Background
Ependymomas are neoplasms of ependymal cells that occur throughout the entire neuraxis in association with the lining of the cerebral ventricles and central canal of the spinal cord.
Pathophysiology
Ependymomas occur most commonly in the intracranial and intraspinal areas, with lesions rarely occurring in the sacral area. Other unusual ectopic sites of ependymoma are the mediastinum, ovary, and broad ligament. In general, the anatomic location determines the pathophysiological manifestations of the tumor. Supratentorial tumors present with mass effect, focal neurological signs, and occasional obstruction of ventricular outflow. The relationship with the ventricular system is more apparent in tumors of the posterior fossa (mostly of the fourth ventricle), which usually present with obstructive hydrocephalus with or without signs of brain stem compression. See the images below.
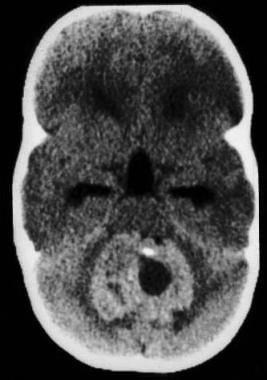 CT scan without contrast, axial view, demonstrates mixed but predominantly hyperdense tumor in the posterior fossa with severe obstructive hydrocephalus.
CT scan without contrast, axial view, demonstrates mixed but predominantly hyperdense tumor in the posterior fossa with severe obstructive hydrocephalus.
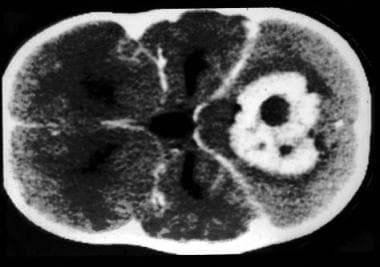 CT scan with contrast, axial view shows moderately intense contrast enhancement (compare with the previous image).
CT scan with contrast, axial view shows moderately intense contrast enhancement (compare with the previous image).
Epidemiology
Frequency
United States
Ependymomas are infrequent tumors, representing 2-8% of all brain tumors. However, ependymomas are the third most common brain tumor in children (8-12%) with up to 30% occurring in children younger than 3 years. Half of the ependymomas occur in the first 2 decades of life; two-thirds are located in the posterior fossa (>90% are in the fourth ventricle). Interestingly, despite their overall low frequency, ependymomas are the most frequent neuroepithelial tumors of the spinal cord.
Mortality/Morbidity
From the biological perspective, ependymomas do not usually proliferate rapidly, are not invasive, and usually do not metastasize. [1] The associated morbidity can mainly be accounted for by the local space-occupying effects of the tumor. However, children and adolescents, the oldest adult age group, cases diagnosed with anaplastic ependymoma, and/or tumor location in a brainstem site had lowest survival rates. [1] In unusual cases, the risk of sudden death from large intracranial ependymomas results from increased intracranial pressure secondary to obstructive hydrocephalus.
Race
No race predilection is reported.
Sex
No sex predilection is reported.
Age
Peak age at presentation ranges from 7 weeks to 16 years with a mean of 3.7 years. A second, lower peak age of presentation occurs in the third decade of life.
-
CT scan without contrast, axial view, demonstrates mixed but predominantly hyperdense tumor in the posterior fossa with severe obstructive hydrocephalus.
-
CT scan with contrast, axial view shows moderately intense contrast enhancement (compare with the previous image).
-
MRI, T2-weighted image, axial view, showing mixed (isodensity and hyperdensity) heterogenous nature of the tumor with some peritumoral edema.
-
MRI, T1-weighted image, without contrast, sagittal view, showing the posterior fossa location, mixed (hypodensity and isodensity) signal intensity and tending to grow out of the fourth ventricle.









