance is measured by the following:
- Able to perform all personal hygiene tasks
- Able to perform all personal hygiene tasks within regular routines; may show difficulty in performing tasks if the routine is changed (eg, hospitalized, moved)
- Able to perform all personal hygiene tasks but requires occasional reminders from staff to complete the task
- Able to perform personal hygiene tasks but requires frequent reminders from staff to complete the task; may need staff guidance (verbal and point cues) in some parts of some tasks (i.e., may forget steps); may still be proficient in one area and lose ability in another area
- Requires staff supervision (verbal and point cues) to complete some personal hygiene tasks and staff assistance (light, moderate physical cues) to complete others
- May still be able to perform some steps of some personal hygiene tasks with staff assistance but depends on staff to meet other personal hygiene needs
- Depend on staff to meet all personal hygiene needs
Environmental awareness
Awareness of the environment is noted by the following:
- Cognizant and responsive, in a relevant way, to familiar and unfamiliar people and other environmental stimuli
- Generally responsive to familiar and unfamiliar people and situations but seems self-absorbed and/or confused most of the time
- Cognizant and responsive in a relevant way to familiar people and situations but shows a delayed or inappropriate response to unfamiliar people and situations
- Cognizant and responsive to stimuli, but the response is often inappropriate, even in familiar situations
- Mostly awake but seems self-involved, showing little or inconsistent response to the environment
- Sometimes awake but shows little interest in surroundings; sleeps at other times
- Sleeps most of the day; needs to be aroused repeatedly to maintain interaction
Treatment of AD in DS
The medications below have been recommended or used in individuals with Alzheimer disease (AD). Donepezil, and rivastigmine, are the only drugs approved by the FDA for the treatment of AD investigated in individuals with Down syndrome (DS). [126, 127, 128, 129]
Acetylcholinesterase inhibitors
Four acetylcholinesterase inhibitors (tacrine, donepezil, rivastigmine, and galantamine) have been approved by the US Food and Drug Administration (FDA) for the treatment of AD in patients without DS. Tacrine is no longer used because its potential liver toxicity necessitates frequent blood monitoring. These drugs are approved for mild-to-moderate dementia. Donepezil remains the only cholinesterase inhibitor also approved to treat patients with severe dementia.
Memantine, a partial N -methyl-D -aspartate (NMDA) antagonist, is approved for the treatment of moderate-to-severe AD.
The efficacy of the choline transferase inhibitors in AD in patients without DS is modest, and the available data have not convincingly demonstrated that these drugs influence the overall progression of the disease. Nonetheless, industry-sponsored studies have shown that AD patients without DS who were treated with these medications may require nursing home placement one year later than patients who were not so treated.
Cholinetransferase inhibitors might be expected to produce the same results in persons with DS. However, AD in patients with DS is often diagnosed later than AD in patients without DS. In addition, most studies of cholinesterase inhibitors were conducted in patients with mild-to-moderate disease, and efficacy in patients with severe disease is less well established.
The efficacy of memantine is also modest. Indeed, its effect size is only half that of the choline transferase inhibitors. Memantine also does not slow the progression of the disease. Some believe its efficacy decreases baseline noise in information processing associated with excess glutamate. A meta-analysis showed that memantine monotherapy might have a beneficial effect on persons with AD (DS not included), [130] but other studies do not confirm these results. [131]
Several studies in patients without DS suggest that both the cholinesterase inhibitors and memantine may effectively treat secondary symptoms of AD (eg, agitation). Given that both groups of medications usually have fewer side effects than neuroleptics do, a trial of a cholinesterase inhibitor or memantine to control secondary symptoms of AD before neuroleptic therapy may be warranted.
Few clinical trials of the choline transferase inhibitor donepezil have been performed in patients with DS and AD. Results have been negative or have consisted of modest benefits that were not sustained for more than a few months. [132, 133, 134, 135, 136, 126, 127]
A Cochrane review of the use of donepezil in persons with DS found a modest and statistically non-significant benefit in persons with DS and AD who could tolerate the adverse effects of the medication. [128]
A small study involving three individuals with DS showed that donepezil treatment resulted in urinary incontinency in two. [133]
Some improvement in cognitive functions with donepezil was reported in another small study involving four individuals with DS. [135]
In a 24-week, double-blind, placebo-controlled, parallel-group involving 30 persons with DS and mild-to-moderate AD, the average age in the placebo group was 55 years (range, 45–62 y) and 53 years (range, 40–69 y). There was a non-significant reduction in deterioration in the treatment group as measured by the Dementia Scale for Mentally Retarded Persons, Severe Impairment Battery, and the Adaptive Behavioral Scale. The tolerance for donepezil was good. [137]
Boada Rovi et al. al (2005), in an open crossover study involving 14 individuals with DS older than 40 years and diagnosed with possible or probable dementia receiving 5 mg of donepezil during the first month of treatment and 10 mg for the next five months, found improvement in cognition and social activities in the first three months of the donepezil-phase of the study, but no difference with the control group at the end of the study.
Improvement in daily activity was observed with a low dose of donepezil (3 mg/day) in a group of 21 women with DS (aged 32–58 y; mean, 45.6 y) and severe cognitive impairment. [138] In this study, donepezil treatment was beneficial for DS patients in the early part of the treatment phase and was never reduced throughout the trial. In addition, most of the patients had IQs below 20, suggesting that donepezil treatment could be beneficial even for severely impaired patients.
Regarding rivastigmine, a retrospective study [51] involving 17 patients with DS and AD received a starting dose of 1.5 mg twice daily and gradually increased up to 12 mg/day over eight weeks. The study showed that individuals treated with rivastigmine had less of a decline, over 24 weeks, in global functioning and adaptive behavior when compared with an untreated group; however, the difference was not statistically significant.
A Cochrane review of the use of rivastigmine in people with DS found four studies addressing this issue, but three were excluded because they did not meet the standards requested, and one was awaiting assessment. The conclusion was that there was no evidence that rivastigmine is useful in this population. [139]
A Cochrane review of the use of galantamine failed to find any study in this population. [140]
A more recent meta-analysis of the use of these medications in persons with DS again failed to show the benefits of donepezil and memantine. Also, participants who received donepezil were significantly more likely to experience an adverse event. [141]
NMDA receptor antagonists
Memantine is the only drug in this group approved for use in AD. A 2009 Cochrane review found no studies for inclusion. [142] Subsequently, a randomized, double-blind, placebo-controlled study of memantine for dementia in DS patients older than 40 years found no evidence of efficacy. [143] This was also confirmed in a 2015 Cochrane review. [141]
Other drug therapies
Several classes of drugs have been tested in persons with AD without DS. Neuroinflammation may have a role in the pathogenesis of AD, [144] but clinical trials with anti-inflammatory drugs have failed to show consistent efficacy.
Drugs that decrease the accumulation of amyloid-beta (Abeta) in the brain have been tried in persons with mild AD without DS. Even though the tolerance was good and there was a reduction in Abeta 42 in the cerebrospinal fluid (CSF), there was no significant clinical impact. [145] Trials involving active immunization of patients with Abeta were halted because 7% of patients developed encephalitis. How adequate immunization was in slowing the progression is controversial in this trial.
Other therapeutic options to study in upcoming clinical trials include anti-tau immunotherapy and APP downregulation via anti-sense oligonucleotides. [94]
Estrogen epidemiologic data suggested that postmenopausal women taking estrogen decreased the risk of developing AD. However, a clinical trial testing this hypothesis among women older than 65 years who had a family history of AD was halted because the women treated with estrogen appeared to have an increased risk for dementia. Data suggest that estrogen therapy may have a protective role if started in younger women at the onset of menopause. Present evidence does not support the use of estrogen for the treatment or prevention of AD.
One study involving simvastatin showed a slight improvement in cognitive function. [141]
Antioxidants
Data suggest that free radicals may contribute to neurodegeneration in AD, but clinical trials have not consistently shown antioxidants to be efficacious. Several studies have addressed this issue, few of them in persons with DS.
A study of the use of lipoic acid in persons with DS failed to show any clinical impact. [146] A Cochrane report also found no evidence of benefit and suggested that lipoic acid should not be recommended for the treatment of dementia. [147]
Administration of acetyl-L-carnitine to improve visual memory and attention was reported in the only study done in persons with DS. This effect was not seen in a control group of persons with mental deficiency but no DS, suggesting specificity. [148] Other studies in persons with mild cognitive impairment and AD also showed some improvement. Acetyl-L-carnitine was given to 40 individuals with DS in a double-blind protocol for six months, but it yielded no benefit in persons with DS. [149] At present, routine use of this medication is not recommended.
A 2-year randomized, double-blind, placebo-controlled trial assessed daily oral antioxidant supplementation (900 IU of alpha-tocopherol, 200 mg of ascorbic acid, and 600 mg of alpha-lipoic acid) in 53 persons with DS and dementia. [150] Although supplementation was safe, it yielded no improvement in cognitive function or stabilization of cognitive decline.
Increased antioxidant effects in cells in patients with AD may improve some symptoms; however, a Cochrane meta-analysis found no evidence to support the use of melatonin in persons with dementia. [151]
Some studies suggested that diets containing high amounts of vitamin E could prevent dementia; [152] however, other studies disagree. [153] A Cochrane review also found no solid evidence for the use of vitamin E in AD but identified enough benefit to justify further studies. [154]
Vitamins B-6, B-12, and folic acid are cofactors in the metabolism of homocysteine that might accumulate if these vitamins are deficient. A high level of homocysteine is a risk factor for AD development. Administration of 5 mg/day of folic acid, either alone or in combination with 5 mg/day of vitamin B-6 or 100 μg of B-12 (or both; see folic acid/cyanocobalamin/pyridoxine), decreased the blood levels of homocysteine in persons with DS. [155] No other studies have evaluated the use of these vitamins in persons with DS. In general, the evidence available does not demonstrate a beneficial effect of the sevitaminsin in preventing or treating AD.
The herbal product ginkgo biloba is probably the most commonly used alternative treatment for the prevention of age-related cognitive decline. [156] The information available is still controversial, with studies showing some mild benefits and others failing to show any positive change. [157] The only study of ginkgo involving two teenagers with DS showed some social and academic skills benefits. [158]
Curcumin is an herb used to preserve food; it is widely consumed in India and might be related to the lower incidence of AD in India. In addition, curcumin is a potent antioxidant and anti-inflammatory. However, there is no investigation of the effect of curcumin in persons with DS. A 2015 meta-analysis failed to show a benefit with antioxidants. [141]
Nonsteroidal anti-inflammatory agents
Some studies have suggested that nonsteroidal anti-inflammatory drugs (NSAIDs) might be beneficial; however, no studies have been done in persons with DS.
Psychotropic medications
Typical and atypical neuroleptics are often used to treat agitation, aggression, and hallucinations in patients with AD without DS. A black box warning from the FDA warns about the use of atypical neuroleptics in patients with dementia. Nonetheless, most experts still occasionally use atypical neuroleptics (eg, quetiapine) with the minor extrapyramidal side effects in treating AD patients with agitation. Therefore, physicians need to inform patients' families that they prescribe such medications despite the black box warning.
The use of atypical antipsychotic medications in persons with AD but no DS for the treatment of aggression, psychosis, or agitation showed that the adverse effects offset the benefits. [159]
Other medications
Small trials have examined using antiseizure medications such as valproate, carbamazepine, and lamotrigine for treating agitation in AD. Results have been inconsistent.
Selegiline is a neuroprotective medication that might benefit persons with DS. [160] A Cochrane meta-analysis of selegiline failed to show any positive effect. This medication has not been evaluated in persons with DS. [161]
In many instances, medications might be needed to treat the frequent comorbid conditions observed in persons with DS. [162]
Surgical care
Some patients may require placement of a feeding tube, and some patients may need a tracheostomy.
Consultations
Consult a neurologist, a gerontologist, or both for diagnosis, advice, and follow-up care. Consult rehabilitation specialists as well. Consult an ethics specialist regarding resuscitation or hospice care decisions in advanced stages.
Diet
No particular diet is required. However, dysphagia may become a prominent feature as the disease progresses, and food texture changes are recommended. These individuals might need a dietitian's help at this stage. In advanced stages, limited intake may be associated with severe weight loss, and should consider a feeding tube.
Activity
Animal studies have shown that physical exercise or environmental enrichment can increase growth in some brain areas. Based on this finding, Head et al. suggested that the application of these ideas might have a significant positive impact in aging persons with DS. [65] These ideas have not been scientifically proven in persons with DS; however, a good comprehensive plan for AD should include various physical and social activities.
Further inpatient care
Inpatient care is unnecessary, except when patients present with acute medical complications. In the advanced stage, institutionalization may be required, and hospice care might be an option to consider. [163]
Further outpatient care
Most services are provided in the outpatient setting. Consult a team that has experience in managing AD patients with DS.
Transfer
When the severity of dementia creates dangerous situations, individuals with AD should be transferred from their usual living conditions. The ideal approach is to obtain support from the family or arrange for caretakers to maintain a familiar and friendly environment.
Deterrence/prevention
At present, there is no known method or treatment for AD prevention. However, some epidemiologic studies have evaluated the importance of lifestyle, diet, and other risk factors. [164, 165] Trials are being performed with ginkgo biloba, NSAIDs, estrogens, vitamins E and C, and beta-carotene, but there is no clear evidence of positive results. [84, 85, 166, 167]
Complications
Good nursing care is needed to prevent complications (eg, decubitus ulcers, aspiration pneumonia, deterioration of gastroesophageal reflux, fractures, dysphagia, urinary tract infections, and accidents).
Patient Education
Discuss issues related to diagnosis and prognosis with the family and caregivers early in the course of the disease. In addition, establishing rapport with a team specializing in Alzheimer disease (AD) management is beneficial. For patient education information, see the Dementia Center.
Caregivers are an essential component in the care of persons with AD. In most instances, caregivers are family members. Caregivers endure a significant burden that might result in physical and emotional disorders. [168] Accordingly, a good program for the treatment of persons with AD, with or without DS, should include education for and protection of the caregivers.
A program consisting of two sessions of individual therapy for the caregiver of an individual with AD (usually the spouse); four sessions of family counseling, support group participation, and continuous availability of phone counseling for the caregiver resulted in a 28.3% reduction in nursing home placement and a delay of almost a year and a half in the admission to a nursing home. In addition, the positive results were achieved without a negative impact on caregiver well-being.
Individuals with DS are considered independent adults once they reach the age of 18 years. Instruct parents to obtain legal guardianship through the courts; otherwise, any authorization provided by the parents has no legal value. Discuss issues such as surgical procedures, placement of feeding tubes, and hospice care with the legal guardians.
Neuropathology
The neuropathology of Alzheimer disease (AD) in persons with Down syndrome (DS) closely resembles that of AD in persons without DS. [9, 10, 11, 12, 13] Autopsy studies in persons with DS showed that almost all had brain lesions meeting the criteria for AD. [14, 15] As has been observed in persons without DS, autopsies of patients with DS showed the hallmarks of AD: intraneural neurofibrillary tangles (NFT) (mainly composed of tau protein, which is encoded by the microtubule-associated protein tau gene [MAPT]), extracellular neuritic plaques, amyloid angiopathy, and deposits of amyloid-beta (Abeta) protein in senile plaques. [14, 169]
In persons with DS, the Abeta deposits can be seen in the cerebral cortex as early as in their 30s. [170, 171] The distribution of these brain abnormalities along with structural and chemical composition is the same in persons without DS; however, there are some differences. For example, persons with DS have an earlier and greater deposition of plaques and tangles in the hippocampal area. [172] In addition, the deposition of beta-amyloid is lower in the cortex in persons with DS compared with those without DS and AD. [173] Also, the amyloid plaques are not homogenous and are also bigger in individuals with DS than in those without DS. [174] Diffuse plaques composed of non-fibrillary deposits of Abeta amyloid, usually not associated with other cytological changes, developed earlier than the dense core plaques that are associated with neuronal and glial changes. [175] These diffuse plaques seem to be a unique feature in DS and are seen in children with DS as young as eight years. [176] They seem not to have an important effect on neurons and do not result in clinical symptoms. [177]
Amyloid also deposits in arterial walls. However, and differently in the non-DS population, vascular dementia is unusual in persons with DS. [178]
Even though amyloid is deposited in the brains of persons with DS very early in life, the deposits are not directly related to the clinical picture. On the contrary, NFT, never reported in the absence of hardcore amyloid, increases in density later in life and is more directly related to the early signs of AD in DS than the presence of amyloid. [179, 180] NFT are intraneuronal, abnormal, twisted filamentous proteins composed mainly of hyperphosphorylated tau proteins. [181] This might indicate that changes in tau protein are more responsible for neuronal dysfunction and clinical symptoms.
Other neuropathological abnormalities have been described in persons with DS and AD, for example, Lewy bodies as seen in Lewy body dementia. However, this type of dementia is unusual in DS. Membrane-bound granulovacuolar degenerations have been described with the same frequency as in the non-DS population. The endosomal system is known to be abnormal before birth in persons with DS, [182] and recent studies showed that this could be important in the development of AD. [178]
Since the neuropathology typical of AD is observed very early in individuals with DS, the study of this condition in adults with DS could result in knowledge that could also be useful for individuals without DS.
Questions & Answers
Overview
What is the relationship between Alzheimer disease (AD) and Down syndrome (DS)?
What is the pathophysiology of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of genetics in the pathophysiology of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of estrogen in the pathophysiology of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of APOE in the pathophysiology of Alzheimer disease (AD) in Down syndrome (DS)?
What is the prevalence of Alzheimer disease (AD) in Down syndrome (DS)?
What are the racial predilections of Alzheimer disease (AD) in Down syndrome (DS)?
What are the sexual predilections of Alzheimer disease (AD) in Down syndrome (DS)?
What are the signs and symptoms of Alzheimer disease (AD) in Down syndrome (DS)?
What is the association between epileptic seizures and Alzheimer disease (AD) in Down syndrome (DS)?
What are the motor disorders associated with Alzheimer disease (AD) in Down syndrome (DS)?
What is the disease progression of Alzheimer disease (AD) in Down syndrome (DS)?
What are the risk factors for Alzheimer disease (AD) in Down syndrome (DS)?
How is pseudodementia differentiated from early-stage Alzheimer disease (AD) in Down syndrome (DS)?
How common is hypothyroidism in Alzheimer disease (AD) in Down syndrome (DS)?
How common is vitamin B-12 deficiency in Alzheimer disease (AD) in Down syndrome (DS)?
What are the common comorbidities of Alzheimer disease (AD) in Down syndrome (DS)?
Which lab tests are included in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of lumbar puncture in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of neuroimaging in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of biomarkers in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of genetic testing in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of CT scanning in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of MRI in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of PET scanning in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of EEG in the workup of Alzheimer disease (AD) in Down syndrome (DS)?
What is the Alzheimer Functional Assessment Tool?
How does the Alzheimer Functional Assessment Tool measure dining abilities?
How does the Alzheimer Functional Assessment Tool measure bathing ability?
How is the Alzheimer Functional Assessment Tool scored?
How does the Alzheimer Functional Assessment Tool measure toileting abilities?
How does the Alzheimer Functional Assessment Tool measure motor skills and walking ability?
How does the Alzheimer Functional Assessment Tool measure dressing skills?
How does the Alzheimer Functional Assessment Tool measure personal hygiene skills?
How does the Alzheimer Functional Assessment Tool measure environmental awareness?
What is the role of memantine in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of estrogen in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of simvastatin in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of antioxidants in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of NSAIDs in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of selegiline in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
What is the role of surgery in the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
When is inpatient care indicated for the treatment of Alzheimer disease (AD) in Down syndrome (DS)?
How is Alzheimer disease (AD) in Down syndrome (DS) prevented?
How are the complications of Alzheimer disease (AD) in Down syndrome (DS) prevented?
What is included in patient education about Alzheimer disease (AD) in Down syndrome (DS)?
What is the neuropathophysiology of Alzheimer disease (AD) in Down syndrome (DS)?
-
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
-
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
-
CT scan of a man who has Down syndrome confirmed by chromosomal analysis. He has a long history of mental deterioration with progressive loss of ability to perform his usual activities. The CT scan, obtained when the patient was aged 60 years and exhibiting advanced signs of Alzheimer disease, shows several calcified areas in the basal ganglia plus diffuse cortical atrophy and enlargement of the ventricular system. The bilateral symmetric calcifications are a frequent finding in this condition.
-
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
-
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
-
CT scan of a 62-year-old man with Down syndrome confirmed by chromosomal analysis. This CT scan was obtained when he was showing signs of moderate-to-advanced Alzheimer disease. The CT scan shows marked, diffuse enlargement of the ventricular system and generalized atrophy of the cerebral cortex.
Tables

What would you like to print?
- Overview
- Pathophysiology/Risk Factors
- Epidemiology
- Presentation
- Etiology of AD in DS
- Differential Diagnosis and Other Considerations
- Laboratory Studies
- Brain CT Scan
- Brain MRI
- Other Studies
- Dementia Scale and Questionnaire
- Alzheimer Functional Assessment Tool
- Scoring for Alzheimer Functional Assessment Tool
- Treatment of AD in DS
- Patient Education
- Neuropathology
- Questions & Answers
- Show All
- Media Gallery
- References







