Overview
Toxoplasmosis can affect various organ systems, but in HIV-infected patients it most commonly manifests itself as CNS toxoplasmosis, a leading cause of focal central nervous system (CNS) disease in AIDS. CNS toxoplasmosis in HIV-infected patients is usually a complication of the advanced phase of the disease.
Typically, lesions are found in the brain and their effects dominate the clinical presentation. Rarely, intraspinal lesions need to be considered in the differential diagnosis of myelopathy.
The decision to treat a patient for CNS toxoplasmosis is usually empiric. Primary therapy is followed by long-term suppressive therapy, which is continued until antiretroviral therapy can raise CD4+ counts above 200 cells/µL.
Prognosis is guarded. Patients may relapse because of noncompliance or increasing dose requirements.
Pathophysiology
Infection with Toxoplasma gondii, a protozoan parasite, occurs by ingestion of contaminated food sources, such as water, undercooked meat, and cat feces. [1] It usually causes asymptomatic or mild acute disease, and remains dormant in latent phase in healthy immunocompetent hosts. CNS toxoplasmosis is almost always due to reactivation of a latent infection in an immunocompromised host. CNS disease occurs during advanced HIV infection when CD4+ counts are less than 200 cells/µL. The greatest risk is in patients with CD4+ counts less than 50 cells/µL. [2] CNS toxoplasmosis rarely results from primary infection. [3]
Epidemiology
Like other HIV-associated infections, the seroprevalence and prevalence of CNS toxoplasmosis vary depending on geographical area and demographics. [4] There is an increased risk of toxoplasmosis with age, likely due to the increased risk of exposure with increased age.
Clinical CNS toxoplasmosis occurs in 3%–15% of patients with AIDS in the United States, where 789 toxoplasmosis deaths were identified during an 11-year study period from 2000 to 2010. [5]
Some clinically silent lesions come to diagnosis only at autopsy. Clinical CNS toxoplasmosis occurs in as many as 50%–75% of patients in some European countries and in Africa.
The probability of developing reactivated toxoplasmosis is as high as 30% among AIDS patients with a CD4 count < 100 cells/microL who are toxoplasma seropositive and are not receiving effective prophylaxis or antiretroviral therapy. The most common site of reactivation is the central nervous system (CNS). [6]
In an epidemiologic study in Mexico City with 320 patients AIDS patients, the main conditions related to HIV/AIDS were brain toxoplasmosis (42%), cerebral cryptococcosis (28%), tuberculous meningitis (8.7%), lymphoma (non-Hodgkin) (3.75%), acute HIV infection (3.4%), and AIDS dementia complex (3%). [7]
The widespread use of antiretroviral treatment has decreased the incidence of toxoplasmic encephalitis. As an example, among HIV-infected patients in the United States, the annual number of toxoplasmosis-related hospitalizations peaked at more than 10,000 in 1995, dropped sharply to 3643 in 2001, and then decreased to 2985 in 2008. [8]
Clinical Presentation
CNS toxoplasmosis begins with encephalitis and constitutional symptoms and headache. Fever is usually but not always present. Later, confusion and drowsiness, seizures, focal weakness, and language disturbance develop. Without treatment, patients progress to coma in days to weeks.
Extracerebral involvement can also be seen including but not limited to pneumonitis, chorioretinitis, etc.
On physical examination, personality and mental status changes may be observed. Seizures, hemiparesis, hemianopia, aphasia, ataxia, and cranial nerve palsies may be evident. Occasionally, symptoms and signs of a radiculomyelopathy predominate.
Differential Diagnosis
The differential diagnosis of CNS toxoplasmosis includes the following:
-
Mycobacterial infection (eg, tuberculous abscess, tuberculoma)
-
Fungal infection (eg, cryptococcosis, candidiasis)
-
Bacterial abscess (eg, Nocardia)
-
Neurosyphilis
Like CNS toxoplasmosis, progressive multifocal leukoencephalopathy (PML) can cause mental status changes and focal signs. However, headache and seizures are unusual with PML, and PML lesions themselves cause no mass effect.
Serologic Studies
Serologic studies in patients with CNS toxoplasmosis may demonstrate rising titers of anti-toxoplasma immunoglobulin G (IgG) antibodies. An immunoglobulin M (IgM) antibody response is seen in cases of newly acquired toxoplasmosis or Toxoplasma encephalitis for up to a year. [9]
However, anti-Toxoplasmagondii IgG detection may be unreliable in immunodeficient individuals who fail to produce significant titers of specific antibodies. In one study, 16% of patients with a clinical diagnosis and 22% of patients with a histologic diagnosis of toxoplasmosis had undetectable anti-T gondii IgG levels. Causes of false-negative results also include recent infection and insensitive assays.
Definitive Diagnosis
Definitive diagnosis of CNS toxoplasmosis requires the following: [2]
-
Compatible clinical findings
-
Identification of one or more mass lesions by CT, MRI, or other radiographic testing
-
Detection of T gondii in a clinical sample
Detection of T gondii DNA on polymerase chain reaction (PCR) testing of cerebrospinal fluid (CSF) samples may facilitate the diagnosis and follow-up of toxoplasmosis in patients with AIDS. [10] In a study using the B1 gene, rapid PCR showed a sensitivity of 83.3% and specificity of 95.7%. [11]
CSF findings may also include elevated protein and variable glucose and WBC counts. The presence of Epstein-Barr virus DNA in the CSF favors the diagnosis of lymphoma.
Lumbar puncture may be contraindicated because of increased intracranial pressure, however. For many clinicians, therefore, CNS toxoplasmosis is an empiric diagnosis that relies on clinical and radiographic improvement in response to specific anti-T gondii therapy. In patients who fail to respond to specific therapy, brain biopsy can be used to secure a clinical sample for testing. [2]
CT and MRI
A brain CT scan or MRI with and without contrast is indicated for all patients presenting with altered mental status, headaches, seizures, or focal neurologic signs. MRI clearly is the superior technique but is not available universally.
Single or multiple hypodense or hypointense lesions in white matter and basal ganglia with mass effects may be observed on CT or MRI scans. Lesions may enhance in a homogeneous or ring pattern with contrast (see the images below). Imaging studies may be normal in diffuse toxoplasmosis.
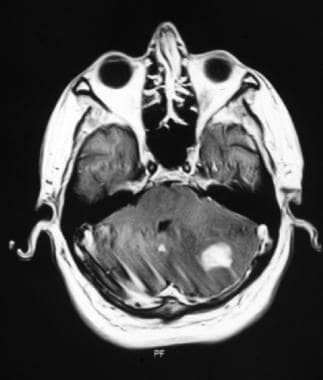 T1-weighted MRI after gadolinium contrast shows a hyperintense lesion in the left cerebellar hemisphere.
T1-weighted MRI after gadolinium contrast shows a hyperintense lesion in the left cerebellar hemisphere.
Single lesions favor the diagnosis of lymphoma over that of toxoplasmosis. However, while multiple lesions are more common than single lesions in toxoplasmosis, in one study 27% of patients had a single lesion on CT scan. In the same study, 14% had a single lesion on MRI. MRI is more sensitive than CT scan in detecting multiple lesions.
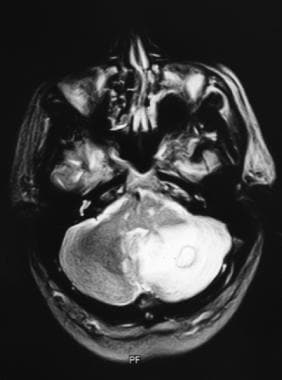
Several MRI patterns have been described in cerebral toxoplasmosis. A concentric target sign is a recently described MRI sign on T2-weighted imaging of cerebral toxoplasmosis; it has concentric alternating zones of hypointensity and hyperintensity. [12]
If the initial imaging study is normal or shows atrophy or focal signal abnormalities (but no mass lesion), diagnostic consideration should be given to meningitides, AIDS dementia complex, or progressive multifocal leukoencephalopathy.
If imaging shows one or more focal mass lesions with impending herniation, an open biopsy with decompression is indicated. Treatment for lymphoma, toxoplasmosis, or other opportunistic infections and neoplasms is initiated, depending on biopsy results.
If imaging shows one or more focal mass lesions without impending herniation, additional studies are warranted.
Scintigraphy
Magnetic resonance spectroscopy (MRS) was not found helpful in differentiating CNS lymphoma from nonmalignant CNS lesions in HIV-infected patients, particularly CNS toxoplasmosis. [13]
Brain Biopsy
Indications for brain biopsy include either of the following:
-
Single mass lesion and negative serologic results
-
No response to 14 days of empiric therapy
Diagnostic yield of stereotactic biopsies increases with the number of specimens obtained.
Histologic findings include the following (also see the images below):
-
Lymphocytic meningitis, individual cyst-containing lesions
-
Astroglial and microglial nodules
-
Associated lymphocytic vasculitis
-
Diffuse encephalitis
 Toxoplasma gondii abscesses are seen on this brain slice. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
Toxoplasma gondii abscesses are seen on this brain slice. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
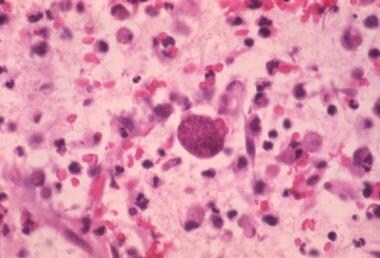 High-magnification photomicrograph shows a tissue cyst and tachyzoites in the brain parenchyma. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
High-magnification photomicrograph shows a tissue cyst and tachyzoites in the brain parenchyma. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.


Treatment and Management
Due to the cystic latent stage of toxoplasmosis and its resistance to medications, eradication of the disease is difficult; [14] however, effective treatments for reactivation exist.
In patients in whom brain imaging shows multiple lesions, whether serologic results are negative or positive, antitoxoplasmosis therapy should be initiated. In cases of impending herniation, an open biopsy with decompression is indicated. Corticosteroid treatment may be warranted in cases of impending brain herniation. However, their use may complicate the interpretation of a response to antitoxoplasmosis therapy.
In a study of 100 patients treated with pyrimethamine-sulfadiazine, the use of adjunctive steroids to treat cerebral edema associated with focal lesions appeared safe but was not associated with better neurologic outcomes. [15]
Empiric antimicrobial therapy must be comprehensive and should cover all likely pathogens in the context of the clinical setting. Antibiotic combinations usually are recommended to circumvent resistance from bacterial subpopulations (which may be resistant to one of the antibiotic components) and to provide additive or synergistic effect.
Standard therapy consists of pyrimethamine, sulfadiazine, and folinic acid in combination. Trimethoprim-sulfamethoxazole (TMP-SMZ) can be used as an alternative regimen. [16] A Cochrane database review found no significant differences between standard therapy and TMP-SMZ. Clindamycin can be used in patients allergic to sulfa drugs. Effective antiretroviral therapy is equally important. [17, 16, 18, 19]
Suggested dosing:
-
Sulfadiazine: 1000 mg 4 times daily among patients < 60 kg or 1500 mg four times a day among patients > 60 kg.
-
Pyrimethamine: 200 mg loading dose followed by 50 mg daily among patients< 60 kg or 75 mg daily among patients > 60 kg.
-
Leucovorin should be administered to prevent pyrimethamine induced hematologic toxicity. Dose can be 10–25 mg daily.
With antibiotic therapy, 74% of patients improve by day 7, and 91% improve by day 14. Imaging studies are performed every 4–6 weeks until complete resolution of the lesion or stabilization after partial resolution.
Primary therapy is given for 6 weeks, followed by long-term suppressive therapy at reduced doses, with the duration determined by response to highly active antiretroviral therapy (HAART). The long-term suppressive therapy can be discontinued in patients with persistent elevation of CD4+ counts greater than 200 cells/µL and resolution of lesions on MRI.
Prevention
To prevent primary toxoplasmosis, patients should avoid eating undercooked meat and should wash their hands carefully after contact with soil or cats. Patients who are seropositive for Toxoplasma should be started on prophylaxis against CNS toxoplasmosis if their CD4+ count drops below 100 cells/μL. [2]
The preferred prophylactic regimen is one double-strength tablet of trimethoprim-sulfamethoxazole (TMP-SMZ) daily, which also provides prophylaxis against Pneumocystis jiroveci pneumonia (PCP). [2] An alternative regimen is one double-strength TMP-SMZ tablet 3 times weekly. The recommended alternative for patients who cannot tolerate TMP-SMZ is dapsone-pyrimethamine plus leucovorin, which is also effective against PCP.
Questions & Answers
Overview
What is CNS toxoplasmosis in HIV infection?
What is the pathophysiology of CNS toxoplasmosis in HIV infection?
What is the prevalence of CNS toxoplasmosis in HIV infection?
Which clinical history findings are characteristic of CNS toxoplasmosis in HIV-infected patients?
Which physical findings are characteristic of CNS toxoplasmosis in HIV-infected patients?
Which conditions are included in the differential diagnoses of CNS toxoplasmosis in HIV infection?
What is the role of serologic studies in the workup of CNS toxoplasmosis in HIV infection?
How is CNS toxoplasmosis in HIV infection diagnosed?
What is the role of imaging studies in the workup of CNS toxoplasmosis in HIV infection?
What is the role of MRS in the workup of CNS toxoplasmosis in HIV infection?
What is the role of brain biopsy in the workup of CNS toxoplasmosis in HIV infection?
Which histologic findings are characteristic of CNS toxoplasmosis in HIV infection?
How is CNS toxoplasmosis prevented in patients with HIV infection?
How is CNS toxoplasmosis treated in patients with HIV infection?
-
T1-weighted MRI after gadolinium contrast shows a hyperintense lesion in the left cerebellar hemisphere.
-
T2-weighted MRI demonstrates intense edema surrounding the lesion.
-
Toxoplasma gondii abscesses are seen on this brain slice. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
-
High-magnification photomicrograph shows a tissue cyst and tachyzoites in the brain parenchyma. Contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.







