Practice Essentials
Spinal cord infarction (SCI) is a serious neurological condition resulting from an interruption of blood flow to the spinal cord, leading to tissue damage and potential neurological deficits.
Signs and symptoms
SCI is usually marked by an acute onset, often heralded by sudden and severe spinal (back) pain, which may radiate caudad. This is associated with bilateral weakness, paresthesias, and sensory loss. Loss of sphincter control with hesitancy and inability to void or defecate becomes evident within a few hours.
The syndrome depends on the level of the cord lesion and may vary from mild or moderate and even reversible leg weakness to quadriplegia.
Diagnosis
A basic knowledge of the signs and symptoms of acute spinal cord dysfunction are required in order to perform a relevant history and physical examination. A spinal sensory level is classically found, but sensory complaints and findings limited to the distal extremities can also be seen early in the course of spinal infarction. Typically onset is apoplectic, evolving in minutes or a few hours to produce severe dysfuction of sensory and motor systems.
Management
The standard drug therapy is aspirin. This is based upon the consensus recommendation for acute treatment of ischemic stroke at any site. Clopidogrel and a combination of aspirin and controlled-release dipyridamole also may be of benefit in reducing the risk of myocardial infarction, recurrent stroke, and death. No direct studies have examined efficacy of drug therapy in SCI.
Background
Occlusive vascular lesions affecting the spinal cord (spinal stroke) are diagnostic challenges. As is the case for the more common cerebrovascular accident affecting cerebral circulation, an acute onset is a clue to the diagnosis. The circulation to the spinal cord has unique features related to the rich anastomotic anatomy of the cord that result in relative rarity of spinal cord infarction in comparison to cerebral infarction, as described in the images below.
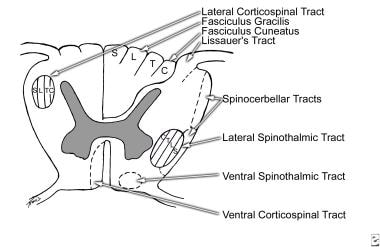 Transverse section of spinal cord showing location of main pathways. The lamination of fibers in posterior columns and in lateral spinothalamic and lateral corticospinal tracts is indicated (C, cervical; T, thoracic; L, lumbar; S, sacral).
Transverse section of spinal cord showing location of main pathways. The lamination of fibers in posterior columns and in lateral spinothalamic and lateral corticospinal tracts is indicated (C, cervical; T, thoracic; L, lumbar; S, sacral).
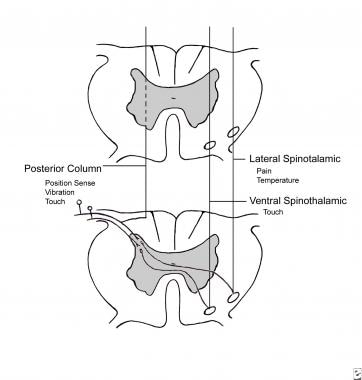 Simplified representation of course of major sensory pathways in the spinal cord. Decussation of the spinothalamic tracts occurs within one or two segments of their entry.
Simplified representation of course of major sensory pathways in the spinal cord. Decussation of the spinothalamic tracts occurs within one or two segments of their entry.
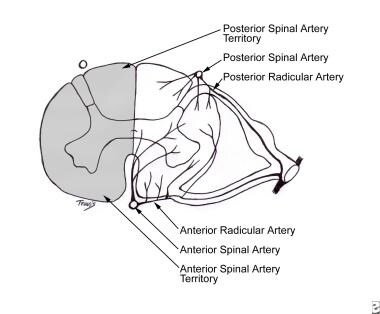 Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
Pathophysiology
The anterior spinal artery is a single long anastomotic channel that lies at the mouth of the anterior central sulcus and supplies the circulation to the anterior two thirds of the spinal cord, shown below.
Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
It gives origin to sulcal arteries that take an arching course to one or the other anterior gray horns. The posterior spinal arteries are smaller paired arteries lying just medial to the dorsal roots. The arterial supply of the spinal cord arises from the aorta and at its cephalad and caudal ends from tributaries of the subclavian and iliac arteries. Eight to ten unpaired anterior medullary arteries are branches of the larger afferent aorta and vertebral and iliac arteries. The largest anterior medullary artery, the great anterior medullary artery of Adamkiewicz, which is susceptible to occlusion with neurologic deficit, is located at the lumbar enlargement, usually at L2 on the left side (but may be at any point from T8 to L2).
Epidemiology
Frequency
Spinal cord infarction is not common, but only fragmentary or indirect data are available on incidence or prevalence. A large study showed that only 9 of 3784 autopsies revealed spinal cord infarction, with a rate of occurrence of 0.23% at death. Conversely, if spinal stroke is approximately 1.2% of strokes, an overall annual incidence of 12 in 100,000 can be estimated.
International incidences are also unclear. Reports that describe patients developing spinal cord infarction in an increasing number of situations and pathologies would influence this because procedures ranging from major surgery to injections for epidural anesthesia, infections and especially meningitis, and medications vary in different countries.
Mortality/morbidity
The risk to life and its quality from spinal cord infarction is substantial because of the disability, which can be severe, with paraplegia, risk of pulmonary emboli, and risk of infection (eg, bladder, lungs, decubiti). However, no epidemiologic studies are available because of the relatively small number of patients affected.
Published series of reports of spinal cord infarction are relatively small, ranging up to 36–44 patients. [1] They find a mortality rate in the vicinity of 20–25% for patients admitted to hospital with spinal cord infarction. [2] No relationship to age is reported. However, the reported series do have a median age of 52 years.
Prognosis
Spinal cord ischemia (and its irreversible tissue injury of infarction) is a myelopathy, generally associated with substantial motor, sensory, and bladder and/or bowel dysfunction. The short-term mortality rate is 20–25% over the first month following onset of symptoms. The overall life expectancy is diminished because of the vascular, infectious, and other medical complications. The striking improvement in medical care and rehabilitation has led to an improvement in quality of life for patients with spinal cord strokes since World War II. A 2012 study of 115 patients with spinal cord infarct found that patients experienced gradual improvement after the event. At 3-year follow-up, 41% of patients using a wheelchair at hospital dismissal were walking and 33% of patients catheterized at dismissal were catheter-free. [21]
Because the extent of damage is less than that sustained in most traumatic cord injuries, and the potential for recovery is greater because ischemia is reversible in part, these patients may have better function than patients with traumatic cord injuries though the prognosis for substantial motor recovery should be guarded.
Patient Education
Those at risk of spinal ischemia cannot be differentiated readily from those at risk of more common disorders of the circulation such as cerebrovascular stroke, myocardial infarction, and renal failure. The measures recommended to reduce these vascular disorders also reduce the incidence and occurrence of myelomalacia. Hence, education of those bearing a treatable vascular risk in regard to diabetic treatment, aspirin prophylaxis, antihypertensive agents, and immunomodulatory therapy logically can be expected to be of benefit and reduce the incidence of spinal thrombosis.
-
Transverse section of spinal cord showing location of main pathways. The lamination of fibers in posterior columns and in lateral spinothalamic and lateral corticospinal tracts is indicated (C, cervical; T, thoracic; L, lumbar; S, sacral).
-
Simplified representation of course of major sensory pathways in the spinal cord. Decussation of the spinothalamic tracts occurs within one or two segments of their entry.
-
Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
-
Guide to clinical determination of the segmental spinal cord level.
-
Transverse section of spinal cord at T12-L1 showing infarction of central cord. The patient became paraplegic following resection of a ruptured abdominal aortic aneurysm. During surgery, prolonged occlusion of the abdominal aorta and great anterior radicular artery was necessary.







