Background
Thrombosis of the venous channels in the brain is an uncommon cause of cerebral infarction relative to arterial disease, but it is an important consideration because of its potential morbidity. (See Prognosis.)
Knowledge of the anatomy of the venous system is essential in evaluating patients with cerebral venous thrombosis (CVT), since symptoms associated with the condition are related to the area of thrombosis. For example, cerebral infarction may occur with cortical vein or sagittal sinus thrombosis secondary to tissue congestion with obstruction. (See Presentation.)
Lateral sinus thrombosis may be associated with headache and a pseudotumor cerebri–like picture. Extension into the jugular bulb may cause jugular foramen syndrome, while cranial nerve palsies may be seen in cavernous sinus thrombosis as a compressive phenomenon. Cerebral hemorrhage also may be a presenting feature in patients with venous sinus thrombosis. (See Presentation.)
Imaging procedures have led to easier recognition of venous sinus thrombosis (see the images below), offering the opportunity for early therapeutic measures. (See Workup.)
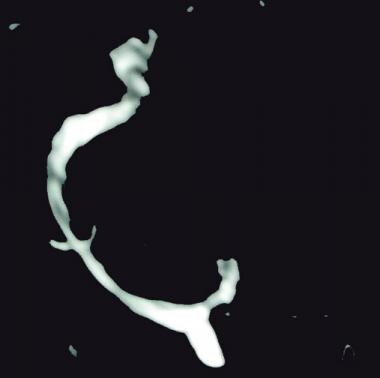 Left lateral sinus thrombosis demonstrated on magnetic resonance venography (MRV). This 42-year-old woman presented with sudden onset of headache. Physical examination revealed no neurologic abnormalities.
Left lateral sinus thrombosis demonstrated on magnetic resonance venography (MRV). This 42-year-old woman presented with sudden onset of headache. Physical examination revealed no neurologic abnormalities.
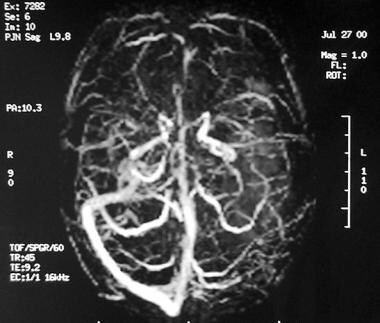 Axial view of magnetic resonance (MR) venogram demonstrating lack of flow in transverse sinus.
Axial view of magnetic resonance (MR) venogram demonstrating lack of flow in transverse sinus.
The following guidelines for CVT have been provided by the American Heart Association and the American Stroke Association [1] :
-
In patients with suspected CVT, routine blood studies consisting of a complete blood count, chemistry panel, prothrombin time, and activated partial thromboplastin time should be performed.
-
Screening for potential prothrombotic conditions that may predispose a person to CVT (eg, use of contraceptives, underlying inflammatory disease, infectious process) is recommended in the initial clinical assessment.
-
Testing for prothrombotic conditions (including protein C, protein S, or antithrombin deficiency), antiphospholipid syndrome, prothrombin G20210A mutation, and factor V Leiden can be beneficial for the management of patients with CVT. Testing for protein C, protein S, and antithrombin deficiency is generally indicated 2-4 weeks after completion of anticoagulation. There is a very limited value of testing in the acute setting or in patients taking warfarin.
-
In patients with provoked CVT (associated with a transient risk factor), vitamin K antagonists may be continued for 3-6 months, with a target international normalized ratio of 2.0-3.0.
-
In patients with unprovoked CVT, vitamin K antagonists may be continued for 6-12 months, with a target international normalized ratio of 2.0-3.0.
-
For patients with recurrent CVT, venous thromboembolism (VTE) after CVT, or first CVT with severe thrombophilia (ie, homozygous prothrombin G20210A; homozygous factor V Leiden; deficiencies of protein C, protein S, or antithrombin; combined thrombophilia defects; or antiphospholipid syndrome), indefinite anticoagulation may be considered, with a target international normalized ratio of 2.0-3.0.
-
For women with CVT during pregnancy, low-molecular-weight heparin (LMWH) in full anticoagulant doses should be continued throughout pregnancy, and LMWH or vitamin K antagonist with a target international normalized ratio of 2.0-3.0 should be continued for ≥6 weeks postpartum (for a total minimum duration of therapy of 6 months).
-
It is reasonable to advise women with a history of CVT that future pregnancy is not contraindicated. Further investigations regarding the underlying cause and a formal consultation with a hematologist or maternal fetal medicine specialist are reasonable.
-
It is reasonable to treat acute CVT during pregnancy with full-dose LMWH rather than unfractionated heparin.
-
For women with a history of CVT, prophylaxis with LMWH during future pregnancies and the postpartum period is reasonable.
Etiology
Many causative conditions have been described in cerebral venous thrombosis (CVT). These may be seen alone or in combination. For example, a prothrombin gene mutation in association with oral contraceptive use raises the odds ratio for developing CVT.
Sinusitis
Infection may occur by extension from the paranasal sinuses. These cases also may be associated with subdural empyema. Bacterial meningitis as a coexistent condition should be considered in these cases. Frontal sinuses are the most common source of infection, with spread through the emissary veins between the posterior sinus mucosa and the meninges. Rarely, sphenoid sinusitis may be associated with cavernous sinus thrombosis. Multiple organisms are to be considered, Staphylococcus aureus being the most common. In chronic infections, gram-negative organisms and fungi such as Aspergillus species may be found.
Trauma and surgery
Trauma may also be an etiologic event. Cerebral sinus thrombosis easily may be overlooked in cases of minor head trauma. Neurosurgical procedures such as dural taps and infusions into the internal jugular vein have been implicated as well.
Hypercoagulable states
Many medical conditions have been associated with CVT. For example, hypercoagulable states associated with the antiphospholipid syndrome, protein S and C deficiencies, antithrombin III deficiency, lupus anticoagulant, and the Leiden factor V mutation may result in CVT. Antibodies against the fibrinolytic receptor, annexin A2 (titer >3 standard deviations), are significantly associated with CVT. [2] Pregnancy also is associated with a hypercoagulable tendency. Malignancies may be associated with hypercoagulable states as well, and therefore may be risk factors.
Intracranial hypotension
Isolated cortical venous thrombosis has been associated with intracranial hypotension syndrome, but only rarely. In a study, Schievink and Maya found that CVT was present in only 3 (2.1%) out of 141 patients with spontaneous intracranial hypotension. [3]
Lumbar puncture
A few cases of CVT have been reported after lumbar puncture (LP), suggesting a causal association. In a study by Canhao et al, LP induced a sustained decrease in mean blood flow velocity (BFV) in the straight sinus (SS), suggesting that the decrease in venous blood flow is a possible mechanism contributing to the occurrence of CVT. In the study, the investigators used transcranial Doppler ultrasonography to register the mean BFV of the SS before, during, and after LP. LP induced a decrease of 47% in mean BFV in the SS, with the mean decrease being significant immediately at the end, 30 min after, and more than 6 hours after LP. [4]
Medications
Several medications are reported to increase the risk of CVT, including the following:
-
Oral contraceptives - Including the third-generation formulations
-
Corticosteroids
-
Epsilon-aminocaproic acid
-
Thalidomide
-
Tamoxifen
-
Erythropoietin
-
Phytoestrogens
-
L-asparaginase
-
Heparin - Heparin therapy has been reported to produce thrombotic thrombocytopenia with associated venous sinus thrombosis
Additional disease risk factors
Other diseases that have been described as risk factors for CVT include the following:
-
Inflammatory bowel diseases, such as Crohn disease and ulcerative colitis, are described as risk factors for venous thrombosis [5] ; corticosteroids used in treatment of these conditions may play a causative role
-
Pregnancy and puerperium are important considerations in women of childbearing age
-
Hematologic conditions, including paroxysmal nocturnal hemoglobinuria, thrombotic thrombocytopenic purpura, sickle cell disease, and polycythemia, are to be considered
-
Collagen-vascular diseases, such as systemic lupus erythematosus, Wegener granulomatosis, and Behçet syndrome, have been reported to be associated with CVT
-
Hyperhomocysteinemia is a strong and independent risk factor for CVT, being present in 27-43% of patients with CVT but in only 8-10% of the general population; whether treatment with folate, pyridoxine, and/or cobalamin reduces the risk of CVT is unclear
-
Dehydration
-
Spontaneous intracranial hypotension
-
High altitude
-
Hepatic cirrhosis
Epidemiology
International occurrence
The incidence of cerebral venous thrombosis (CVT) is difficult to determine, but generally, it is believed to be an uncommon cause of stroke, with the reported ratio of venous to arterial strokes being 1:62.5. In 1973, Towbin reported CVT in 9% of 182 autopsies, [6] while in 1995, Daif reported a frequency in Saudi Arabia of 7 cases per 100,000 hospital patients. [7]
However, with the advent of newer imaging techniques, the reported incidence of CVT is likely to increase as less severe cases are found.
Sex- and age-related demographics
CVT is believed to be more common in women than in men. In a series of 110 cases, Ameri and Bousser found a female-to-male ratio of 1.29:1. [8]
In 1992, Ameri and Bousser reported a uniform age distribution in men with CVT, while 61% of women with CVT were aged 20-35 years. [8] This difference may be related to pregnancy or the use of oral contraceptives. [9]
Prognosis
Smith demonstrated the efficacy of anticoagulant and thrombolytic therapy in patients with cerebral venous thrombosis (CVT). In his study, he compared outcomes of patients who were treated with heparin and local infusion of urokinase (12 patients) with those of patients who received no treatment (21 patients). [10] The results appear in the Table, below.
Table. Patients With Cerebral Venous Thrombosis Treated With Heparin and Local Infusion of Urokinase vs Nontreated Group (Open Table in a new window)
|
Treated Group, % (n = 12) |
Nontreated Group, % (n = 21) |
Full recovery |
62.5 |
29 |
Mild disability |
12.5 |
13 |
Severe disability |
12.5 |
9.6 |
Fatal outcome |
12.5 |
48 |
Morbidity and mortality
Herniation attributable to unilateral mass effect is the major cause of death in CVT. In CVT patients with large parenchymal lesions causing herniation, decompressive surgery has been lifesaving and often results in good functional outcome, even in patients with severe clinical conditions. [11]
Mortality in untreated cases of venous thrombosis has been reported to range from 13.8-48%; this high mortality rate may be a reflection of clinical severity at entrance into the study. Between 25% and 30% of patients have full recovery.
In a Portuguese study that prospectively analyzed 91 patients with CVT over a mean 1-year follow-up interval, the majority of patients experienced complete recovery. [12] Of the patients analyzed, 7% died in the acute phase, 1% died during the one year follow-up, 82% recovered completely, and 1% were dependent; 59% developed thrombotic events during the follow-up, 10% had seizures, 11% complained of severe headaches, and 1 patient experienced severe visual loss.
In 2003, Buccino et al found a good overall outcome in their reinvestigation of a series of 34 patients with confirmed CVT. [13] However, 10 patients (30%) had episodic headaches, 3 patients (8.8%) had seizures, 4 patients (11.7%) had pyramidal signs, and 2 (5.9%) had visual deficits. Mild nonfluent aphasia was seen in 3 patients. Working memory deficit and depression of mood were seen in 6 patients (17.6%).
-
Left lateral sinus thrombosis demonstrated on magnetic resonance venography (MRV). This 42-year-old woman presented with sudden onset of headache. Physical examination revealed no neurologic abnormalities.
-
Same patient as in the previous image. One week after treatment with heparin, the magnetic resonance (MR) venogram displayed increased flow in the left lateral sinus consistent with early recanalization of the sinus; headache had resolved at this point.
-
Magnetic resonance venogram (MRV) - axial view; A = lateral (transverse) sinus; B = sigmoid sinus; C = confluence of sinuses; and D = superior sagittal sinus.
-
Magnetic resonance venogram (MRV) - sagittal view; A = lateral (transverse) sinus; C = confluence of sinuses; D = superior sagittal sinus; and E = straight sinus.
-
Computed tomography (CT) scan demonstrates a left posterior temporal hematoma in a 38-year-old woman on oral contraceptives (the only identified risk factor).
-
Contrast-enhanced magnetic resonance imaging (MRI) scan showing lack of filling of left transverse sinus.
-
Axial view of magnetic resonance (MR) venogram demonstrating lack of flow in transverse sinus.
-
Coronal view of magnetic resonance (MR) venogram demonstrating lack of flow in the left transverse and sigmoid sinuses.
Tables
|
Treated Group, % (n = 12) |
Nontreated Group, % (n = 21) |
Full recovery |
62.5 |
29 |
Mild disability |
12.5 |
13 |
Severe disability |
12.5 |
9.6 |
Fatal outcome |
12.5 |
48 |







