Overview
Absence seizures are a type of generalized non-motor seizures. [1] They were first described by Poupart in 1705, and later by Tissot in 1770, who used the term petit access. In 1824, Calmeil used the term absence. [2] In 1935, Gibbs, Davis, and Lennox described the association of impaired consciousness and 3-Hz spike-and-slow-wave complexes on electroencephalograms (EEGs). [3]
Absence seizures occur in idiopathic and symptomatic generalized epilepsies. [4] Among the idiopathic generalized epilepsies, absence seizures are seen in childhood absence epilepsy (pyknolepsy), juvenile absence epilepsy, and juvenile myoclonic epilepsy (impulsive petit mal). [5] The seizures in these conditions are called typical absence seizures and are usually associated with generalized 3-4 Hz spike-and-slow-wave complexes on EEG. [6]
In childhood absence epilepsy, seizures are frequent and brief, lasting just a few seconds (pyknoleptic). Some children can have many such seizures per day. In other epilepsies, particularly those with an older age of onset, the seizures can last several seconds to minutes and may occur only a few times a day; these are called nonpyknoleptic or spanioleptic absence seizures.
Myoclonic and tonic-clonic seizures may also be present, especially in syndromes with an older age of onset.
In the cryptogenic or symptomatic generalized epilepsies, absence seizures are often associated with slow spike-wave complexes of 1.5-2.5 Hz [5] ; these are also called sharp-and-slow-wave complexes. These seizures may be associated with loss of axial tone and head nodding; a fall may occur. Increased tone, autonomic features, and automatisms may also be seen. Absence seizures associated with slow spike-wave complexes are called atypical absence seizures. [7]
See Epilepsy and Seizures for a general overview of these topics.
Classification
The International League Against Epilepsy (ILAE) Commission on Classification and Terminology revised the concepts, terminology, and approaches for classifying seizures and epilepsy. [8]
The classification of absence seizures has been simplified as follows:
-
Typical absence
-
Atypical absence
-
Myoclonic absence
-
Eyelid myoclonia
Patient education
Patients who are old enough to drive should be warned about driving and operating heavy machinery. Physicians should be familiar with state laws concerning driving with epilepsy; inform patients concerning these legal matters.
For patient education information, see the Brain and Nervous System Center, as well as Epilepsy.
Etiology
The etiology of idiopathic epilepsies with age-related onset is genetic. About 15-40% of patients with these epilepsies have a family history of epilepsy; overall concordance in monozygotic twins is 74%, with a 100% concordance during the peak age of phenotypic expression. [9] Family members may have other forms of idiopathic or genetic epilepsy (eg, febrile convulsions, generalized tonic-clonic seizures).
The idiopathic generalized epilepsies are a group of primary generalized epilepsies with absence, myoclonic, and tonic-clonic seizures. Based on age of onset and seizure types, some can be grouped into well-recognized syndromes, such as childhood absence epilepsy, juvenile absence epilepsy, and juvenile myoclonic epilepsy.
However, patients with other syndromes, such as generalized epilepsy with febrile seizures plus (GEFS+), as well as patients who have childhood absence epilepsy that leads into juvenile myoclonic epilepsy, illustrate that these syndromes represent a genetically determined lower threshold to have seizures.
The idiopathic generalized epilepsies are best viewed as a spectrum of clinical syndromes [10] with varied genetic causes that affect the function of ion channels.
Genetic studies have shown that these syndromes are channelopathies, but different gene mutations have been found in the same syndromes. Juvenile myoclonic epilepsy has been linked to chromosome 6, [11, 12] with linkage to chromosome 6p12 in Mexican families. [13] Mutations in the EFHC1 gene have been found in Mexican [14, 15] and Italian families [16] with juvenile myoclonic epilepsy, but not in a group of Dutch families. [17]
Childhood absence epilepsy with generalized tonic-clonic seizure has been linked to chromosome 8q24 in a 5-generation family from Bombay, India. [18] Childhood absence epilepsy with febrile seizures has been linked to the GABA(A) receptor γ2 subunit (GABRG2) on chromosome 5q3.1-33.1. [19]
A mutation in the GABA(A) receptor gene GABRB3 was found in Mexican families with childhood absence epilepsy. Mutations showed hyperglycosylation in vitro, with reduced GABA-evoked current density from whole cells. Expression of this gene in the developing brain may help explain an age-related onset and remission in childhood absence epilepsy. [20]
Pathophysiology
The pathophysiology of absence seizures is not fully understood. In 1947, Jasper and Droogleever-Fortuyn electrically stimulated nuclei in the thalami of cats at 3 Hz and produced bilaterally synchronous spike-and-wave discharges on EEG. [21] In 1953, bilaterally synchronous spike-and-wave discharges were recorded by placing depth electrodes in the thalamus of a child with absence seizures. [22]
In 1977, Gloor et al demonstrated that the bilaterally synchronous, 3-Hz spike-wave discharges in the feline penicillin model of absence seizures were generated in the cortex. This led to the corticoreticular theory of primarily generalized seizures.
Abnormal oscillatory rhythms are believed to develop in thalamocortical pathways. This involves gamma-aminobutyric acid (GABA)-B–mediated inhibition alternating with glutamate-mediated excitation.
The cellular mechanism is believed to involve T-type calcium currents. T channels of the GABAergic reticular thalamic nucleus neurons appear to play a major role in the spike-wave discharges of the GABAergic thalamic neurons. [23]
GABA-B inhibition appears to be altered in absence seizures, and potentiation of GABA-B inhibition with tiagabine (Gabitril), vigabatrin (Sabril), [24] and, possibly, gabapentin (Neurontin), results in exacerbation of absence seizures. Enhanced burst firing in selected corticothalamic networks may increase GABA-B receptor activation in the thalamus, leading to generalized spike-wave activity.
These data suggest that activity of thalamic networks is necessary for spike-wave discharge rhythmogenesis, and cortical hyperexcitability is necessary for their generation. [25]
In symptomatic generalized epilepsies, absence seizures are due to a wide variety of causes that at an early stage of neural development, result in diffuse or multifocal brain damage. The causes and management of secondary generalized epilepsies, and the other seizure types that accompany them, are not discussed in this article.
Risk factors
After noncompliance with treatment, lack of sleep is the most frequent cause of seizure exacerbations. Drugs that lower the seizure threshold (eg, alcohol, cocaine, high-dose penicillin, isoniazid [INH] overdose, neuroleptics) are most likely to cause seizures in patients with epilepsy. Withdrawal of alcohol, benzodiazepines, and other sedatives are also common causes.
Epidemiology
Incidence in the United States
The incidence of absence seizures in the United States is 1.9-8 cases per 100,000 population.
Morbidity and mortality
The morbidity from typical absence seizures is related to the frequency and duration of the seizures, as well as to the patient's activities; effective treatment ameliorates these factors.
Educational and behavioral problems are sequelae of frequent, unrecognized seizures.
No deaths result directly from absence seizures. However, if an individual suffers an absence seizure while driving or operating dangerous machinery, a fatal accident may occur.
In children with absence seizures due to secondary generalized epilepsies, death is related to the underlying disease.
Sex predilection
Absence seizures are generally believed to be more common in females than in males. Up to two thirds of children with childhood absence epilepsy are girls. [9, 26]
Absence epilepsy with myoclonus has a male predominance. [27]
Age of onset
The generalized idiopathic epilepsies have age-related onset.
Onset of absence seizures in children with symptomatic generalized epilepsies depends on the underlying disorder. While many of these disorders may have their onset at an early (prenatal, perinatal, or postnatal) age, absence seizures do not appear until later in childhood. An example is the Lennox-Gastaut syndrome. The cause may be a genetic disorder or a perinatal insult, but the absence seizures do not present until age 1-8 years. [28]
Childhood absence epilepsy onset is at age 4-8 years, with peak onset at age 6-7 years. [26]
Juvenile absence epilepsy onset is generally around puberty. Actual age of onset may vary, depending on whether pyknoleptic (8.3 ± 4.5 y) or nonpyknoleptic seizures occur (14.8 ± 8.3 y). [29]
Juvenile myoclonic epilepsy has a more varied age of onset (8-26 y), but 79% of patients have an onset between the ages of 12 and 18 years. [30] Because the absence and myoclonic seizures are brief, they often go unrecognized, and many patients do not present until they experience a tonic-clonic seizure.
Clinical Presentation
Patient history
Children with idiopathic generalized epilepsies may present with a history of staring spells, but infrequent absence seizures may not be diagnosed until a generalized tonic-clonic seizure has occurred.
Other symptoms, such as behavioral problems, may be the presenting complaint. [31] Whether this is a comorbid condition or a result of brief, unrecognized attacks that cause lapses of awareness and interferes with attention is unknown.
Decline in school performance may be an indication of the onset or breakthrough of absence seizures.
In symptomatic generalized epilepsies, atypical absence seizures often occur in the setting of developmental delay or intellectual disability. (See Table 1, below, for features of typical and atypical absence seizures.)
Other seizure types can be present in the patient, such as myoclonic, tonic, atonic, tonic-clonic, and even partial seizures.
Physical examination
Physical and neurologic findings are normal in children with idiopathic generalized epilepsies. Having the child hyperventilate for 3-5 minutes can often provoke absence seizures. This procedure can easily be performed in the clinic or office, and the result is diagnostic.
On clinical examination, typical absence seizures appear as brief staring spells. Patients have no warning or postictal phase, and if engaged in gross motor activity, such as walking, they may stop and stand motionless or they may continue to walk. Children are not responsive during the seizure and have no memory of what happened during the attack; they are generally unaware that a seizure has occurred. (See Table 1, below.)
Atypical absence seizures, which occur in patients with symptomatic generalized epilepsies, are usually longer than typical absences and often have more gradual onset and resolution.
In symptomatic generalized epilepsies, physical and neurologic findings may be abnormal, reflecting the underlying disorder. Physical examination may reveal stigmata of a genetic disease, such as a neurocutaneous disorder (eg, tuberous sclerosis) or an inborn error of metabolism. Neurologic examination may show signs of developmental delay or more specific signs, such as spastic paresis in cerebral palsy.
Table 1. Clinical and EEG Findings in Typical and Atypical Absence Seizures* (Open Table in a new window)
Type of Clinical Seizure |
EEG Findings |
||
Typical absence |
Impairment of consciousness only |
Usually regular and symmetrical 3 Hz, possible 2- to 4-Hz spike-and-slow-wave complexes, and possible multiple spike-and-slow-wave complexes |
|
Mild clonic components |
|||
Atonic components |
|||
Tonic component |
|||
Automatisms |
|||
Autonomic components |
|||
Atypical absence |
Changes in tone more pronounced than those of typical absence seizure |
EEG more heterogeneous than in typical absence; may include irregular spike-and-slow-wave complexes, fast activity, or other paroxysmal activity; abnormalities bilateral but often irregular and asymmetrical |
|
Nonabrupt onset or cessation abrupt |
|||
*May be seen alone or in combination. Adapted from Dreifuss FE. Classification of epileptic seizures. In: Engel J Jr, Pedley TA, eds. Epilepsy: A Comprehensive Textbook. Philadelphia, PA: Lippincott-Raven;1997. |
|||
Differential Diagnosis
Attention Deficit Hyperactivity Disorder (ADHD)
Confusional States and Acute Memory Disorders
Psychogenic Nonepileptic Seizures
Breath-holding spells are another differential.
Staring spells, daydreaming, migraine equivalents, and panic and/or anxiety attacks all may be confused with nonconvulsive seizures.
Absence versus complex partial seizures
Absence seizures may be confused with complex partial seizures, especially in cases of prolonged seizures with automatisms (see Table 2, below).
Table 2. Differentiating Features of Complex Partial and Absence Seizures (Open Table in a new window)
Feature |
Complex Partial |
Absence |
Onset |
May have simple partial onset |
Abrupt |
Duration |
Usually >30 s |
Usually < 30 s |
Automatisms |
Present |
Duration dependent |
Awareness |
No |
No |
Ending |
Gradual postictal |
Abrupt |
The occurrence of automatisms is dependent on duration of the seizure; the longer the seizure, the more likely automatisms are to occur (see image below). [32]
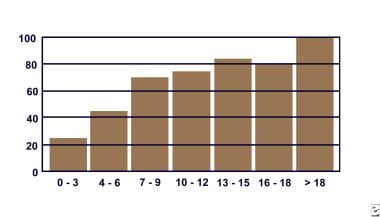 Percentage of absence seizures with automatisms as a function of duration in seconds. (Data gathered from Penry et al, 1975.)
Percentage of absence seizures with automatisms as a function of duration in seconds. (Data gathered from Penry et al, 1975.)
Laboratory Studies
When evaluating a child for staring spells, laboratory tests for metabolic abnormalities or toxic or drug ingestion (especially in older children) may be indicated. If a clear history of the episodic nature of the attacks is obtained, then the EEG can be diagnostic and laboratory tests may not be necessary.
When evaluating a child with a developmental delay, or if the EEG reveals atypical absences, then a full work-up for the underlying cause of a symptomatic generalized epilepsy is indicated.
Neuroimaging Studies
Neuroimaging findings are normal in idiopathic epilepsies by definition, and therefore, neuroimaging is not indicated if the typical clinical pattern is present.
However, neuroimaging is often ordered by primary care providers and the emergency department, especially if a child presents with a generalized tonic-clonic seizure, to rule out significant structural causes of seizures. A normal result helps to support the diagnosis of idiopathic epilepsy. For cryptogenic and symptomatic generalized epilepsies, neuroimaging can help in the diagnosis of any underlying structural abnormality.
If imaging is performed, magnetic resonance imaging (MRI) is preferred to computed tomography (CT) scanning. MRI is more sensitive for certain anatomic abnormalities.
A review of 134 MRI scans in patients with idiopathic generalized epilepsies found nonspecific abnormalities in 24%. [33]
Electroencephalography
The only diagnostic test for absence seizures is the EEG.
Background activity is normal. In syndromes with frequent absence seizures, such as childhood absence epilepsy, a routine awake recording is often pathognomonic. Bursts of frontally predominant, generalized 3-Hz spike-and-wave complexes are seen during the seizures. [3] In syndromes with less frequent absence seizures (juvenile absence epilepsy or juvenile myoclonic epilepsy), an awake recording may be normal; a sleep or sleep-deprived recording may be needed.
Typical absence seizures have generalized 3-Hz spike-and-wave complexes (see image below).
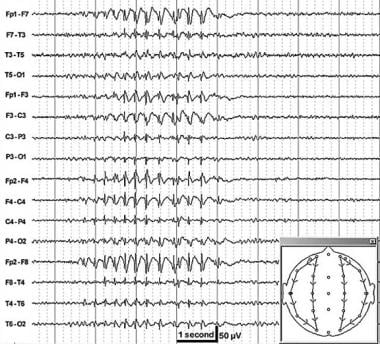
The spike frequency is often faster at the onset, with a slight deceleration at the end. [26] They can range from 2.5-6 Hz, with the faster frequencies seen in syndromes with older age of onset.
Bursts of generalized polyspikes and waves (multiple spike-and-slow-wave complexes) may also be seen, [30] especially during sleep and in syndromes with older age of onset.
The onset and ending of these seizures are abrupt; no postictal EEG slowing is noted.
Hyperventilation often provokes these seizures and should be a routine part of all EEGs in children.
Photosensitivity may be present in idiopathic generalized epilepsies and is more often seen in juvenile myoclonic epilepsy and childhood absence epilepsy than juvenile absence epilepsy. [29]
EEG video monitoring demonstrates that clinical seizure manifestations may lag behind the start of ictal EEG activity; bursts lasting less than 3 seconds are usually clinically silent. During the absence seizure, rhythmic eye blinks and mild clonic jerks may be present. As a seizure progresses, automatisms may be seen. [32]
Clinical and EEG features may vary considerably in different children. [34]
Go to EEG Video Monitoring for procedural information on this topic.
EEG findings in atypical absence seizures
Atypical absence seizures are characterized by slow spike-and-wave paroxysms, classically 2.5 Hz (see the image below). The onset may be difficult to discern, and postictal EEG slowing may be noted.
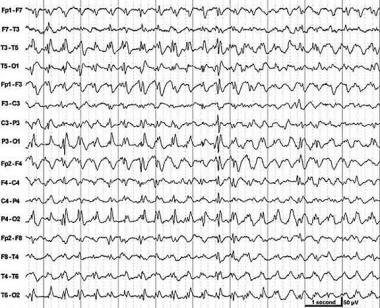 Slow spike-and-wave discharges (2.5 Hz). This is an interictal pattern in a child with seizures and developmental delay.
Slow spike-and-wave discharges (2.5 Hz). This is an interictal pattern in a child with seizures and developmental delay.
Background activity is often abnormal, reflecting the diffuse or multifocal underlying encephalopathy of symptomatic generalized epilepsy.
Generalized polyspike-and-wave complexes also may be present, and focal features may be observed.
The clinical correlation of generalized spike-and-wave complexes with clinical seizures is not as clear-cut as in typical absence seizures. Generalized slow spikes and waves may be present as an interictal pattern, as in Lennox-Gastaut syndrome.
EEG video monitoring can show a more varied alteration of consciousness than in typical absence seizures. If the patient has underlying intellectual disability, discerning changes in mental status may be more difficult in atypical absence.
Changes in postural tone, most noticeably head nods, are common.
Ambulatory EEG monitoring over 24 hours may be useful to quantitate the number of seizures per day and their most likely times of occurrence.
Pharmacologic Treatment
Treatment for absence seizures involves antiepileptic drugs (AEDs). Once the proper diagnosis (ie, of the specific epilepsy syndrome) is made, the likelihood of other, coexistent seizure types in the patient, such as myoclonic or tonic-clonic seizures, should be considered and an appropriate medication selected. Since altered awareness occurs with even brief bursts of spike-wave paroxysms on EEG, treatment should be titrated to suppressing all epileptiform activity.
The decision to start antiepileptic medication must be made with great care. Most AEDs are relatively toxic and can have sedative and cognitive side effects. Children with absence seizures may need to be on medication for many years, and in some cases, for life. EEG can usually confirm the diagnosis, and the presence of spontaneous seizures can be documented on routine EEG or with longer recordings (ie, 24-hour ambulatory EEG or EEG video monitoring).
Only 2 first-line AEDs have approval from the US Food and Drug Administration (FDA) to be indicated for absence seizures: ethosuximide (Zarontin) and valproic acid (Depakene, Depacon). Ethosuximide has efficacy for absence seizures only and valproic acid has efficacy for absence, generalized tonic-clonic, and myoclonic seizures.
Ethosuximide (Zarontin) is effective only against absence seizures.
Valproic acid (Depakene, Depacon, Depakote, Depakote ER) is considered a broad-spectrum AED, because it is effective against absence, myoclonic, tonic-clonic, and partial seizures.
A study showed that ethosuximide and valproic acid were more effective than lamotrigine in the treatment of childhood absence epilepsy, and that ethosuximide had fewer adverse attentional side effects. [35]
Symptomatic generalized epilepsies are often refractory to first-line AEDs. Lamotrigine (Lamictal), topiramate (Topamax), and felbamate (Felbatol) are approved by the FDA as adjunctive therapy for the generalized seizures of Lennox-Gastaut syndrome in adult and pediatric patients (>2 y). Clonazepam (Klonopin) and the ketogenic or medium-chain triglyceride diet have been attempted to reduce seizure frequency. However, these adjunctive therapies have limited efficacy.
Of the newer AEDs, lamotrigine, topiramate, and levetiracetam have been shown to have efficacy against seizures in idiopathic generalized epilepsy [36, 37] and have received FDA approval to be indicated for adjunctive therapy of generalized tonic-clonic seizures in idiopathic generalized epilepsy in children aged 2 years and older (for lamotrigine and topiramate) and in children aged 6 years and older (for levetiracetam). Levetiracetam is indicated as adjunct therapy for generalized tonic-clonic and myoclonic seizures. It has been shown to have only modest efficacy against absence seizures. [38, 39]
Lamotrigine and topiramate are also approved as adjunctive therapy in Lennox-Gastaut syndrome in children aged 2 years and older. Rufinamide (Banzel) has been shown effective against typical and atypical absence seizures as well as other seizures in Lennox-Gastaut syndrome [40] and is approved as adjunct therapy in children older than 4 years.
Topiramate has also received FDA approval as initial monotherapy for generalized tonic-clonic seizures in children aged 10 years and older with idiopathic generalized epilepsy. Studies have shown these medications to have antiabsence efficacy, but the data are incomplete. [41]
Some AEDs can aggravate seizures, especially in cryptogenic or symptomatic generalized epilepsies. [42] Treatment with carbamazepine (Tegretol, Tegretol XR, Carbatrol) [43, 44] and oxcarbazepine (Trileptal) [45] has been associated with the exacerbation of absence seizures. Gabapentin (Neurontin) is ineffective against absence seizures, [46] and tiagabine (Gabitril) and vigabatrin (Sabril) have been associated with the exacerbation of absence or myoclonic seizures in some patients. [47]
Conception and pregnancy considerations
Women of childbearing age who are not using adequate birth control should not be treated with valproic acid, if equally effective alternatives are available for them.
If a woman taking valproic acid wishes to become pregnant, treatment may be crossed over to ethosuximide if only absence seizures are present, and she may be given folic acid 1-5 mg/d before conception. After the first trimester, treatment may be switched back to valproic acid.
Women with generalized tonic-clonic seizures may be crossed over to lamotrigine, and given folic acid 1-5 mg/d before conception.
Most clinicians believe that women treated with valproic acid or any hepatic enzyme-inducing AED should be treated with vitamin K before delivery.
Consultations
All patients with suspected absence seizures should be examined by a neurologist who has expertise in diagnosing epileptic syndromes. Patients with refractory seizures, especially those with symptomatic epilepsies, may need to be referred to an epileptologist for prolonged EEG video monitoring and medication adjustments.
Diet
A ketogenic [48] or medium-chain triglyceride diet [49] may be tried in patients with medically intractable seizures. Although these diets are difficult to maintain, there is evidence for their effectiveness. [50] Children in whom such diets are being considered should be referred to a center with specialized dietary services.
Activity
Physical activity should not be restricted any more than necessary. Activities in which a seizure might pose a threat, such as swimming or rock climbing, may be allowed with appropriate supervision. A child with epilepsy should not be unnecessarily handicapped. Patients with uncontrolled absence seizures should not be allowed to drive. The situation may be unclear when the patient's clinical seizures are controlled but the EEG still shows some spike-wave activity.
Outpatient Management
Children with absence seizures should be monitored closely during titration or crossover of AEDs. The dose of the medication should be increased weekly until seizures are controlled or adverse effects develop.
The aim in therapy is to control seizures completely with the minimum required amount of medication to minimize adverse effects.
The therapeutic effect of valproic acid for absence seizures may lag several weeks behind reaching a therapeutic level. [51]
Liver function test, amylase and/or lipase, and complete blood cell (CBC) count results should be monitored during drug treatment to watch for adverse reactions.
Drug levels should be monitored to ensure treatment compliance and to watch for toxic levels in patients who are too young or too developmentally disabled to articulate subjective adverse effects.
Prognosis
The prognosis for the primary generalized epilepsies depends on the particular epileptic syndrome. Because seizures, particularly generalized tonic-clonic seizures, may occur well after patients appear to achieve good control, a long seizure-free period should be achieved before discontinuation of therapy is considered.
The remission rate for childhood absence epilepsy is good; 80% of patients respond to medication. Complete remission rates vary widely, perhaps dependent on the length of follow-up.
Generalized tonic-clonic seizures may develop in up to 40% of children with childhood absence epilepsy. [26] Persistence of seizures is more likely in those with generalized tonic-clonic seizures.
Early onset of absence seizures, quick response to therapy, [52] and normal EEG background are good prognostic signs.
Juvenile myoclonic epilepsy carries a high risk of generalized tonic-clonic seizures. Despite excellent control with relatively small doses of an AED, the relapse rate is greater than 90%. [53]
Patients with juvenile myoclonic epilepsy generally need to be treated for life, although occasional patients achieve control with careful attention to lifestyle issues (eg, adequate sleep, abstinence from alcohol).
Questions & Answers
Overview
How are absence seizures classified?
What is included in patient education about absence seizures?
What is the pathophysiology of absence seizures?
What are the risk factors for absence seizures?
What is the incidence of absence seizures in the US?
What is the morbidity associated with absence seizures?
What are the sexual predilections of absence seizures?
Which age groups have the highest prevalence of absence seizures?
Which clinical history findings are characteristic of absence seizures?
Which physical findings are characteristic of absence seizures?
Which conditions should be included in the differential diagnosis of absence seizures?
How are absence seizures differentiated from complex partial seizures?
What is the role of lab testing in the workup of absence seizures?
What is the role of neuroimaging studies in the diagnosis of absence seizures?
What is the role of EEG in the diagnosis of absence seizures?
How are absence seizures treated?
What is the role of antiepileptic drugs (AEDs) in the treatment of absence seizures?
How are absence seizures treated during pregnancy?
Which specialist consultations are beneficial to patients with absence seizures?
Which dietary modifications are used in the treatment of absence seizures?
Which activity modifications are used in the treatment of absence seizures?
What is included in the long-term monitoring of patients with absence seizures?
What is the prognosis of absence seizures?
-
Percentage of absence seizures with automatisms as a function of duration in seconds. (Data gathered from Penry et al, 1975.)
-
EEG of a typical absence seizure with 3-Hz spike-and-wave discharges.
-
Slow spike-and-wave discharges (2.5 Hz). This is an interictal pattern in a child with seizures and developmental delay.
Tables
Type of Clinical Seizure |
EEG Findings |
||
Typical absence |
Impairment of consciousness only |
Usually regular and symmetrical 3 Hz, possible 2- to 4-Hz spike-and-slow-wave complexes, and possible multiple spike-and-slow-wave complexes |
|
Mild clonic components |
|||
Atonic components |
|||
Tonic component |
|||
Automatisms |
|||
Autonomic components |
|||
Atypical absence |
Changes in tone more pronounced than those of typical absence seizure |
EEG more heterogeneous than in typical absence; may include irregular spike-and-slow-wave complexes, fast activity, or other paroxysmal activity; abnormalities bilateral but often irregular and asymmetrical |
|
Nonabrupt onset or cessation abrupt |
|||
*May be seen alone or in combination. Adapted from Dreifuss FE. Classification of epileptic seizures. In: Engel J Jr, Pedley TA, eds. Epilepsy: A Comprehensive Textbook. Philadelphia, PA: Lippincott-Raven;1997. |
|||
Feature |
Complex Partial |
Absence |
Onset |
May have simple partial onset |
Abrupt |
Duration |
Usually >30 s |
Usually < 30 s |
Automatisms |
Present |
Duration dependent |
Awareness |
No |
No |
Ending |
Gradual postictal |
Abrupt |






