Practice Essentials
Chronic pain syndrome (CPS) is a common problem that presents a major challenge to health-care providers because of its complex natural history, unclear etiology, and poor response to therapy. [1] CPS is a poorly defined condition. Most authors consider ongoing pain lasting longer than 6 months as diagnostic, and others have used 3 months as the minimum criterion. In chronic pain, the duration parameter is used arbitrarily. Some authors suggest that any pain that persists longer than the reasonably expected healing time for the involved tissues should be considered chronic pain. [2] (See Presentation and Workup.)
CPS is a constellation of syndromes that usually do not respond to the medical model of care. This condition is managed best with a multidisciplinary approach, requiring good integration and knowledge of multiple organ systems. (The images below demonstrate conditions associated with CPS.) (See Treatment and Medication.)
 Sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with cervical radiculopathy. This image reveals a C6-C7 herniated nucleus pulposus.
Sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with cervical radiculopathy. This image reveals a C6-C7 herniated nucleus pulposus.

 Changes in the hand caused by rheumatoid arthritis. Photograph by David Effron MD, FACEP.
Changes in the hand caused by rheumatoid arthritis. Photograph by David Effron MD, FACEP.
Approximately 35% of Americans have some element of chronic pain, and approximately 50 million Americans are disabled partially or totally due to chronic pain. Chronic pain is reported more commonly in women.
Complications
CPS can affect patients in various ways. Major effects in the patient's life are depressed mood, poor-quality or nonrestorative sleep, fatigue, reduced activity and libido, excessive use of drugs and alcohol, dependent behavior, and disability out of proportion with impairment. (See Presentation.) [3]
Chronic pain may lead to prolonged physical suffering, marital or family problems, loss of employment, and various adverse medical reactions from long-term therapy.
Parental chronic pain increases the risk of internalizing symptoms, including anxiety and depression, in adolescents. [4]
A study by van Tilburg et al indicates that adolescents who have chronic pain and depressive thoughts are at increased risk for suicide ideation and attempt. [5]
Diagnosis and management
The decision to perform any laboratory or imaging evaluations is based on the need to confirm the diagnosis and to rule out other potentially life-threatening illnesses. Sometimes certain investigations are needed to provide appropriate and safe medical or surgical treatment. The recommended treatment should be based on clinical findings or changes in examination findings.
Imaging studies, including with radiography, magnetic resonance imaging (MRI), and computed tomography (CT) scanning, are important tools in the workup of patients with CPS.
Management of chronic pain in patients with multiple problems is complex, usually requiring specific treatment, simultaneous psychological treatment, and physical therapy (PT). [6, 7] PT techniques include hot or cold applications, positioning, stretching exercises, traction, massage, ultrasonographic therapy, transcutaneous electrical nerve stimulation (TENS), and manipulations.
Other treatments include nerve blocks, spinal cord stimulation, and intrathecal morphine pumps.
Etiology
The pathophysiology of chronic pain syndrome (CPS) is multifactorial and complex and still is poorly understood. Some authors have suggested that CPS might be a learned behavioral syndrome that begins with a noxious stimulus that causes pain. This pain behavior then is rewarded externally or internally. Thus, this pain behavior is reinforced, and then it occurs without any noxious stimulus. Internal reinforcers are relief from personal factors associated with many emotions (eg, guilt, fear of work, sex, responsibilities). External reinforcers include such factors as attention from family members and friends, socialization with the physician, medications, compensation, and time off from work.
Patients with several psychological syndromes (eg, major depression, somatization disorder, hypochondriasis, conversion disorder) are prone to developing CPS.
Various neuromuscular, reproductive, gastrointestinal (GI), and urologic disorders may cause or contribute to chronic pain. Sometimes multiple contributing factors may be present in a single patient.
In a study by Alonso-Blanco, a connection was found in women between the number of active myofascial trigger points (MTrPs) and the intensity of spontaneous pain, as well as widespread mechanical hypersensitivity. Nociceptive inputs from these MTrPs may be linked to central sensitization. [8]
A literature review by Gupta et al indicated that in chronic pain patients, primary sensorimotor structural and functional changes are more prominent in females than in males. Males and females differed with regard to the nature and degree of insula changes (with males showing greater insula reactivity), as well as in the extent of anterior cingulate structural changes and in reactivity to emotional arousal. [9]
Musculoskeletal disorders
Musculoskeletal disorders commonly associated with chronic pain include the following:
-
Osteoarthritis/degenerative joint disease/spondylosis (see the image below)
-
Rheumatoid arthritis (see the image below)
 T1-weighted sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with rheumatoid arthritis shows basilar invagination with cranial migration of an eroded odontoid peg. There is minimal pannus. The tip of the peg indents the medulla, and there is narrowing of the foramen magnum, due to the presence of the peg. Inflammatory fusion of several cervical vertebral bodies is shown.
T1-weighted sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with rheumatoid arthritis shows basilar invagination with cranial migration of an eroded odontoid peg. There is minimal pannus. The tip of the peg indents the medulla, and there is narrowing of the foramen magnum, due to the presence of the peg. Inflammatory fusion of several cervical vertebral bodies is shown.
-
Lyme disease
-
Reiter syndrome
-
Disk herniation/facet osteoarthropathy
-
Fractures/compression fracture of lumbar vertebrae
-
Faulty or poor posture
-
Polymyalgia rheumatica
-
Mechanical low back pain
-
Muscular strains and sprains
-
Pelvic floor myalgia (levator ani spasm)
-
Piriformis syndrome (see the image below)
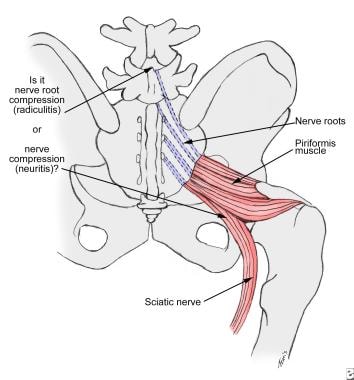 Nerve irritation in the herniated disk occurs at the root (sciatic radiculitis). In piriformis syndrome, the irritation extends to the full thickness of the nerve (sciatic neuritis).
Nerve irritation in the herniated disk occurs at the root (sciatic radiculitis). In piriformis syndrome, the irritation extends to the full thickness of the nerve (sciatic neuritis).
-
Rectus tendon strain
-
Hernias (eg, obturator, sciatic, inguinal, femoral, spigelian, perineal, umbilical)
-
Abdominal wall myofascial pain (trigger points)
-
Chronic overuse syndromes (eg, tendonitis, bursitis)


Neurologic disorders
Neurologic disorders associated with chronic pain include the following:
-
Brachial plexus traction injury
-
Cervical radiculopathy
-
Thoracic outlet syndrome
-
Spinal stenosis (see the image below)
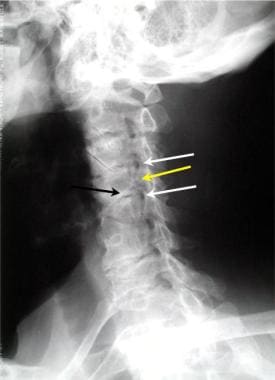 Oblique view of the cervical spine demonstrates 2 levels of foraminal stenosis (white arrows) resulting from facet hypertrophy (yellow arrow) and uncovertebral joint hypertrophy.
Oblique view of the cervical spine demonstrates 2 levels of foraminal stenosis (white arrows) resulting from facet hypertrophy (yellow arrow) and uncovertebral joint hypertrophy.
-
Arachnoiditis
-
Metabolic deficiency myalgias
-
Polymyositis
-
Neoplasia of spinal cord or sacral nerve
-
Cutaneous nerve entrapment in surgical scar
-
Neuralgia (eg, iliohypogastric, ilioinguinal, or genitofemoral nerves)
-
Polyneuropathies
-
Polyradiculoneuropathies
-
Mononeuritis multiplex
-
Chronic daily headaches
-
Muscle tension headaches
-
Migraine headaches
-
Temporomandibular joint dysfunction
-
Temporalis tendonitis
-
Sinusitis
-
Atypical facial pain
-
Trigeminal neuralgia
-
Glossopharyngeal neuralgia
-
Nervus intermedius neuralgia
-
Sphenopalatine neuralgia
-
Referred dental or temporomandibular joint pain
-
Abdominal epilepsy
-
Abdominal migraine
-
Stroke (central poststroke pain) [17]

Urologic disorders
Urologic disorders associated with chronic pain include the following:
-
Bladder neoplasm
-
Chronic urinary tract infection
-
Interstitial cystitis
-
Radiation cystitis
-
Recurrent cystitis
-
Recurrent urethritis
-
Urolithiasis
-
Uninhibited bladder contractions (detrusor-sphincter dyssynergia)
-
Urethral diverticulum
-
Chronic urethral syndrome
-
Urethral carbuncle
-
Prostatitis
-
Urethral stricture
-
Testicular torsion
-
Peyronie disease
Gastrointestinal disorders
GI disorders associated with chronic pain include the following:
-
Chronic visceral pain syndrome
-
Gastroesophageal reflux
-
Peptic ulcer disease
-
Pancreatitis
-
Chronic intermittent bowel obstruction
-
Colitis (see the image below)
 Severe colitis noted during colonoscopy. The mucosa is grossly denuded, with active bleeding noted. This patient had her colon resected very shortly after this view was obtained.
Severe colitis noted during colonoscopy. The mucosa is grossly denuded, with active bleeding noted. This patient had her colon resected very shortly after this view was obtained.
-
Chronic constipation
-
Diverticular disease
-
Inflammatory bowel disease
-
Irritable bowel syndrome

Reproductive disorders (extrauterine)
Extrauterine reproductive disorders associated with chronic pain include the following:
-
Endometriosis (see the image below)
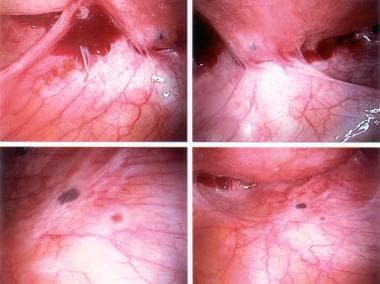 Active endometriosis with red and powder-burn lesions; adhesions from old scarring are present.
Active endometriosis with red and powder-burn lesions; adhesions from old scarring are present.
-
Adhesions
-
Adnexal cysts
-
Chronic ectopic pregnancy
-
Chlamydial endometritis or salpingitis
-
Endosalpingiosis
-
Ovarian retention syndrome (residual ovary syndrome)
-
Ovarian remnant syndrome
-
Ovarian dystrophy or ovulatory pain
-
Pelvic congestion syndrome
-
Postoperative peritoneal cysts
-
Residual accessory ovary
-
Subacute salpingo-oophoritis
-
Tuberculous salpingitis

Reproductive disorders (uterine)
Uterine reproductive disorders associated with chronic pain include the following:
-
Adenomyosis
-
Chronic endometritis
-
Atypical dysmenorrhea or ovulatory pain
-
Cervical stenosis
-
Endometrial or cervical polyps
-
Leiomyomata
-
Symptomatic pelvic relaxation (genital prolapse)
An intrauterine contraceptive device can also be associated with chronic pain.
Psychological disorders
Psychological disorders associated with chronic pain include the following:
-
Bipolar personality disorders
-
Depression
-
Porphyria
-
Sleep disturbances
Other
The following disorders can also be associated with chronic pain:
-
Cardiovascular disease (eg, angina)
-
Peripheral vascular disease
-
Chemotherapeutic, radiation, or surgical complications
Fibromyalgia risk
Results from a study by Mork et al indicated that women who are overweight or obese have a 60-70% greater risk of developing fibromyalgia than do women of normal weight, with body mass index (BMI) being an independent risk factor for the condition. The report looked at whether physical exercise and high BMI influence the occurrence of fibromyalgia. The study included 15,990 women, none of whom at baseline had fibromyalgia or any other physical impairment. By 11-year follow-up, incident fibromyalgia had reportedly occurred in 380 women. The authors noted that only a weak association typically existed between exercise level and fibromyalgia risk.
In overweight or obese women in the study who exercised for at least 1 hour each week, the relative risk (RR) for fibromyalgia (in comparison with women of normal weight and a similar activity level) was 1.72, while in overweight or obese women who did not exercise or who did so for less than an hour per week, the RR was 2.09. [10]
Patient Education
The patient and family should have a good understanding about the multifactorial nature of chronic pain and the benefits of a multidisciplinary comprehensive management plan. [6]
The patient should avoid uncomfortable stressful positions and bad posture. In addition, regular exercise, good sleeping habits, and balanced meals are helpful in maintaining good health. The patient may also benefit from instruction in biofeedback and relaxation techniques.
For excellent patient education information, see the Mental Health Center, as well as Chronic Pain, Fibromyalgia, Chronic Fatigue Syndrome (CFS), and Pain Medications.
-
Sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with cervical radiculopathy. This image reveals a C6-C7 herniated nucleus pulposus.
-
Axial magnetic resonance imaging (MRI) scan of the cervical spine in a patient with cervical radiculopathy. This image reveals a C6-C7 herniated nucleus pulposus.
-
Osteoarthritis of the knee, Kellgren stage III.
-
Nerve irritation in the herniated disk occurs at the root (sciatic radiculitis). In piriformis syndrome, the irritation extends to the full thickness of the nerve (sciatic neuritis).
-
Changes in the hand caused by rheumatoid arthritis. Photograph by David Effron MD, FACEP.
-
Oblique view of the cervical spine demonstrates 2 levels of foraminal stenosis (white arrows) resulting from facet hypertrophy (yellow arrow) and uncovertebral joint hypertrophy.
-
T1-weighted sagittal magnetic resonance imaging (MRI) scan of the cervical spine in a patient with rheumatoid arthritis shows basilar invagination with cranial migration of an eroded odontoid peg. There is minimal pannus. The tip of the peg indents the medulla, and there is narrowing of the foramen magnum, due to the presence of the peg. Inflammatory fusion of several cervical vertebral bodies is shown.
-
Schematic anatomical representations, sympathetic chain and stellate ganglion.
-
Stellate block, important anatomical landmarks (surface and cross-sectional views).
-
Pertinent anatomy for lumbar sympathetic block (cross-sectional view).
-
Severe colitis noted during colonoscopy. The mucosa is grossly denuded, with active bleeding noted. This patient had her colon resected very shortly after this view was obtained.
-
Active endometriosis with red and powder-burn lesions; adhesions from old scarring are present.