Background
Viral meningitis is inflammation of the leptomeninges as a manifestation of central nervous system (CNS) infection. Viral names the causative agent, and the term meningitis implies lack of parenchymal and spinal cord involvement (otherwise called encephalitis and myelitis, respectively). Viral meningitis is also often referred to as aseptic meningitis.
In uncomplicated viral meningitis, the clinical course is usually self-limited, with complete recovery in 7-10 days. However, when the viral pathogen causes a more involved meningoencephalitis or meningomyelitis, the course can be significantly more protracted. A magnetic resonance imaging (MRI) scan of a patient with meningoencephalitis is seen below.
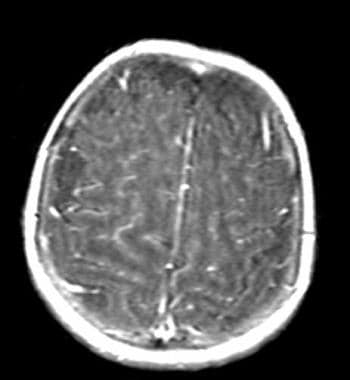 T1-weighted MRI of brain demonstrates diffuse enhancement of the meninges in viral meningoencephalitis.
T1-weighted MRI of brain demonstrates diffuse enhancement of the meninges in viral meningoencephalitis.
Currently, more than 85% of viral meningitis cases are caused by nonpolio enteroviruses. Disease characteristics, clinical manifestations, and epidemiology generally mimic those of enteroviral infections.
Mumps, polio, and lymphocytic choriomeningitis viruses (LCMVs) are now rare offenders in developed countries. However, polio remains a major cause of debilitating myelitis in some regions of the world.
As discussed below, many viruses are capable of causing meningitis. This discussion attempts to simplify the microbiology of each viral family with emphasis on disease manifestations and risk factors. Note that in as many as one third of cases, no causative agents are identified. This number is improving with new testing methodologies.
Enteroviruses
Enteroviruses account for more than 85% of all cases of viral meningitis. They are part of the viral family Picornaviridae ("pico" for small, "rna" for ribonucleic acid) and include echoviruses, coxsackieviruses A and B, polioviruses, and the numbered enteroviruses. Nonpolio enteroviruses are common viruses; they are nearly as prevalent as rhinoviruses (which cause the common cold). [1]
The overwhelming majority of meningitis cases are caused by serotypes of coxsackievirus and echovirus. Coxsackievirus B subgroups alone account for more than 60% of meningitis cases in children younger than age 3 months.
Enteroviruses enter the human host usually via the oral-fecal route, but can also spread through the respiratory route.
Enteroviruses are ubiquitous in the summer and early fall; their propensity to cause infection during the warmer months is the major factor in the higher incidence of aseptic meningitis during that time.
The associated clinical findings in enteroviral infections may include pharyngitis, pleurodynia, rash, and pericarditis.
Expectant mothers infected with coxsackievirus B may remain minimally symptomatic, but their infants can acquire the infection perinatally and develop a potential fatal illness, with the infection targeted mainly toward the heart.
Enteroviruses 70 and 71, which exhibit strong neurotropism, are associated with meningoencephalitis, poliolike paralytic syndromes, and Guillain-Barre syndrome, as well as aseptic meningitis.
Arboviruses
Arboviruses account for about 5% of cases in North America.
Arboviruses consist of more than 500 viruses from different viral families, all given the common name "ar-bo," for arthropod-borne disease. Blood-sucking arthropods, usually mosquitoes, serve as vectors for transmission.
Because exposure to mosquitoes or ticks is the risk factor for transmission, the number of infections is highest in summer and early fall, in concordance with high mosquito populations.
Some of the important arboviruses include the eastern and western equine encephalitis viruses, from the Togavirus family; St. Louis encephalitis’ West Nile, Japanese B, and Murray Valley viruses, from the Flavivirus family; and California group and Jamestown Canyon viruses, from the Bunyaviridae family. Colorado tick fever is caused by a coltivirus in the western regions of the United States.
The most common clinical manifestation is meningoencephalitis rather than pure meningitis.
Seizures are more common with arboviral meningitis than with any other group of viruses.
Some agents preferentially infect certain age groups, such as St. Louis encephalitis, which affects the extremes of age, and California virus, which infects young children. Children with St. Louis or California group encephalitis viruses may not exhibit any neurologic signs or altered mental status.
St. Louis encephalitis (SLE) virus is the most common cause of arboviral meningitis, and is also the most common mosquito-transmitted disease in the United States. Internationally, Japanese B virus is the biggest offender in this group.
Of the arboviruses, West Nile virus caused much attention, as it was first recognized in the United States only in 1999 and quickly became an epidemic in 2002, with more than 4,000 reported cases. In 2008, 1,356 cases were reported. [2]
Infection with the West Nile virus is usually asymptomatic or manifests as mild symptoms of nonspecific fever, myalgia, and fatigue. However, 1 in 150 cases develop into severe disease involving the nervous system, with encephalitis reported more than meningitis. In 2008, 687 cases of West Nile neuroinvasive disease were reported to the US Centers for Disease Control and Prevention (CDC) from all across the United States. [2]
Neuroinvasive West Nile disease occurs more often in elderly persons.
Mumps
A member of the Paramyxovirus family, mumps virus was one of the first known causative agents of meningitis and meningoencephalitis. [3]
The incidence of mumps in the vaccination era has decreased significantly to 1 per 100,000 population in the United States.
Nonetheless, outbreaks have occurred in vaccinated populations, including a large epidemic in the United Kingdom that peaked in 2005 and several outbreaks in the American Midwest in 2006. [4, 18] In addition, mumps continues to cause 10-20% of meningitis and meningoencephalitis cases in parts of the world where vaccines are not readily accessible.
Males 16-21 years of age are at highest risk for developing this infection, with a 3:1 male/female ratio.
Clusters of cases occur in schools and colleges in the winter months.
Concomitant parotitis is a helpful clinical tool, but it may be absent in as many as half of cases with CNS involvement.
A cohort study of 12,000 unvaccinated children from northern Finland revealed that mumps meningoencephalitis accounted for 40.9% of all viral CNS infections. Mumps also remains an important cause of aseptic meningitis in England and Japan. [15]
In 2003, epidemics of aseptic meningitis following measles, mumps, rubella (MMR) vaccination campaigns in various nations (including Brazil and the UK) prompted the Global Advisory Committee on Vaccine Safety to conduct a review of vaccine-derived mumps meningitis. [5] At the time, the committee stated that certain strains of the mumps vaccine (Urabe, Leningrad-Zagreb, and Leningrad-3 strains) were associated with higher incidences of postvaccination aseptic meningitis.
In 2006, the committee determined that the international literature reviewed was actually inconclusive and that further studies were needed. [6] Even so, replacement mumps components were developed and vaccines were reformulated worldwide.
Herpes family viruses
Herpes simplex virus (HSV)-1, HSV-2, varicella-zoster virus (VZV), Ebstein-Barr virus (EBV), cytomegalovirus (CMV), and human herpesvirus-6 collectively cause approximately 4% of cases of viral meningitis, with HSV-2 being the most common offender. The viruses may attack at any time of the year.
Meningitis caused by these viruses is often self-limited. When associated with encephalitis, however, the mortality rate can be high. Early treatment with acyclovir can significantly reduce morbidity.
HSV-1 remains the most common cause of sporadic encephalitis, while HSV-2 infections of CNS mostly are restricted to aseptic meningitis.
HSV-2 genital infection may precede meningitis; sexual contact with actively infected individuals is one of the known risk factors.
In one review, however, only 3 of 23 patients with HSV-2 meningitis had a history of prior genital herpes or had genital lesions noted at the time of presentation. [7] Maternal-fetal transmission of HSV-2 can occur, leading to significant systemic sequelae, including infantile septicemia and death.
EBV, HSV-1, and especially HSV-2 have been associated with Mollaret meningitis, a rare, benign, recurrent meningitis that resolves spontaneously. Mollaret cells (activated monocytes with an atypical appearance of enlarged, bilobed nuclei and amorphous cytoplasm) are found in the CSF usually on the first day of symptoms. Herpesvirus-6, EBV, and the human immunodeficiency virus (HIV; which is not a member of the herpes family) have also been implicated. These viruses are all known to remain latent within the nervous system.
CMV infections occur mostly in immunocompromised hosts. CMV may cause subacute encephalitis in patients with AIDS. Congenital CMV, which is a much more serious form of infection, has significant associated morbidity and mortality.
Childhood or adult chickenpox infections by VZV rarely are complicated by meningitis. Adult zoster involving any dermatome may lead to meningitis or meningoencephalitis.
Lymphocytic choriomeningitis virus
LCMV belongs to the family of arenaviruses. Now a rare cause of meningitis, the virus is transmitted to humans by contact with rodents (eg, hamster, rats, mice) or their excreta. Persons at highest risk of infection are laboratory workers, pet owners, or persons living in nonhygienic areas.
Adenovirus
Adenovirus is a rare cause of meningitis in immunocompetent individuals but a major cause in patients with acquired immunodeficiency syndrome (AIDS). The infection may occur simultaneously with an upper respiratory infection.
Measles
This Morbillivirus is another cause of meningitis that has become rare. The characteristic maculopapular rash aids in the diagnosis. Most cases occur in younger people in schools and colleges. Still a worldwide health threat, measles has the highest attack rate of any infection.
From January 1 through April 24, 2015, the United States experienced 5 outbreaks, with 166 cases reported. [19] Preliminary investigations of a large multistate outbreak that originated in California revealed 45% of the infected were unvaccinated, and 43% had unknown vaccination status. [19]
Eradication of measles is an important goal of the World Health Organization (WHO).
HIV
HIV may be a cause of atypical meningitis characterized by chronicity and recurrence. About the time of seroconversion, patients may present with CSF pleocytosis, elevated protein level and, occasionally, high intracranial pressure.
Reports have suggested that as many as 5-10% of HIV infections can be heralded by meningitis. Aside from the usual meningeal signs, HIV infections may also cause global encephalopathy, seizures, and focal neurologic deficits. Some patients develop chronically abnormal CSF findings with mild or no symptoms. HIV often can be isolated from the CSF.
Nonviral causes of meningitis
Tuberculous, fungal, and mycoplasmal organisms are among the important nonviral causes of aseptic meningitis and should be suspected in the appropriate clinical setting.
For example, Lyme borreliosis causes a significant number of cases of aseptic meningitis in the Northeast and Mid-Atlantic states. The diagnosis is suggested by the history of tick bite or outdoor activity in these areas of endemic disease, and the presence of erythema chronicum migrans at the site of tick bite is pathognomonic. Lyme meningitis has a predilection to cause focal cranial nerve palsies, with the seventh nerve most commonly affected.
Clinicians must consider partially-treated bacterial meningitis as a possible etiology for the aseptic nature of their patient's disease; for example, patients with bacterial otitis and sinusitis who have been taking antibiotics may present with meningitis and CSF findings identical to those of viral meningitis.
The clinician should also realize that the picture of aseptic meningitis is created not only by infectious agents, but also by chemical irritation (chemical meningitis), neoplasm (meningitis carcinomatous), granulomatous disorders, and other inflammatory conditions. This discussion, however, focuses on meningitis caused by viral agents.
Pathophysiology
Some controversy exists as to the long-term effects of viral meningitis on children, with some studies attributing learning disabilities, neuromuscular impairments (ie, mild paresis or loss of coordination), and deafness to viral meningitis. Investigators believe that most of these cases must involve the CNS parenchyma, causing encephalitis or encephalomyelitis.
Communicating hydrocephalus is a rare complication of viral meningitis and is due to obstruction of arachnoid granulations by inflammatory debris. The usual time of onset is within weeks of the original symptoms. Less common is acute hydrocephalus, with onset within hours to days of the original symptoms.
Etiology
Viral pathogens may gain access to the CNS via either of 2 main routes: hematogenous and neural. The hematogenous route is more common for penetration of most known viral pathogens. Neural penetration refers to spread along nerve roots and is usually limited to herpes viruses (HSV-1, HSV-2, VZV B) and possibly some enteroviruses.
Multiple host defenses prevent viral inoculum from causing clinically significant infection. These include local and systemic immune responses, skin and mucosal barriers, and the blood-brain barrier (BBB).
The virus replicates in the initial organ system (ie, respiratory or gastrointestinal mucosa) and gains access to the bloodstream. Primary viremia introduces the virus to the reticuloendothelial organs (liver, spleen, lymph nodes). If the replication persists despite immunologic defenses, secondary viremia occurs, which is thought to be responsible for seeding of the CNS. Rapid viral replication likely plays a major role in overcoming the host defenses.
The actual mechanism of viral penetration into the CNS is not well understood. The virus may cross the BBB directly at the capillary endothelial level or through natural defects, such as the area postrema and other sites that lack a BBB.
The inflammatory response is seen in the form of pleocytosis; polymorphonuclear leukocytes (PMNs) lead the differential cell count in the first 24-48 hours, followed later by increasing numbers of monocytes and lymphocytes. The CSF lymphocytes have been recognized as T cells, although B cell immunity is also important in defending against some viruses.
Evidence exists that some viruses gain access to the CNS by retrograde transport along nerve roots. For example, the likely pathway for HSV-1 encephalitis is via the olfactory or trigeminal nerve roots, with the virus being transported by the olfactory fibers to the basal frontal and anterior temporal lobes.
Examples of modes of transmission in viral meningitis include the following (see Background):
-
Enteroviruses - Usually through the oral-fecal route, but also sometimes through the respiratory route
-
Arboviruses - Via blood-sucking arthropods, usually mosquitoes
-
Lymphocytic choriomeningitis virus - Through contact with rodents (eg, hamster, rats, mice) or their excreta
Epidemiology
Incidence of viral meningitis in the United States
More than 10,000 cases of viral meningitis are reported annually, but the actual incidence may be as high as 75,000. Lack of reporting is due to the uneventful clinical outcome of most cases and the inability of some viral agents to grow in culture.
According to reports from the Centers for Disease Control and Prevention (CDC), inpatient hospitalizations resulting from viral meningitis range from 25,000-50,000 each year. An incidence of 11 per 100,000 population per year has been estimated in some reports.
International incidence of viral meningitis
Obtaining accurate international prevalence and incidence of this clinically heterogenous and often benign disease is difficult. Worldwide causes of viral meningitis include enteroviruses, mumps virus, measles virus, VZV, and HIV. Meningitis symptoms may develop in as few as 1 in 3,000 cases of infection by these agents.
Mumps causes 10-20% of meningitis and meningoencephalitis cases in parts of the world where vaccines are not readily accessible.
Japanese B encephalitis virus, the most common pathogen in epidemic viral meningitis worldwide, accounts for more than 35,000 infections annually throughout Asia but is estimated to cause 200-300 times that number of subclinical infections.
Viral meningitis is a notifiable disease in England and Wales, but many cases go unreported. [16] This is also true in Ireland. [17]
Age predilection
The incidence of viral meningitis drops with age, with the incidence during the first year of life being 20 times greater than it is in older children and adults.
Studies from Finland have estimated the incidence of viral meningitis to be 19 per 100,000 population in children aged 1-4 years. This is in significant contrast to 219 cases per 100,000 population estimated for children younger than age 1 year. [15]
Most arboviruses have diverse attack characteristics that affect both sexes, but at different ages. Some agents preferentially infect certain age groups, such as St. Louis encephalitis, which affects the extremes of age, and California virus, which infects young children.
In neonates older than 7 days, enteroviruses are the most common cause of aseptic meningitis. Vaccination has greatly reduced the incidence of meningitis from mumps, polio, and measles viruses.
Some of the arboviruses strike at the extremes of age, with the elderly at greater risk of infection, while mumps and measles peak in the later teenage years.
Males 16-21 years of age are at highest risk of developing mumps. Clusters of cases occur in schools and colleges in the winter months.
Most cases of measles occur in younger people in schools and colleges.
Sex predilection
Depending on the type of viral pathogen, the ratio of affected males to females can vary. Enteroviruses are thought to affect males 1.3-1.5 times more often than females. Mumps virus is known to affect males 3 times more often than females.
Morbidity and mortality in viral meningitis
Long-term neurologic sequelae from uncomplicated viral meningitis are rare. Sequelae in children (especially infants and young children), as reported in the literature, include the following:
-
Seizure disorders
-
Hydrocephalus
-
Sensorineural hearing loss
-
Weakness
-
Paralysis
-
Cranial nerve palsy
-
Learning disabilities
-
Blindness
-
Behavior disorders
-
Speech delay
Physicians must realize that viruses capable of causing meningitis can also cause more serious infections of the CNS and other organs. Complications, such as brain edema, hydrocephalus, and seizures, can occur in the acute period.
WHO statistical reports from 1997 reported enteroviral meningitis with sepsis as the fifth most frequent cause of neonatal mortality.
Excluding the neonatal period, the mortality rate associated with viral meningitis is less than 1%; the morbidity rate is also low.
Prognosis
The prognosis for viral meningitis is usually excellent, with most cases resolving in 7-10 days. Implicit in the diagnosis is the self-limited nature of this disease. The exception falls with the neonatal patients, in whom viral meningitis can be fatal or associated with significant morbidity.
Concomitant encephalitis adds significant potential for adverse outcomes. Concurrent systemic manifestations, such as pericarditis and hepatitis, are other indicators of poor prognosis.
Patient Education
Pregnant women should avoid exposure to rodents, rats, and house mice, which carry LCMV. Some investigators even suggest avoidance of young children and public pools by pregnant women in the third trimester, in order to decrease the risk of enteroviral colonization and transmission to the fetus. Infected pets also pose a risk to pregnant women.
Neonates should be kept away from exposure to mosquitoes, for the prevention of arboviral infection.
Vaccination remains the most potent means of combating infections by polio, measles, mumps, and varicella viruses.
Strict handwashing is effective in controlling the spread of enterovirus-related infections, but maintaining public hygiene remains a problem in some developing countries.
The education of sex partners about the use of barrier devices can significantly decrease the incidence of HSV-2 infections.
Protection against mosquito exposure (using insect sprays, netting, and eradication of breeding sites) should be exercised to prevent arbovirus infection and is especially important in vulnerable patients, such as the young.
Avoidance of exposure to rodents can decrease the incidence of LCMV meningoencephalitis. Infected pets, house mice, and rats pose a risk to pregnant women.
For patient education information, visit eMedicineHealth's Brain and Nervous System Center and Children's Health Center. Also, see eMedicineHealth's patient education articles Meningitis in Adults, Meningitis in Children, Encephalitis, and Ticks.
-
T1-weighted MRI of brain demonstrates diffuse enhancement of the meninges in viral meningoencephalitis.
-
This rash consists of an enlarging annular plaque. Image courtesy of Lyme Disease Network (http://www.lymenet.org/).








