Practice Essentials
Amyotrophic lateral sclerosis (ALS) is the most common degenerative disease of the motor neuron system. Although ALS is incurable and fatal, with median survival of 3 years, treatment can extend the length and meaningful quality of life for patients.
Signs and symptoms
In 75–80% of patients, symptoms begin with limb involvement. Initial complaints in patients with lower limb onset are often as follows:
-
Tripping, stumbling, or awkwardness when running
-
Loss of lower extremity muscle bulk, strength, or endurance
-
Foot drop; patients may report a "slapping" gait
Initial complaints with upper limb onset include the following:
-
Reduced finger dexterity, cramping, stiffness, and weakness or wasting of intrinsic hand muscles
-
Wrist drop interfering with work performance
With bulbar onset (20–25% of patients), initial complaints are as follows:
-
Slurred speech, hoarseness, or decreased volume of speech
-
Aspiration or choking during a meal
Emotional difficulties in some ALS patients are as follows:
-
Involuntary laughing or crying
-
Depression
-
Impaired executive function and other cognitive changes
-
Behavioral changes
Some patients will show cognitive and behavioral changes due to involvement of the prefrontal cortex. In their extreme form, these changes will meet criteria for behavioral-variant frontotemporal dementia (bvFTD). This occurs in 16% of patients with ALS; 33% will have either behavioral or cognitive changes not meeting the threshold to be classified as bvFTD.
Features of more-advanced disease are as follows:
-
Muscle atrophy becomes more apparent
-
Spasticity may compromise gait and manual dexterity
-
Muscle cramps are common
-
Rarely, painful joint contractures may result from immobility
Progression of bulbar disease leads to the following:
-
Voice changes: Hypernasality and development of a strained, strangled vocal quality; eventually, speech may be lost
-
Swallowing difficulties, usually starting with liquids
-
Drooling
See Clinical Presentation for more detail.
Diagnosis
Definitive diagnosis may not be possible with early ALS. Confirmation of the disease may require a period of observation to document its progressive nature and to exclude alternative diagnoses.
Two recent developments have reframed the discussion regarding the early diagnosis of ALS.
First, a group of experts introduced the Gold Coast criteria [1] to establish the minimal changes needed to diagnose ALS. Based on these criteria, ALS can be diagnosed when there is a progressive disease with either (1) upper and lower motor findings in one body region; or (2) lower motor findings in two body regions – without an alternative demonstrable cause.
The image below illustrates the 4 regions of the body.
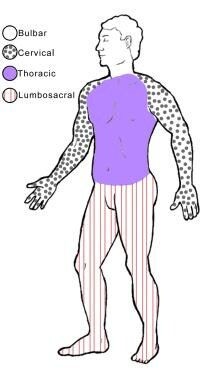 The 4 regions or levels of the body. Bulbar (muscles of the face, mouth, and throat); cervical (muscles of the back of the head and the neck, the shoulders and upper back, and the upper extremities); thoracic (muscles of the chest and abdomen and the middle portion of the spinal muscles); lumbosacral (muscles of the lower back, groin, and lower extremities).
The 4 regions or levels of the body. Bulbar (muscles of the face, mouth, and throat); cervical (muscles of the back of the head and the neck, the shoulders and upper back, and the upper extremities); thoracic (muscles of the chest and abdomen and the middle portion of the spinal muscles); lumbosacral (muscles of the lower back, groin, and lower extremities).
Second, drawing on the terms “Mild Cognitive Impairment” and “Mild Behavioral Impairment” developed by the cognitive/ behavioral neurology community, a group of ALS experts has put forth the concept of Mild Motor Impairment (MMI). [2]
This term emerged out of the standardized longitudinal observation of pre-symptomatic carriers of autosomal dominant genes for ALS within the pre-fALS study, a natural history observational study. [3]
When first evaluated, the patients had a completely normal neurological exam. As they were re-examined periodically a few patients developed subtle motor findings that did not meet diagnostic criteria for ALS and often had not been noticed by the patient. These changes progressed and preceded by a few months or years the emergence of symptomatic, diagnosable ALS.
The application of the concept of MMI to individual patients who are not ALS gene carriers presenting with subtle motor symptoms is expected to evolve. At the very least, the term implies that at this time we cannot predict if the patients will worsen and, if so, at what rate. Whether they should be sent for genetic testing or for determination of serum neurofilament light chain levels [4] are open questions.
Previously, the World Federation of Neurology (WFN) had developed a diagnostic algorithm (the revised El Escorial criteria) that combines clinical and, in some cases, electrophysiologic findings. [5] The degree of certainty of diagnosis is increased by the number of body segments that demonstrate upper motor neuron (UMN) and lower motor neuron (LMN) signs. UMN signs are mild weakness, spasticity, abnormally brisk reflexes, and pathological pyramidal reflexes; LMN signs are progressive weakness, wasting, and loss of reflexes and muscle tone. WFN categories are as follows:
-
Clinically definite ALS: UMN and LMN signs in at least 3 body segments
-
Clinically probable ALS: UMN and LMN signs in at least 2 body segments with some UMN signs in a segment above the LMN signs
-
Clinically probable, laboratory-supported ALS: UMN and LMN signs in 1 segment or UMN signs in 1 region coupled with LMN signs by electromyography (EMG) in at least 2 limbs
-
Clinically possible ALS: UMN and LMN signs in 1 body segment, UMN signs alone in at least 2 segments, or LMN signs in segments above UMN signs
-
Clinically suspected ALS: Pure LMN syndrome with other causes of LMN disease adequately excluded
The WFN framework is still in widespread use, primarily in clinical research settings, and is referenced for that reason. The qualifying terms “possible” and “probable” have been a source of confusion to the layperson. The Gold Coast criteria have done away with the qualifying terms. A previous, intermediate effort to simplify the diagnostic process resulted in the Awaji criteria, [6] which have found limited acceptance.
Hallmark findings in the electrodiagnosis of ALS are normal sensory nerve conduction studies and abnormal motor nerve conduction studies, with reduced compound muscle action potential amplitudes. The needle exam shows patterns characteristic of active, ongoing denervation and reinnervation of muscles.
In patients with familial ALS, genetic testing may be requested after appropriate counseling. The results of genetic testing may affect not only the patient, but also family members. Tests for the SOD1, TARDBP (coding for TDP-43), FUS, ANG, C9orf72, and FIG4 genes and for the gene causing Kennedy disease are available commercially. Patients with other forms of familial ALS may be referred to centers with a research interest in familial ALS.
See Workup for more detail.
Management
American Academy of Neurology recommendations for management of patients with ALS can be summarized as follows: [7, 8]
-
Riluzole should be offered to all patients with ALS to slow disease progression; since the AAN recommendations were published, additional drugs (edaravone, tofersen) have been approved by the FDA
-
Enteral nutrition via percutaneous endoscopic gastrostomy (PEG) should be considered to stabilize body weight in patients with impaired oral intake; PEG placement probably prolongs survival to some degree; PEG placement when forced vital capacity (FVC) is still over 50% predicted minimizes risk of insertion
-
Noninvasive ventilation (NIV) should be offered to treat respiratory insufficiency to prolong survival and slow the decline of FVC; NIV may be considered at the earliest sign of nocturnal hypoventilation or respiratory insufficiency
-
Mechanical insufflation/exsufflation may be considered to clear secretions in patients with reduced peak cough flow, particularly during an acute lower respiratory infection
-
Creatine and high-dose vitamin E should not be used
Invasive ventilatory support, requiring tracheostomy, may be considered in the following cases:
-
Patients who present with respiratory failure and who are otherwise largely neurologically intact
-
Patients who want to be kept alive using long-term invasive ventilatory support as their disease progresses
-
Patients in whom secretions cannot be managed and who therefore cannot benefit from noninvasive ventilatory support (this occurs very rarely)
-
Muscle relaxants to relieve spasticity
-
The combination of dextromethorphan and quinidine (Nuedexta) to decrease emotional lability (pseudobulbar affect)
-
Anticholinergics and sympathomimetics for sialorrhea
-
Mucolytics for thickened secretions
-
Lorazepam for anxiety
-
Selective serotonin reuptake inhibitors (SSRIs) for depression
-
Nonsteroidal anti-inflammatory drugs (NSAIDs), tramadol (Ultram), ketorolac (Toradol), morphine (immediate or extended release), or transdermal fentanyl for pain
See Treatment and Medication for more detail.
Background
Amyotrophic lateral sclerosis (ALS) is the most common degenerative disease of the motor neuron system. The disorder is named for its underlying pathophysiology, with “amyotrophy” referring to the atrophy of muscle fibers, which are denervated as their corresponding anterior horn cells degenerate. “Lateral sclerosis” refers to the changes seen in the lateral columns of the spinal cord as the upper motor neuron (UMN) axons in these areas degenerate and are replaced by fibrous astrocytes (gliosis).
ALS is a fatal disease, with a median survival period of 3 years from onset of weakness. [9] (See Prognosis.) Aspiration pneumonia and medical complications of immobility contribute to morbidity in most patients with the disease.
ALS was first described in 1869 by the French neurologist Jean-Martin Charcot and hence is also known as Charcot disease; however, it gained popular recognition and its best-known eponym in the United States after the baseball player Lou Gehrig announced his diagnosis with the disease in 1939. [10, 11, 12, 13, 14] ALS is also known as motor neuron disease (MND).
It has long been held, that “the cause of ALS is unknown." This stark statement needs to be retired, as it shuts the door on recognizing how much is actually known about ALS pathogenesis. It is more correct to say, today, that we have a fairly good understanding of how ALS gets started and how it evolves. We no longer think in terms of a single cause for initiation of the disease, but rather in terms of multiple potential causes and pathways. (See Disease Pathogenesis.)
Most contemporary research focuses on unveiling the downstream “final common pathway” mechanisms thatlead to cell death, hoping to find ways of interfering with these “downstream” mechanisms and extending patient survival.
Two exceptions are the study of the role of mutant SOD1 in generating and propagating ALS within the motor systems of carriers of an SOD1 gene and the study of the role of misfolded TDP-43 in spreading disease in the motor systems of carriers and most non-carriers of TDP-43 mutations, including all sporadic cases.
In familial ALS due to an SOD1 mutation, the altered gene product is (1) the agent of spread of the disease in the motor network and (2) its accumulation and aggregation in motor neurons leads to their demise. An intrathecal treatment (tofersen) that interferes with production of mSOD1 has been developed and approved for treatment of this form of familial ALS [REF as above].
In contrast, TDP-43 is a nuclear-to-cytoplasmic mRNA transporter protein that misfolds and precipitates in the motor neuronal cytoplasm of patients with sporadic ALS /FTLD and most cases of familial ALS/ FTLD, including but not limited to those inheriting a mutated TDP-43 gene. Abnormal misfolded TDP-43 derived from precipitate of familial (TDP-43 mutant) or sporadic FTLD cases can spread within the motor neuronal system. [15]
Degenerative effects of ALS
ALS is one of the system degeneration diseases, disorders that cause networks that work together in health to disintegrate together in an organized manner. [16, 17] ALS results from the systematic dismantling of the motor neuron system, with the clinical manifestations in each patient deriving from the site of onset and cell type involved; the relative affinity of the dismantling process for prefrontal, upper and lower motor neurons; and the rate of the disease’s spread within the network. [18]
In its classic form, ALS affects motor neurons at 2 or more levels of the motor neuron network supplying multiple regions of the body. It affects lower motor neurons (LMNs) that reside in the anterior horn of the spinal cord and in the brain stem, corticospinal UMNs that reside in the precentral gyrus, and, frequently, prefrontal motor neurons that are involved in planning or orchestrating the work of the upper and lower motor neurons. [19] (See Pathophysiology.)
Loss of LMNs leads to progressive muscle weakness, wasting (atrophy), and fasciculations, with loss of reflexes and muscle tone. Loss of corticospinal UMNs usually leads to milder weakness associated with stiffness (spasticity), which may be severe, and abnormally brisk reflexes.
Loss of prefrontal neurons may result in special forms of cognitive impairment that include, most commonly, executive dysfunction but that may also include an altered awareness of social implications of one’s circumstances and, consequently, maladaptive social behaviors. [20] In its fully expressed forms, the prefrontal dysfunction meets established criteria for frontotemporal dementia. [21, 22] Loss of ability to integrate motor function (apraxia), a premotor function, is seen at times. It is more noticeable in limbs that are not overly weak.
Types of motor neuron disease
Classic ALS
The term classic ALS is reserved for the form of disease that involves upper and lower motor neurons. The classic form of sporadic ALS usually starts as dysfunction or weakness in one part of the body and spreads gradually within that part and then to the rest of the body. [23] Ventilatory failure results in death 3 years, on average, after the onset of focal weakness. The rate of disease progression varies widely, however, with some patients dying a few months after experiencing their first symptom and others still walking 10 years afterward.
Progressive muscular atrophy and flail limb syndrome
The disease may be restricted to LMNs. When the pattern of LMN involvement is asymmetrical, the disorder is termed progressive muscular atrophy (PMA).
Most patients with PMA have a course indistinguishable from that of patients with classic ALS (except for the absence of UMN findings).
Kim et al concluded that PMA should be considered a form of ALS. [24] Review of the medical records of 91 patients with PMA and 871 with ALS showed that patients with PMA were more likely to be male, to be older, and to live longer than those with ALS, but risk of death increased with age at onset in both patient groups and UMN signs developed in 22% of patients with PMA within 61 months after diagnosis. [24]
In the study, demographic and other clinical variables did not differ at diagnosis between patients who did or did not develop UMN signs. In PMA, as in ALS, the factors present at diagnosis that predicted shorter survival were greater number of body regions affected, lower FVC, and lower ALSFRS-R score.
Patients with a symmetrical pattern, called flail limb syndrome, have a course that may be far longer. [25, 26]
Primary lateral sclerosis
When only UMNs are involved, the disease is called primary lateral sclerosis (PLS). The course of PLS differs from that of ALS and is usually measured in decades. [27] PLS should not be considered “a form of ALS,” and is a distinct entity.
Progressive bulbar palsy
Rarely, the disease is restricted to bulbar muscles, in which case it is called progressive bulbar palsy (PBP). In most patients who present with initial involvement of bulbar muscles, the disease evolves to classic ALS.
Familial ALS
Worldwide, a family history of ALS is obtained in about 5% of cases; these patients have familial ALS. Most familial ALS is inherited in an autosomal dominant pattern, [19] often with reduced penetrance, but other patterns, such as X-linked or autosomal recessive inheritance, are seen (see Etiology.)
The fact that in most patients ALS is sporadic does not preclude a genetic contribution to the disease in these cases. ALS as a whole is best thought of as a disease showing complex inheritance.
Complications
Complications of ALS can include the following:
-
Progressive inability to perform activities of daily living (ADLs), including handling utensils for self feeding
-
Deterioration of ambulation
-
Aspiration pneumonia
-
Respiratory insufficiency
-
Complications from being wheelchair-bound or bedridden, including decubitus ulcers and skin infections (while rare in patients with ALS, these complications can emerge if appropriate padding is not used)
-
Deep vein thromboses and pulmonary emboli (these are rare in patients with ALS, but have been encountered with greater frequency in the active treatment arm of some clinical trials)
Diagnosis and treatment
The diagnosis of ALS is primarily clinical. Electrodiagnostic testing contributes to the diagnostic accuracy (see Clinical Presentation and Workup). Making a diagnosis is important to patients and families, allowing them to stop the search for alternative causes of a patient's disability and to focus their attention on treatment.
The Gold Coast criteria provide the minimal requirements for a definitive diagnosis of ALS, and have removed the use of “possible” and “probable” as qualifiers. In a patient presenting with acquired, progressive weakness, ALS may be diagnosed it there are either (1) upper and lower motor findings in one body region or (2) lower motor findings in two regions without an alternative demonstrable cause.
Although ALS is incurable, there are treatments that can extend the length and meaningful quality of life for patients (see Treatment).
Mechanism-specific treatments directed at the processes that cause the disease to evolve after it has expressed itself sufficiently to be diagnosed may, at best, have an ameliorative effect. Treatments that halt the spread of the disease may be more effective than those that try to salvage affected motor neurons. Treatments have emerged in both categories. However, the mainstay of ALS therapy remains adaptive treatments directed at the clinical manifestations of the disease.
Pathophysiology
ALS should not be considered a single disease entity, but rather a clinical diagnosis for different pathophysiologic cascades that share the common consequence of causing preferential progressive loss of motor neurons and the orderly dismantling of the motor neuron system.
ALS mechanisms
Previously, research into the mechanisms resulting in sporadic and familial types of ALS had examined several possibilities. For example, excitotoxicity was suggested to occur secondary to overactivation of glutamate receptors.
Oxidative stress linked to free radical formation was also explored as a cause of ALS, owing to the discovery of mutations in the free radical–scavenging enzyme superoxide dismutase 1 (SOD1). [28] Mitochondrial damage was implicated as a possible mechanism as well, as was autoimmunity to calcium ion channels.
The observation of cytoskeletal proteins in cellular inclusions led to consideration of neurofilament defects as another possible cause of ALS. Inclusions in general implicated defects in the proteasome system were considered as a possible unifying mechanism.
More recent research has focused on RNA processing, because several genetic risk factors for ALS are involved in this metabolic pathway, and aggregation of proteins involved in RNA metabolism has been seen in most forms of ALS. Apoptosis has emerged as a possible method of neuronal death, although this is not certain.
Despite such research, no direct mechanism for ALS has been identified. Most investigators and clinicians agree that various factors, possibly a combination of some or all of the above processes, may lead to development of the disease. [29, 30]
If ALS is considered under the umbrella of neuronal system degenerative diseases, then the specificity for the motor system attacked by the disorder can be attributed to a pathologic process that arises within and spreads through the motor neuron system. Similarly, the focal onset (with subsequent spread) can be compared with the pathogenesis of prion disease (focal onset of a misfolded protein and its spread) or malignancy (a single DNA change or summative mutations, with a final one that confers the pathologic activity and its subsequent spread).
Prionlike propagation of misfolding of proteins—in particular, SOD1 and the 43 kDa transactive response DNA binding protein (TDP-43)—has been proposed as a mechanism for the regional spread of ALS symptoms. [28] The accumulation of misfolded proteins has parallels in other neurodegenerative diseases, including Alzheimer, Parkinson, and Huntington disease.
Axonal degeneration
Motor axons die by Wallerian degeneration in ALS, and large motor neurons are affected to a greater extent than smaller ones. This process occurs as a result of the death of the anterior horn cell body, leading to degeneration of the associated motor axon.
As the axon breaks down, surrounding Schwann cells catabolize the axon's myelin sheath and engulf the axon, breaking it into fragments. This forms small ovoid compartments containing axonal debris and surrounding myelin, termed myelin ovoids. Ovoids then are phagocytized by macrophages recruited into the area to clean up debris.
This type of axonal degeneration can be seen in the brain on biopsy as atrophy and pallor of myelinated motor axons in the corticospinal tracts. In cases in which the disease has been active for a long time, atrophy of the primary motor and premotor cortex may be seen as well. On biopsy of the spinal cord, degeneration of the myelinated motor axons with associated atrophy of the anterior motor roots of the spinal cord can be observed.
Wallerian degeneration also occurs peripherally, and collateral branches of surviving axons in the surrounding area can be seen attempting to reinnervate denervated muscle fibers. On muscle biopsy, various stages of atrophy are noted from this pattern of denervation and subsequent reinnervation of muscle fibers.
In typical ALS, certain motor neurons are spared until very late in the disease process. In the brain stem, these include the oculomotor, trochlear, and abducens nerves. In the spinal cord, the posterior columns, spinocerebellar tracts, nucleus of Onuf (which controls bowel and bladder function), and the Clarke column generally are spared, though the Clarke column can be affected in the familial form of the disease.
Pathways to cell death
Pathways that lead to cell death in ALS may be mediated by the following: [31]
-
Oxidative damage
-
Mitochondrial dysfunction
-
Caspase-mediated cell death (apoptosis)
-
Defects in axonal transport
-
Abnormal growth factor expression
-
Glial cell pathology
-
Glutamate excitotoxicity
-
Aggregation of abnormal proteins
Mutations in the copper/zinc superoxide dismutase 1 (SOD1) gene, which encodes an important antioxidant protein, have been seen in up to 20% of familial ALS patients. [32] Studies in transgenic mice carrying the human SOD1 mutation have provided important information on the pathophysiology of ALS. [31] Also, high levels of oxidative damage to proteins have been found in serum, urine, and cerebrospinal fluid samples from patients, as well as in postmortem samples of patients with both sporadic ALS and SOD1 -familial ALS. [33, 34, 35]
Inferences from animal models, including transgenic models of familial disease, to sporadic human disease are tenuous. However, recognition of the role of glutamate excitotoxicity in sporadic disease and in animal models paved the way to the testing and approval of riluzole, the first treatment that was shown to ameliorate the course of sporadic ALS, extending patients’ lives by 2-3 months. [36, 37]
Derangements of RNA metabolism
The findings below have placed derangements of RNA metabolism at the core of current thinking with regard to the pathophysiology of most types of ALS.
TARDBP gene
In 2006, ubiquitinated inclusions containing pathologic forms of TAR DNA-binding protein-43 (TDP-43) were identified in the cytoplasm of motor neurons of patients with sporadic ALS and in a subset of patients with frontotemporal dementia. [38, 39] TDP-43 is an RNA-processing protein that is normally localized predominantly in the nucleus.
Shortly after their identification in sporadic ALS, TDP-43–positive cytoplasmic inclusions were identified in patients with non-SOD1 familial ALS, [40, 41] and mutations in the gene on chromosome 1 coding for TDP-43 were identified in patients with sporadic and familial ALS. [42, 43, 44, 45, 46, 47]
Mutations in the TARDBP gene, which codes for TDP-43, account for 5% of patients with familial ALS. In addition, TDP-43 inclusions have been found in more than 90% of patients with sporadic ALS, in patients with Guamanian parkinsonism-dementia complex, [48] in the majority of patients with frontotemporal dementia, and in patients with familial British dementia. [49] A review of the continuum of multisystem TDP-43 proteinopathies concluded that the phenotypic expression is linked to the specific cells that are affected by the proteinopathy. [50]
FUS/TLS gene
In 2009, two groups [51, 52] reported that ALS-6, an autosomal dominant form of ALS, results from mutations in the gene for another RNA-processing protein, fused in sarcoma/translated in liposarcoma, or FUS/TLS. (The gene, FUS/TLS, is located on chromosome 16.) Patients these mutations have cytoplasmic inclusions containing FUS/TLS but not TDP-43. Usually, FUS/TLS, like TDP-43, is concentrated in the nucleus. Mutations in FUS/TLS account for 4% of patients with familial ALS.
Additional evidence
Further support for this idea has come from the following: [53, 54]
-
Association and functional studies of another RNA-processing protein, ELP3, in which variants apparently influencing expression alter the risk of ALS
-
The observation that other ALS genes, such as ANG, have a second role in RNA metabolism
-
The examination of genes implicated in related motor neuron diseases, such as SMN, GARS, and others that cause spinal muscular atrophy, which are also involved in this pathway
In 2011, researchers reported that a large hexanucleotide repeat expansion in the noncoding region adjacent to the C9orf72 gene, which is located on the short arm of chromosome 9, accounts for nearly 50% of familial ALS and frontotemporal dementia (FTD) in the Finnish population and more than a third of familial ALS in other groups of European ancestry. [55, 56] It is the most common mutation seen in patients with sporadic ALS. One effect of this mutation is the formation of nuclear RNA foci containing antisense RNA repeats. In addition, a novel mechanism of poly-dipeptide production, repeat-associated non-ATG translation (RAN) [57] has been shown to occur in carriers of the hexanucleotide expansion. [58] The abnormal polypeptides form cytoplasmic deposits. It is unclear how these deposits cause disease. In particular, since median age of onset of C9orf72-associated ALS is the same as that of sporadic ALS, and the deposits precede clinical disease by years, it is unclear how the nuclear or cytoplasmic deposits cause ALS or FTD.
Role of TDP-43 in disease propagation
TDP-43 is a nuclear-to-cytoplasmic mRNA transporter protein that misfolds and precipitates in the motor neuronal cytoplasm of patients with sporadic ALS /FTLD and most cases of familial ALS/ FTLD, including but not limited to those inheriting a mutated TDP-43 gene. Abnormal misfolded TDP-43 derived from precipitate of familial (TDP-43 mutant) or sporadic FTLD cases can spread within the motor neuronal system. [15]
STATHMIN2 – Linking deranged mRNA metabolism and motor neuron degeneration
A link between TDP-43 precipitation and motor neuron degeneration has been identified. [59]
The authors cite: “TDP-43 regulates expression of the neuronal growth-associated factor stathmin-2. Lowered TDP-43 levels, which reduce its binding to sites within the first intron of stathmin-2 pre-messenger RNA, uncover a cryptic polyadenylation site whose utilization produces a truncated, non-functional mRNA. Reduced stathmin-2 expression is found in neurons trans-differentiated from patient fibroblasts expressing an ALS-causing TDP-43 mutation, in motor cortex and spinal motor neurons from patients with sporadic ALS and familial ALS with GGGGCC repeat expansion in the C9orf72 gene, and in induced pluripotent stem cell (iPSC)-derived motor neurons depleted of TDP-43. Remarkably, while reduction in TDP-43 is shown to inhibit axonal regeneration of iPSC-derived motor neurons, rescue of stathmin-2 expression restores axonal regenerative capacity." [59]
These and subsequent findings led to the launch in April 2023 of a phase I clinical trial evaluating the safety and tolerability of QRL-201 in ALS. [60] QRL-201 is an investigational agent designed to restore STATHMIN-2 (STMN2) expression in patients with amyotrophic lateral sclerosis (ALS).
The significance of these developments is that the understanding of the pathophysiology of ALS has moved upstream from the final consequences of the disease, with identification (a) of specific agents of propagation of the disease within the motor system and (b) of a specific protein that when removed results in motor neuronal loss, which can be protected against if its presence if restored. Targeting these pathophysiological mechanisms is more likely to lead to clinically meaningful slowing or possibly halting of disease progression that has been possible with interventions dealing with the end-stage processes impacting death of diseased motor neurons. [61, 62]
Genetic influence on rate of disease progression
One of the most significant aspects of ALS, which varies between individuals thus contributing to the heterogeneity of the disease, is its rate of progression. Several studies have identified genetic conributions to this variability.
Exploring the non-coding genome
The noncoding genome is substantially larger than the protein-coding genome but has been largely unexplored by genetic association studies. [63] A region-based rare variant association analysis of > 25,000 variants in untranslated regions of 6139 ALS whole genomes and the whole genomes of 70,403 non-ALS controls resulted in identification of interleukin-18 receptor accessory protein (IL18RAP) 3' untranslated region (3'UTR) variants as significantly enriched in non-ALS genomes and associated with a fivefold reduced risk of developing ALS. [63]
The finding is of particular significance because it explored genome regions that had not been looked at previously. It remains to be seen, if additional non-coding regions remain to be discovered, and how identification of protective genetic variants can be translated into disease prevention in individuals not carrying those variants.
The role of microRNAs in ALS
MicroRNAs (miRNAs) are short (21-23 nucleotid long), single-stranded, non-coding RNA chains. They regulate the translation of mRNA to protein by binding to complementary RNA segments on mRNA, thereby interfering with mRNA translation. Upregulation of miRNA results in less mRNA translation, down regulation of miRNA results in more mRNA translations. Each miRNA may regulate several hundred mRNAs and each mRNA may be regulated by many miRNAs. MiRNAs determine the identity of specific cells as they differentiate from stem cells. Derangements in miRNA function may result in cellular dedifferention and the emergence of malignancies. [64]
MiRNA dysregulation has been identified in neurodegenerative diseases, as well as ALS. MiRNA profiles have been put forth to serve as biomarkers for the disease, and specific miRNSa have been suggested as linkd to ALS pathogenesis and pathophysiolog, and as therapeutic targets. [65, 66]
Disease onset (pathogenesis)
Making the distinction between the pathogenesis and pathophysiology of ALS matters because the mechanisms underlying each of these stages are probably different. This means that interfering with these mechanisms likely requires different approaches. The interventions to prevent disease onset are probably not the same as those required to slow or halt its progression after onset. Prevention of ALS requires modifying or removing factors that are part of disease pathogenesis. A precondition is identifying probable risk factors for ALS. [67]
In contrast to the approach to understanding the pathophysiology of ALS, which relies on direct biological experiments, the mechanisms that lead to disease onset (ie, pathogenesis) have been inferred from strong circumstantial evidence. In patients with familial ALS, it is reasonable to assume that the abnormal gene or gene product plays a role in triggering disease onset and may have a role in disease propagation, but having an abnormal gene is neither necessary nor sufficient for developing ALS.
Additional factors must be postulated to intervene between birth and disease onset even in patients who develop familial ALS, because the disease does not appear to start at birth, and within a given family there is great variability in the age of onset. Having normal copies of these genes does not prevent development of sporadic ALS.
ALS initiation is a multistep process. [68] In all likelihood, it takes place in a cortical motor neuron [69] with or without its immediate environment, akin to the initiation of malignancies in dividing cells. The number of steps is 6 in sporadic ALS, [68] and fewer in carriers of genes for the disease. Different genes require a different number of additional steps for disease initiation. [70] The need for additional steps in patients who are gene carriers explains why they do not have ALS from birth, and why not all carriers develop the disease (“incomplete penetrance.”)
A family history of the disease is obtained in about 5% of patients, and twin studies show a genetic contribution with heritability of about 61%. [71] More recently, upto 20% of patients presenting with sporadic ALS are found to be carriers of pathogenic or potentially pathogenic genes. [72]
The precise percentage and genes represented depend on the population. In some cases, ALS overlaps clinically, pathologically, and biologically with frontotemporal dementia, and it may share common biologic susceptibility mechanisms with Alzheimer’s disease, Parkinson’s disease, and other neurodegenerative diseases. [73, 74, 55, 56] (See Etiology.)
The multistep hypothesis for disease pathogenesis provides a fairly good idea regarding how and where ALS is initiated. Application of new tools has brought us closer to elucidating the precise cortical pathways involved. A report describes the use of hierarchical clustering on the 5000 most variably expressed autosomal genes identified from post-mortem motor cortex expression data of people with sporadic ALS to indentify networks in which they differed from controls. [75] Three molecular phenotypes were identifed, which reflect the proposed major mechanisms of ALS pathogenesis: synaptic and neuropeptide signalling, excitotoxicity and oxidative stress, and neuroinflammation. Known ALS risk genes were identified among the informative genes of each cluster. Phenotype analysis identified distinct cluster-related outcomes associated with progression, survival and age of death. [75]
The significance of these findings is that (1) they provide genetic underpinnings for the development of sporadic ALS; (2) they localize these underpinnings to the motor cortex; (3) they confirm that the ALS phenotype may be produced through different pathogenic mechansims, with mechanism-related phenotypic variability.
In summary, our current understanding of ALS pathogenesis is sufficiently advanced, that it is time to retire the adage “the cause of ALS is unknown.” It is more correct to say that we have a fairly good understanding of how ALS is initiated and how it spreads, new and more specific information is emerging every year, and that this information has led and is leading to clinical trials focusing more directly on the processes involved early in the course of the disease.
Course of the disease
Loss of motor neurons bridges disease pathophysiology and its clinical expression. When advanced, this loss results in the characteristic picture seen in cross-sections of the spinal cord in ALS. At the level of the muscle, loss of discrete LMNs causes loss of innervation of individual motor units.
Early in the disease, surviving nerve fibers establish connections and reinnervate motor units that have lost their connection to axons that have died; as a result, larger motor units are formed. These large motor units manifest in histologic stains as fiber-type grouping. (See the image below.) They also have special characteristics on electromyographic testing. Later in the disease, when the motor neurons that supply the large motor units die, group atrophy ensues.
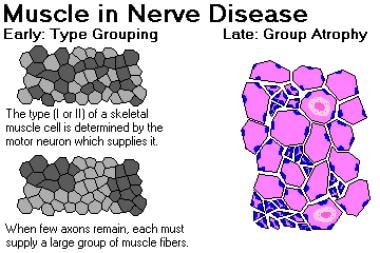 Muscle in nerve disease. Image courtesy of Dr. Friedlander, Associate Professor and Chair of Pathology at Kansas City University of Medicine and Biosciences.
Muscle in nerve disease. Image courtesy of Dr. Friedlander, Associate Professor and Chair of Pathology at Kansas City University of Medicine and Biosciences.
As long as reinnervation can keep up with denervation, clinical weakness may not be detectable, although loss of dexterity may occur. However, as the motor units grow larger and their numbers decrease, the earliest consequence is that affected muscle may fatigue faster than muscle with normal motor units; consequently, one of the first symptoms of ALS may be fatigability of function in the region of onset (for example, “his speech would become muffled toward the end of his sermons”).
As the number of motor units innervating a muscle decreases further, reinnervation can no longer keep up with denervation, permanent weakness develops and progresses, and the affected muscles gradually atrophy. In general, loss of cortical neurons may also result in weakness, but spasticity manifesting as stiffness is a more prominent and disabling UMN symptom.
Risk factors and triggering of onset
Acquired nucleic acid changes may trigger disease onset in sporadic ALS. [76] The past 10 years have seen an increase in evidence supporting this hypothesis. This hypothesis relies on the observation that smoking is the only established risk factor for sporadic ALS [77, 78] and provides a mechanism by which smoking might cause the disease—namely, by induction of changes in nucleic acids. It is supported by clinical observation that age-specific incidence of ALS increases with age. It follows a similar logic that suggests that the alkylating components in the cycad are responsible for delayed onset of Western Pacific ALS/PDC. [79, 80]
Simultaneous initial involvement of cortical and spinal motor neurons responsible for the same body part in ALS and the independent spread of disease at spinal and cortical levels has been shown. [81] These observations have been replicated, [82] although other patterns of spread are sometimes seen. They establish an irrefutable role for corticospinal neurons in the early spread of ALS and provide an observational foundation for postulating the existence of a focus of onset and one or more "agents of spread." [69]
Further support for this hypothesis comes from a statistical examination of acquired somatic mutation rates in humans. Somatic mutations inevitably occur during the many cell divisions required for the single-cell zygote to develop into a full organism; those mutations result in genetic mosaicism, and a small focus of genetically altered cells could be a trigger for ALS. [83]
The increase, with age, of age-specific incidence of sporadic ALS suggests that as time passes there is greater chance for changes to accumulate in nucleic acids that will lead ultimately to the development of ALS. This observation has been recently subjected to confirmatory quantitative analysis. [68] This analysis showed that ALS incidence increases with age in a logarithmic fashion, and the slope of log incidence vs. log age is 5. This suggests a multi-step process, analogous to carcinogenesis, [82] with 6 steps needed for ALS to be triggered.
An alternative trigger for disease onset might be appearance of a misfolded intracellular protein that induces other proteins to misfold, with cell-to-cell transmission of the misfolded protein within the motor network. The difference from classic prion disease is lack of transmissibility by inoculation to other organisms, and the confinement to a neuronal system, or network, with a common function. Hereditary or acquired nucleic acid changes may increase the likelihood that a gene product would be susceptible to misfolding, thus triggering disease onset.
The recent identification of the non-coding C9ORF72 hexanucleotide expansion in many familial and some sporadic ALS cases opens up a possibility that failure of regulation of a normal gene product may underlie ALS initiation and spread. [84, 85, 86, 87, 88, 89] In a broader sense, generation of a faulty regulatory gene product responsible for motor network maintenance, or failure to regulate such a product, may account for the specific disintegration of the motor network. MicroRNAs are particularly attractive candidates for this role.
The affirmation of spread substantiates the concept of a biologic focal onset for ALS. This in turn lends credibility to the concept of a focal trigger for ALS onset that generates the production of 1 or more agents of spread. [76]
Under this hypothesis, disease phenotype in each patient depends on the site of onset and the relative affinity of the specific agent of spread in that patient to motor neurons at the different hierarchical levels of the motor system (prefrontal, corticospinal, spinal/bulbar). [69] The concept of preferential affinity of the agent of spread may apply even to specific motor neurons within a given hierarchy, resulting, for example, in the special phenotypes in which LMNs are predominantly affected (flail arm syndrome, flail leg syndrome). [26]
Most of the biochemical changes found in the upper and lower motor neurons of diseased patients are probably downstream from those that initiate the disease and cause its spread. Some of these changes may represent the processes by which the motor neurons die, but others may reflect the efforts of the motor neurons to survive by compensating for, or “fighting,” the primary pathologic processes driving progression of ALS.
Etiology
Most amyotrophic lateral sclerosis (ALS) cases are sporadic. We have a fairly good understanding of how sporadic ALS is initiated and how it spreads. New and more specific information is emerging every year (See Disease Onset above). Many abnormal genes have been identified in familial cases and are considered causal, although the precise mechanism by which they cause ALS is unknown for most, with the exception of SOD1 and TDP43.
All of the mutated genes found to give rise to familial ALS have also been found in patients with sporadic ALS. This is to be expected, as the distinction between familial and apparently sporadic disease is based on obtaining a family history, which in turn depends on gene penetrance, family size, age of family members, and the level of knowledge of the person being interviewed. [90]
In addition, first-degree relatives of patients with apparently sporadic disease have an increased risk of ALS. The overall lifetime risk of ALS in these relatives is low, however (approximately 1 in 50). [91]
Familial cases
A family history of ALS is obtained in about 5% of cases and is often consistent with a Mendelian autosomal dominant pattern of inheritance. While most cases of familial ALS are indistinguishable from sporadic disease, others have unique phenotypes. [92]
Juvenile forms of ALS are more commonly familial. Mean age of onset is 10-20 years younger in patients with familial ALS than in patients with apparently sporadic disease, and variability in age of onset between families is greater than variability within families. [19] Age of onset may also be modified by genetic factors independent of the cause of ALS. [93, 94]
Many specific heritable gene mutations have been described in familial ALS (see Table 1, below). [13] A curated, up-to-date list that includes unpublished mutations, genotype-phenotype correlations, and tools for analysis is maintained on the ALSoD website.
Table 1. Familial Forms of ALS [95, 96, 97] (Open Table in a new window)
Gene |
Locus |
Protein |
Inheritance |
SOD1 (ALS1) |
21q22.11 |
Superoxide dismutase 1 (SOD1) |
AD* |
ALS2 |
2q33 |
Alsin (ALS2) |
Juvenile/AR** |
ALS3 |
18q21 |
Unknown |
AD |
ALS4 |
9q34 |
SETX |
Juvenile/AD |
ALSS |
15q15 |
SPG11 |
Juvenile/AR |
FUS (ALS6) |
16p11.2 |
FUS |
AD |
ALS7 |
20ptel-p13 |
Unknown |
AD |
ALS8 |
20q13.3 |
VABP |
AD |
ALS9 |
14q11.2 |
Angiogenin (ANG) |
AD |
TARDBP (ALS10) |
1p36.2 |
TAR DNA-binding protein (TARDBP) |
AD |
ALS11 |
6q21 |
FIG4 |
AD |
ALS12 |
10p13 |
OPTN |
AD; AR |
ALS13 |
12q24 |
ATXN2 |
AD |
ALSX |
Xp11 |
UBQLN2 |
X-linked |
C9orf72 (ALS-FTD) |
9q21-22 |
C9ORF72 |
AD |
ALS-FTD |
9p13.3 |
SIGMAR1 |
AD; Juvenile/AR |
PFL1 |
17p13.2 |
Profilin 1 |
AD |
*AD–autosomal dominant; **AR—autosomal recessive |
|||
About 10-20% of familial ALS cases result from a mutation in the copper/zinc superoxide dismutase 1 (SOD1) gene, also known as ALS1. In general, SOD1 ALS is a LMN form of the disease. [98] The other genes most commonly involved in familial ALS are C9orf72, FUS (ALS6) and TARDBP (ALS10).
SOD1 mutations
More than 140 allelic variations have been seen in SOD1. Some of these variations are characterized by a relatively predictable age of onset or rate of disease progression.
The traditionally used numbering of the amino acids in SOD1, which omits the start codon, is no longer in line with standard practice but will be used here. To translate to the modern numbering, an additional codon should be counted. For example, the D90A mutation frequent in Scandinavia should be p.D91A.
The most common SOD1 mutation in the United States is the A4V mutation, accounting for 50% of SOD1 ALS cases. It causes a rapidly progressive lower motor disease with a mean survival period of 1 year. The North American SOD1 A4V mutation descended from 2 founders (Amerindian and European) 400-500 years ago. [99]
Not all individuals with an SOD1 mutation develop ALS. SOD1 ALS has been shown to be a gain-of-function disease; knockout mice depleted of SOD1 do not develop ALS, and transgenic mice with 1 mutated and 2 normal genes have worse disease than those with 1 normal and 1 mutated gene. Misfolding and precipitation of the abnormal (and normal) SOD1 proteins are considered part of the pathophysiology of SOD1 ALS, and spread of abnormal SOD1 is considered to be the mechanism of spread of disease in mSOD1 patients. How the precipitation of misfolded SOD1 causes the LMN ALS phenotype is still notclear.
Work in animal models suggests that silencing from birth of the expression of mutant SOD1 by silencing RNA molecules (siRNA) may prevent disease onset in transgenic mouse models. [100] This is an exciting direction for research in humans with SOD1 mutation, but major barriers need to be overcome first, including demonstration that this approach is effective in halting the disease after its clinical onset. [92, 95, 96, 101] This goal has been attained. A treatment designed to silence mSOD1 after disease onset in humans has shown efficacy albeit limited in slowing disease progression [102] and has been approved by the FDA. [103]
TARDBP and FUS mutations
Gene mutations resulting in abnormalities in proteins that regulate RNA processing have been discovered in patients with autosomal dominant familial ALS. Mutations in the TARDBP gene, which codes for TDP-43, have been found in 5% of patients with familial ALS. [40, 41, 42, 43, 44, 45, 46, 47] Mutations in the FUS gene are found in 3-4% of familial ALS cases. [92]
The mechanism by which these mutations cause ALS is distinct from that which takes place in SOD1 mutations. Although ubiquinated pathologic TDP-43 aggregates have been found in motor neuron cytoplasm of patients with sporadic ALS, they are not specific for this disease and have been found in affected nonmotor cells in patients with Guamanian parkinsonism-dementia complex, [48] British familial dementia, [49] and Alzheimer disease, [104] as well as in most patients with frontotemporal dementia.
Thus, formation of pathologic TDP-43 and its ubiquination may prove to be a mechanism of cell death that is not specific to ALS and is triggered by upstream processes, causing clinical pathology that depends on the cells affected. Conversely, TDP-43 deposition may prove to be a nonspecific defense mechanism involving an unsuccessful attempt to mitigate the action of the true instigators of cell death in a spectrum of neurodegenerative diseases, or it may be an epiphenomenon common to many forms of neurodegenerative diseases. Transgenic animal models with mutated TDP-43 do not develop ALS. However, transfer of misfolded TDP-43 from cell to cell within the motor neuron network is implicated in disease propagation (See Role of TDP-43 in disease propagation, above).
C9orf72 mutation
Studies of families with familial ALS in which some individuals also had frontotemporal dementia found linkage to a region on chromosome 9p21 [105, 106, 107] Subsequently, a large genome-wide association study (GWAS) identified single-nucleotide polymorphisms (SNPs) associated with apparently sporadic ALS in the same region. This was confirmed in a further GWAS-wide association study of patients with apparently sporadic ALS and controls from 8 countries, [108] as well as in a Finnish study [109] using family-based samples.
In 2011, two groups reported the discovery of a hexanucleotide (GGGGCC) repeat expansion in the first intron of the chromosome 9 open reading frame 72 (C9orf72) gene—the function of which is as yet unknown—as the cause of chromosome 9p21–associated ALS and frontotemporal dementia. [84, 85] This expansion of hexanucleotide repeats (from ≤23 in normal individuals to thousands in affected individuals) appears to be the most common genetic abnormality in ALS and in frontotemporal dementia.
The repeat expansion was found in 46.0% of patients with familial ALS, 21.1% with sporadic ALS, and 29.3% with familial frontotemporal dementia, in the Finnish population. [85] In their analysis of an extended North American clinical series, DeJesus-Hernandez et al found the C9orf72 expansion in 23.5% of patients with ALS cases and 11.7% of patients with familial frontotemporal dementia. [84]
More recent reports have found the C9ORF72 repeat expansion in 22-57% of familial ALS patients (depending in part on geographic origin) and in 3.6-7% of sporadic ALS patients. [86, 87, 88, 89] The frequency of the mutation varies widely even within Europe. [110]
Haplotype analysis of 5 European cohorts has shown that the hexanucleotide repeat expansion in C9orf72 had a single founder and arose around 6300 years ago. [110] The haplotype from which the mutation arose is intrinsically unstable, with an increased number of repeats. [110]
The phenotype of C9orf72 -mediated ALS shows distinct pathology, with p62-positive, TDP43-negative inclusions in the cerebellum and hippocampus. [111] Clinically, patients with this mutation have an earlier onset of disease and are more likely to have bulbar-onset disease, cognitive and behavioral impairment, and a family history of frontotemporal dementia than are ALS patients who carry other known mutations.
Other genes in familial ALS
Mutation in the ubiquilin 2 (UBQLN2) gene has been identified as a cause of X-linked dominant familial ALS and ALS with frontotemporal dementia. [112] This finding is of interest because it directly implicates the proteasome pathway in ALS pathogenesis.
Mutation in the profilin 1 (PFN1) gene has been identified in families with familial ALS. [97] The protein encoded by PFN1 plays a critical role in the conversion of monomeric (G)-actin to filamentous (F)-actin. Thus, the identification of this mutation provides further support for the role of the cytoskeleton and axonal transport in ALS pathogenesis.
Sporadic cases
The most widely accepted hypothesis regarding the cause of sporadic ALS posits that interactions between genetic, environmental, and age-dependent risk factors trigger disease onset. (See the image below.) ALS shows complex inheritance, which means that Mendelian, non-Mendelian, and apparently sporadic patterns of inheritance are seen. Smoking is the only environmental risk factor identified to date that may be considered “established.” [77, 78]
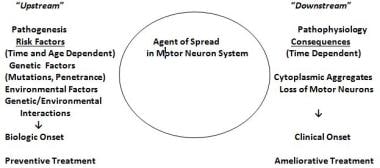 The genetic/environmental/age- and time-dependent interactions hypothesis for amyotrophic lateral sclerosis (ALS). Risk factors operate upstream to a putative biochemical transformation (likely an acquired nucleic acid or protein change), which causes the appearance of altered proteins or nucleic acids or abnormal quantities of normal proteins or nucleid acids. These agents spread within the motor system and cause the downstream disintegration of the motor system and the downstream biochemical, histologic, and clinical consequences of ALS. (Adapted from Armon C. What is ALS? In: Amyotrophic Lateral Sclerosis: A Patient Care Guide for Clinicians. Bedlack RS, Mitsumoto H, Eds. Demos Medical Publishing, New York, 2012:1-23)
The genetic/environmental/age- and time-dependent interactions hypothesis for amyotrophic lateral sclerosis (ALS). Risk factors operate upstream to a putative biochemical transformation (likely an acquired nucleic acid or protein change), which causes the appearance of altered proteins or nucleic acids or abnormal quantities of normal proteins or nucleid acids. These agents spread within the motor system and cause the downstream disintegration of the motor system and the downstream biochemical, histologic, and clinical consequences of ALS. (Adapted from Armon C. What is ALS? In: Amyotrophic Lateral Sclerosis: A Patient Care Guide for Clinicians. Bedlack RS, Mitsumoto H, Eds. Demos Medical Publishing, New York, 2012:1-23)
Several lines of evidence support the hypothesis that genetic risk factors may influence disease initiation in apparently sporadic ALS, apart from finding known Mendelian gene mutations in patients with no family history. Twin studies show a genetic contribution to apparently sporadic ALS, with heritability of 0.61. [71] Increased risk for ALS and (in some studies) clustering of non-ALS neurodegenerative disease is found in relatives of patients with apparently sporadic ALS. [91, 113, 114, 115]
Environmental risk factors
Smoking
Cigarette smoking was the first exogenous risk factor to be considered an established risk factor for ALS [77] (level A conclusion, based on 3 class II studies [116, 117, 118] and 1 class III study [119] ). In addition, a population-based study from the Netherlands demonstrated that current smokers are at increased risk for ALS, with an odds ratio of 1.38, and have shorter survival. [78]
Some aspects of the findings in these studies suggest that smoking may be implicated directly in causing the disease. Overall, studies have shown that active smokers have approximately double the risk of developing ALS compared with never smokers. Former smokers have an intermediate risk.
Identifying smoking as an established risk factor for ALS has the following major implications:
-
The findings provide a link between the environment and the occurrence of sporadic ALS; no link had previously been identified with this level of certainty
-
Since smoking has no redeeming features, avoidance of smoking may reduce the future occurrence of ALS
-
Future studies of risk factors in ALS need to be designed to precisely quantify active and passive smoking, to ensure that other putative risk factors confer a risk that is independent of their association with smoking
-
Since some of the mechanisms by which smoking causes other diseases in humans are understood fairly well, recognition of smoking’s role in the occurrence of ALS may help to pinpoint the biologic processes that initiate the disease
Focusing on processes at the initiation of sporadic ALS and close to its initiation, in order to account for its early spread within the motor system, may provide new avenues to treatments to stop its progression. This approach may augment the focus on processes that occur later in the course of the disease and cause the death of motor neurons directly.
The past few years have seen the application of Mendelian randomization methods to assessing risk factors for ALS. Two of the more contentious risk factors considered have been smoking and lipid levels. A 2022 review indicated that several studies conclude that there is a causal link between blood lipids and risk of ALS that has been replicated across different datasets as well as different populations. However, there is doubt that Mendelian randomization studies are useful for other putative risk factors, such as smoking and immune function. [120] These conclusions are subject to limitations acknowledged by the authors, and summarized in part here.
It is difficult to control for survival bias [121] and collider bias [122] in Mendelian randomization studies in ALS. These biases affect how patients and controls get to be included in the samples for Mendelian randomization studies. They affect differently smoking and cholesterol levels. Risk factors need to be sought in incidence samples. The samples used for ALS Mendelian randomization samples are prevalence samples. If the risk factor under consideration also affects the patients’ likelihood to be represented in the sample investigated, then finding its presence or absence may be misleading. When sought in prevalence samples, a risk factor may be missed if it is a risk not only for disease onset but also for shortened survival after disease onset, which is the case for smoking. It may be identified spuriously if it confers extended survival after disease onset, which is the case for elevated lipids. Moreover, smoking is a source of mortality competitive to ALS more than elevated lipids, hence may result in underrepresentation of patients in whom ALS has been initiated biologically but not manifested clinically before they succumbed to other smoking-related causes of mortality. Finally – most, if not all, studies considering the role of smoking are biased towards not detecting the effect, as they have not been able to control for the effects of passive smoking in patients and controls. [123]
As further Mendelian randomization studies are pursued in search ot risk factors for ALS – meticulous attention to methods of developing new patient and control samples, with particular emphasis on complete sampling of population-based, incident cases and appropriate controls, may ameliorate some of the limitations inherent in the existing samples. Results of Mendelian randomization studies need to be interpreted in the context of other available information, factoring in also the traditional viewpoints applied to infer causation from association, [124] applied to the 21st century. [125]
Air pollution
Air pollution has been associated with neurodegenerative diseases. [126] It has also been identified as a possible risk factor in ALS. [127, 128, 129]
The role of air pollution is currently being studied through a grant from the CDC to the University of Michigan. [130] Preliminary results reported at scientific meetings have been suggestive.
Military service
Putative risk factors include service in the US military during World War II, the Korean War, and Vietnam, [131] as well as deployment to the Persian Gulf in the 1991 Persian Gulf War. [132] However, close scrutiny has cast doubt on the quality of the evidence supporting the role of these factors in triggering ALS. [132, 133, 134, 135, 136] More recently, a 13-year follow-up study found no excess of ALS among Gulf War veterans. [137]
Repetitive head injuries
A possible increased risk of ALS in Italian professional soccer players was reported in 2005. [138, 139] Initially, it appeared that the apparent increase in risk may have resulted from underestimation of the expected number of cases of ALS. [140, 141, 142, 143, 144] However, a 5-year extension of the follow-up of this cohort showed an unambiguous excess of cases of ALS; 8 cases (including 3 new ones) were reported, even though the number of expected cases was 1.24. [145]
However, the ALS in the professional soccer players displayed atypical features; ie, 5 of the 8 cases had a bulbar onset, and 5 had been diagnosed between 2000 and 2006 (compared with 3 between 1980 and 1999 and none between 1970 and 1979). The authors concluded that the predilection for soccer players to develop ALS derives from a complex interplay between genetic predisposition for physical endurance and external factors such as drugs or herbicides. [145]
A subsequent report suggested that a form of motor neuron disease might develop in individuals, such as boxers, who have sustained repetitive injuries to the brain and developed chronic traumatic encephalopathy (CTE). [146] However, the claim that this was a novel form of motor neuron disease was challenged; instead, the possibility that these cases represented coincidental co-occurrence of ALS was proposed as more plausible. [147, 148, 149]
More recently, a study in retired US National Football League (NFL) players showed that, while their overall mortality was 50% less than expected, their mortality from neurodegenerative diseases was higher than expected. In particular, mortality from ALS and Alzheimer disease was 4-fold higher than expected. [150] These results are based on 7 individuals who died with Alzheimer disease and 7 individuals who died with ALS, out of a cohort of 3439 individuals.
The interpretation of this number as excessive appears to be a consequence of the method used to calculate the expected rate, [140] which may result in underestimation of that rate. In addition, when an apparent excess of neurodegenerative disease appears in the context of greatly reduced overall morality, the emergence of neurodegenerative deaths due to loss of competing causes of mortality needs to be considered.
These reports raised the question whether trauma to the head may be a risk factor for ALS. An evidence-based review of the literature concluded that for instances of isolated head trauma this was not the case. [151]
A subsequently published national population–based case-control study from Sweden found no association of ALS with severe head injury occurring more than 3 years before ALS diagnosis, nor was ALS associated with subtypes of head injury or repeated injuries occurring more than 3 years before diagnosis. [152] Exclusion of injuries occurring within 3 years of diagnosis is necessary to have some assurance that the injury occurred before biologic onset of the disease, which likely precedes clinical onset by several years. [153]
A population-based study from Rochester, Minnesota, showed no increased risk of neurodegenerative diseases among 438 players who played American football in high school between 1946 and 1956, despite poorer protective equipment and less regard for concussions compared with today, and no rules prohibiting head-first tackling. [154]
One report indicated that head injury does not alter disease progression or neuropathological outcomes in patients with ALS. [155]
In conclusion, the association of development of chronic traumatic encephalopathy with multiple instances of trauma to the head is well established, and has been recognized since it was described in boxers as “dementia pugilistica.” The question of if recurrent head trauma also increases the risk of developing ALS, specifically, doubles the risk, remains unresolved.
The balance of the evidence supports the conclusion that head trauma in general is not a risk factor for ALS; and the risk of repetitive head trauma for the general population is uncertain, as the data about risk derive from cohorts of professional athletes.
In the case of the Italian soccer players, their form of ALS was unusual, with most experiencing bulbar onset.
The special circumstances of the NFL players are also of uncertain generalizability, as the data are sparse. One review concluded that professional sports prone to repetitive concussive head and cervical spinal trauma were associated with substantially greater effects compared with (a) nonprofessional sports prone to repetitive concussive head and cervical spinal trauma; (b) professional sports not prone to repetitive head and neck trauma; or (c) nonprofessional sports not prone to repetitive concussive head and cervical spinal trauma. [156]
Risk factors other than the sport itself may be involved, including local environmental risk factors or ingestion of testosterone, anabolic steroids, or other drugs or supplements. [145, 157]
Other putative exogenous risk factors have not risen to the level of probable. These include exposure to pesticides, [158] postmenopausal hormone use, [67, 159] and physical exercise. [160]
Trauma, physical activity, residence in rural areas and alcohol consumption are probably not risk factors for ALS. [67] Indeed, in the population-based study from the Netherlands noted above, current alcohol consumption was associated with a reduced risk of ALS. [78]
Western Pacific ALS
Most of the research on Western Pacific ALS has focused on Guam. Ingestion of food products derived from the false sago palm, Cycas micronesica (recently separated from Cycas circinalis), was proposed by nutritional anthropologist Marjorie Whiting as the process predisposing to the development of this form of ALS. [161] Despite the cycad nut being subjected to an elaborate preparation process to rid it of toxins before being used as a substrate for flour, some toxic factor was presumed to remain. [162]
In addition, the cycad nut is consumed by the flying fox (a type of bat), which used to be part of the Chamorro peoples' diet on Guam. Toxins from the cycad nut may have been concentrated (bioamplified) in the bat and delivered to the human consumer. The consumption of the flying fox was higher in the mid-20th century than it is now. [163] Most flying foxes consumed in Guam currently are imported.
An epidemiologic study in Guam provided evidence consistent with that hypothesis; its conclusions have been challenged, [163] but the challenges themselves have been questioned. [162]
The nature of the putative toxic component of cycad that may be responsible for delayed-onset neurodegenerative disease has also been a matter of intense debate. One hypothesis is that cycad contains excitotoxic amino acids that do not exert an effect until many years after they have been ingested. [164, 165, 166]
An alternative hypothesis is that alkylating components induce changes in nucleic acids [79, 80] that increase the likelihood that subsequent, additional, age-dependent nucleic acid changes trigger disease onset in Guamanian ALS/Parkinson-dementia complex (ALS/PDC).
Epidemiology
Occurrence in the United States
Approximately 5600 people in the United States are diagnosed with ALS each year. The annual incidence is 2-3 per 100,000 population; this is about equal to that of multiple sclerosis and 5 times higher than that of Huntington disease. It is estimated that as many as 18,000 Americans may have ALS at any given time.
The lifetime risk for developing ALS for individuals aged 18 years has been estimated to be 1 in 350 for men and 1 in 420 for women. [140] These estimates are close to those reported from 4 European registries, using different methods. [167, 168, 169]
International occurrence
Age-adjusted European incidence data are similar to those for members of the US population who are of European descent. [167, 170] Most variability between countries has been attributed to different age composition or differences in case finding. More recent data, however, suggest that ethnic variability in disease incidence exists [171, 172] that may not be explained entirely by differences in case finding, with lower incidence in nonwhites or individuals of mixed ethnicity. Although this possibility is not supported by all studies, it merits further examination. [173]
Finland has one of the highest rates of ALS in the world; the disease occurs in the Finnish population nearly twice as frequently as it does in other populations of European ancestry. [109] A study from Finland found 2 clusters of cases based on geographic location at time of death and a cluster based on time of birth that closely matched one of the time-of-death clusters. [174] It was recognized that these results could be consistent with either a genetic or environmental cause. With the discovery of the hexanucleotide repeat expansion in C9orf72, most cases of ALS in Finland have been confirmed to be due to genetic factors.
Race-related demographics
In the United States, ALS affects whites more often than nonwhites; the white-to-nonwhite ratio is 1.6:1. [171] Uncertainty surrounds this finding, however, as it has been considered to be an artifact of reduced case-finding in nonwhites. This reservation may be less relevant today due to increased awareness of ALS in all communities, greater availability of health insurance coverage nationwide, and more widespread presence of ALS centers providing care regardless of the patient’s insurance status. Evidence for racial differences has come from an epidemiologic study in Cuba [172] where access to care is considered uniform.
Small population clusters have been identified that have higher rates of ALS. The Chamorro people of Guam and Marianas Island, residents of the Kii peninsula of Japan’s Honshu Island, and the Auyu and Jakai people of southwest New Guinea have a higher incidence of ALS than is found in populations elsewhere in the world. [13] The Chamorro population in Guam in the mid-20th century had an annual incidence of ALS (often in association with parkinsonism and dementia) as high as 70 cases per 100,000 (see Pathophysiology). [164] The incidence has since decreased to 7 cases per 100,000. These findings may be due to environmental exposure rather than to race.
Sex- and age-related demographics
For most of the lifespan, the incidence of ALS is higher in men than in women, with an overall male-to-female ratio of 1.5-2:1. [19] Later in life, the incidence tends to equalize; this occurs at age 40-50 years in some populations and after the age of 65-70 years in others. [175]
Onset of ALS may occur from the teenage years to the late 80s; the incidence rises with increasing age until approximately age 75-80 years. Mean age of onset of sporadic ALS is 65 years; mean age of onset of familial ALS ranges from 46-55 years.
Prognosis
ALS is a fatal disease. Median survival is 3 years from clinical onset of weakness. However, longer survival is not rare. About 15% of patients with ALS live 5 years after diagnosis, and about 5% survive for more than 10 years. Long-term survival is associated with a younger age at onset, being male, and limb (rather than bulbar) symptom onset. Rare reports of spontaneous remission exist. [176] In familial ALS that results from an alanine-to-valine mutation in codon 4 of the SOD1 gene (A4V mutation), average survival is 12 months from disease onset.81 Survival in other SOD1 mutations is greater than in sporadic ALS. [177]
Regionally limited forms of motor neuron disease (ie, brachial biplegia, lumbosacral biplegia, and progressive bulbar palsy [PBP] that remains restricted [178] ) progress slower than does classic ALS. Progressive muscular atrophy (PMA), distinct from classic ALS because of lack of upper motor neuron (UMN) findings, progresses at the same rate as classic ALS. UMN-predominant ALS progresses at a slower rate. These observations suggest that it is the loss of LMNs that determines the prognosis. Survival in cases of primary lateral sclerosis (PLS), which is, strictly speaking, not a form of ALS, is measured in decades.
Frontotemporal executive dysfunction may precede or follow the onset of ALS, but most patients with ALS do not have overt dementia, and cognitive impairment is usually subtle. [179] Approximately 15% of patients with ALS meet criteria for frontotemporal dementia (FTD). Patients with ALS associated with FTD have shorter survival than do those with ALS alone. [180, 181]
A readily available predictor of survival is the rate of observed disease progression. This may be estimated in more than one way. First is the time between symptom onset and diagnosis. Shorter time translates into worse prognosis. Second is the degree of loss of function at the time the patient is first seen, using quantitaitve measures such as the ALS Functional Rating Scale (ALSFRS). [182] However, not all losses on the ALSFRS-R are of equal prognostic significance: bulbar losses result in a worse prognosis than spinal losses of equal numerical value. Third, true estimates of rates of progression may be derived as a ratio between loss and time since symptom onset. The measurement of functional loss may be obtained using the ALSFRS-Revised (ALSFRS-R), the forced vital capacity (FVC) as percent of predicted, strength, or motor unit number estimates (MUNEs). [183, 184, 185, 186, 187] In each case, the current number is subtracted from a presumptive baseline to give the magnitude of the loss.
Multifactorial algorithms to predict survival and loss of critical functions have been developed. [188, 189, 190, 191]
In the 2021 meta-analysis by Su et al, [191] NFL (HR:3.70, 6.80, in serum and CSF, respectively), FTD (HR:2.98), ALSFRS-R change (HR:2.37), respiratory subtype (HR:2.20), executive dysfunction (HR:2.10), and age of onset (HR:1.03) were superior predictors for poor prognosis, but pLMN or pUMN (HR:0.32), baseline ALSFRS-R score (HR:0.95), duration (HR:0.96), and diagnostic delay (HR:0.97) were superior predictors for a good prognosis.
This meta-analysis also highlights the emergence of biomarkers as predictors of prognosis. Of these, Neurofilament Light (NFL) has been the most reliable at reflecting rate of progression, with higher levels reflecting faster progression. Use of biomarkers has not yet entered routine clinical practice but is becoming more frequent in the research setting to stratify patients based on a biological measure of disease progression.
Some prognostic algorithms are available as online tools, intended for use by physicians, recognizing that receiving stark unfavorable information online can be disturbing for patients.
A final consideration is what degree of prognostic precision is relevant to patients, and whether complex algorithms confer added precision that is meaningful to patients, beyond what may be inferred more intuitively by ascertaining their age, rate of progression and degrees of bulbar, respiratory and cognitive involvement at presentation.
Measures of disease progression
Roche et al proposed a system of stages (the King's staging system), the timing of which is standardized as proportions of elapsed time through the course of ALS. [192] The milestones, and their typical time of occurrence, are as follows:
-
Stage 1: Symptom onset (involvement of first region)
-
Stage 2A: Diagnosis (35% of the way through the disease course)
-
Stage 2B: Involvement of second region (38%)
-
Stage 3: Involvement of third region (61%)
-
Stage 4A: Need for gastrostomy (77%)
-
Stage 4B: Need for noninvasive ventilation (80%)
-
Stage 5: Death
It may be seen that most patients are diagnosed at a point at which ALS has extended to involve at least 2 regions and that the needs for gastrostomy and noninvasive ventilation (NIV) are usually recognized almost at the same time. These percentages are consistent with the numbers usually cited of 12 months’ mean time from onset to diagnosis and 3 years’ mean duration of disease from onset to death.
A standard operating procedure has been designed to help apply this staging system. [193]
An additional staging system, the Milano–Torino (MiToS) Staging system, has also been developed. It comprises six stages based on functional impairment as assessed by the revised ALS Functional Rating Scale (ALSFRS-R). [194]
The systems are complementary, with the King’s system predicated on anatomical progression and the MiTos system on functional decline. The King’s clinical staging has a higher resolution in early-mid diseases stages and the MiToS system in late disease stages. [193, 195, 196]
The need for these staging systems has arisen, in part, in order to permit demonstrating efficacy of treatments by showing by how many months they delay transition from one stage to another, thereby providing clinically meaningful measures of slowing disease progression, beyond what may be understood by percentage of slowing of a slope.
Discussing prognosis with the patient
Patients the author has surveyed have indicated ambivalence about being offered individualized information early in the course of the disease (when it may matter most). [197] The author does not offer patients individualized prognostic information at the first visit. When patients do request it, he asks them to consider the possible implications of the answers they may receive and to ask him again at a subsequent visit. It is also helpful to discuss the implications of the rate of disease progression, based on the joint observations of the patient and the physician.
Patient Education
The following education resources are available to patients with ALS:
-
ALS Association, Living With ALS Manuals
-
Muscular Dystrophy Association: MDA ALS Caregiver’s Guide
-
ALS 1996 and Beyond: New Hopes and Challenges. A Manual for Patients, Families and Friends (Fourth edition, 2007) [198]
Informational web sites include the following:
-
Motor Neurone Disease Association (England, Wales, and Northern Ireland)
For patient education information, see the Brain and Nervous System Center, as well as Amyotrophic Lateral Sclerosis (ALS, Lou Gehrig’s Disease) and Advance Directives.
-
The 4 regions or levels of the body. Bulbar (muscles of the face, mouth, and throat); cervical (muscles of the back of the head and the neck, the shoulders and upper back, and the upper extremities); thoracic (muscles of the chest and abdomen and the middle portion of the spinal muscles); lumbosacral (muscles of the lower back, groin, and lower extremities).
-
The genetic/environmental/age- and time-dependent interactions hypothesis for amyotrophic lateral sclerosis (ALS). Risk factors operate upstream to a putative biochemical transformation (likely an acquired nucleic acid or protein change), which causes the appearance of altered proteins or nucleic acids or abnormal quantities of normal proteins or nucleid acids. These agents spread within the motor system and cause the downstream disintegration of the motor system and the downstream biochemical, histologic, and clinical consequences of ALS. (Adapted from Armon C. What is ALS? In: Amyotrophic Lateral Sclerosis: A Patient Care Guide for Clinicians. Bedlack RS, Mitsumoto H, Eds. Demos Medical Publishing, New York, 2012:1-23)
-
Muscle in nerve disease. Image courtesy of Dr. Friedlander, Associate Professor and Chair of Pathology at Kansas City University of Medicine and Biosciences.
Tables
Gene |
Locus |
Protein |
Inheritance |
SOD1 (ALS1) |
21q22.11 |
Superoxide dismutase 1 (SOD1) |
AD* |
ALS2 |
2q33 |
Alsin (ALS2) |
Juvenile/AR** |
ALS3 |
18q21 |
Unknown |
AD |
ALS4 |
9q34 |
SETX |
Juvenile/AD |
ALSS |
15q15 |
SPG11 |
Juvenile/AR |
FUS (ALS6) |
16p11.2 |
FUS |
AD |
ALS7 |
20ptel-p13 |
Unknown |
AD |
ALS8 |
20q13.3 |
VABP |
AD |
ALS9 |
14q11.2 |
Angiogenin (ANG) |
AD |
TARDBP (ALS10) |
1p36.2 |
TAR DNA-binding protein (TARDBP) |
AD |
ALS11 |
6q21 |
FIG4 |
AD |
ALS12 |
10p13 |
OPTN |
AD; AR |
ALS13 |
12q24 |
ATXN2 |
AD |
ALSX |
Xp11 |
UBQLN2 |
X-linked |
C9orf72 (ALS-FTD) |
9q21-22 |
C9ORF72 |
AD |
ALS-FTD |
9p13.3 |
SIGMAR1 |
AD; Juvenile/AR |
PFL1 |
17p13.2 |
Profilin 1 |
AD |
*AD–autosomal dominant; **AR—autosomal recessive |
|||

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Inpatient and Outpatient Care
- Pharmacologic Treatment
- Treatment of Symptoms
- Ventilatory Support
- Dietary Considerations
- Activity Restriction
- Alternative Therapies
- Informing Patients of the Diagnosis
- Patient Support and Advice
- Consultations
- Long-Term Monitoring
- Prevention
- Show All
- Guidelines
- Medication
- Questions & Answers
- Media Gallery
- Tables
- References






