Background
Child abuse is often misdiagnosed and under recognized by physicians and caregivers. Child abuse occurs in many forms and is best defined as purposeful infliction of physical or emotional harm, sexual exploitation, and/or neglect of basic needs (eg, nutrition, education, medical care). Child abuse is an important cause of death in children. Among child abuse fatalities, head injury is the leading cause of death in infancy.
Shaken baby syndrome (SBS) is of particular interest to the neurologist, as it affects the nervous system. Shaken baby syndrome may cause long-term sequelae in the developing nervous system, and the effects may even be lethal. See the image below.
In 1946, Caffey reported a series of patients with multiple fractures and chronic subdural hematoma, which fit the profile of what is now defined as shaken baby syndrome. [1] Kempe et al coined the term battered child syndrome. [2] In 1967, Gilkes and Mann first reported the funduscopic findings of battered babies. [3] In 1972, Caffey wrote about the syndrome of shaken infants. His report brought attention to this form of child abuse. [4]
The term "shaken baby syndrome" has been commonly used to describe symptoms consistent with shaking an infant, which produces bilateral retinal hemorrahge and diffuse brain injury. However, the term shaken impact syndrome is used for injuries that exceed those just from shaking and have evidence of blunt head trauma. The American Academy of Pediatrics in 2009 recommended the use of the term "abusive head trauma," rather than shaken baby syndrome or non-accidental injury. [5] This term describes the type of injury rather than the mechanism of injury.
Abusive head trauma (AHT) is a well-recognized brain injury associated with the direct application of force to an infant that results in physical injury to the brain and/or its contents. [6]
Pathophysiology
Anatomic features make infants especially prone to neurologic injury from excessive shaking or trauma. Infants have a large head compared with their body size, and the cervical paraspinal muscles are weak. (This accounts for head lag observed during the first month of life.) The infant brain has a higher water content than that of the adult brain, and it is incompletely myelinated. The subarachnoid spaces are also larger in infants than in adults, given the small size of their brains.
When the infant is shaken, movement of the immature brain in relation to the skull and the poor muscle tone in the neck cause the bridging vessels to tear, resulting in the classic finding of a subdural hematoma. Retinal hemorrhages are produced when venous congestion causes rupture of the retinal vasculature. Therefore, shaken baby syndrome is defined by subdural hemorrhage and retinal hemorrhage. One additional feature is occult fractures, particularly of ribs and long bone metaphyses.
The mechanism by which brain damage occurs is controversial. Traditionally, shearing forces from direct trauma were believed to cause axonal damage. Geddes et al suggested hypoxia-ischemia as the mechanism rather than axonal injury that is seen in older children and adults with lethal head trauma. [7, 8] They also thought that acceleration and deceleration forces may damage the neuraxis to cause apnea, with consequent ischemia and cerebral edema.
Biomechanical studies of infant trauma injuries have shown that the magnitude of angular deceleration is 50 times greater when the infant's head strikes a surface than when he or she is only shaken. This force is distinct from those of other accidental traumas that occur in infants. This evidence suggests that the term shaking-impact syndrome is more accurate than shaken baby syndrome.
Epidemiology
Frequency
In 2021, an estimated 1820 children died from abuse and neglect in the United States. In the same year, 51 states reported 588,229 victims of child abuse and neglect; 76.0% of victims are neglected, 16.0% are physically abused, 10.1% are sexually abused, and 0.2% are sex trafficked. The youngest children were most vulnerable to maltreatment. Children younger than 1 year old have the highest rate of victimization at 25.3 per 1000 children of the same age in the national population. The victimization rate for girls is 8.7 per 1000 girls in the population, which is higher than boys at 7.5 per 1000 boys in the population. [9, 10]
Mortality/morbidity
Abuse and neglect account for 5–14% of all deaths of children. The youngest children were most vulnerable to maltreatment. Children in the first year of their life had the highest rate of victimization 25.3 per 1000 children nationwide. [9, 10]
In Missouri, 30 out of 35 children who died from inflicted abuse or neglect at the hands of a parent or caregiver were four years of age or younger. Of those, 13 were infants younger than one year. [11] In Illinois in 2016, incidence of child abuse–related deaths was 216 per 100,000 children.{ref42-INVALID REFERENCE}
Sex
Boys are affected more often than girls.
The perpetrator is usually alone with the victim. Men are the abusers in 90% of cases. The abuser is usually the biologic father or, in some cases, the mother's boyfriend. The most common female attacker is a babysitter.
According to a Philadelphia-based study, 1 in 7 mothers who were abused as children admitted to using corporal punishment on their children. [12]
Age
More than 600,000 children are abused in the United States each year. Children in the first year of their life account for 15% of all victims, and 28% of child maltreatment victims are no more than 2 years old. The typical abused child is younger than 6 months. [10]
Prognosis
The prognosis depends on the severity of the neurologic injury and the involvement of other organ systems.
-
CT scan shows a subdural hematoma.
-
CT scan shows cerebral edema with loss of gray matter–white matter distinction.
-
T1-weighted MRIs reveal bilateral chronic subdural hematomas as well as severe encephalomalacia involving the parietal, occipital, and temporal lobes.
-
T1-weighted MRIs show chronic bilateral subdural hematomas.
-
T2-weighted MRIs show encephalomalacia after shaken baby syndrome.
-
Sagittal MRIs show chronic subdural hematoma.
-
Funduscopic image shows intraretinal hemorrhages, subhyaloid hemorrhages, localized hemorrhagic choroid detachments, and thin retinal folds.
-
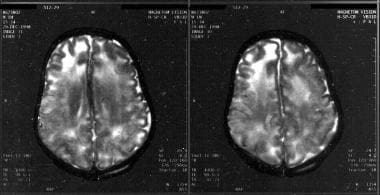
Flair and T2 images reveal intrahemispheric bleeding.









