Practice Essentials
Graves disease is an autoimmune disorder characterized by hyperthyroidism due to circulating autoantibodies. Thyroid-stimulating immunoglobulins (TSIs) bind to and activate thyroid-stimulating hormone (TSH) receptors, causing the thyroid gland to grow and the thyroid follicles to increase synthesis of thyroid hormone. Graves disease, along with Hashimoto thyroiditis, is classified as an autoimmune thyroid disorder. Ultrasensitive (third-generation) TSH assays remain the best screening test for thyroid disorders. Treatment involves alleviation of symptoms and correction of the thyrotoxic state. Graves disease is named after Robert J. Graves, MD, [1] who described the condition in 1835.
In some patients, Graves disease represents a part of more extensive autoimmune processes leading to dysfunction of multiple organs (eg, polyglandular autoimmune syndromes). Graves disease is associated with pernicious anemia, vitiligo, diabetes mellitus type 1, autoimmune adrenal insufficiency, systemic sclerosis, myasthenia gravis, Sjögren syndrome, rheumatoid arthritis, and systemic lupus erythematosus. [2] Moreover, advances in cancer immunotherapy with immune checkpoint inhibitors (anti–CTLA-4, anti–PD-1, and anti–PD-L1 antibodies) have led to immune-related adverse effects, including problems affecting the thyroid glands (ie, thyroiditis [typically with a transient hyperthyroid phase followed by a permanent hypothyroid phase] and Graves disease). [3]
Graves ophthalmopathy (also known as Graves orbitopathy) is shown below.

Signs and symptoms of Graves disease
Common physical findings in Graves disease, organized by anatomic region, are as follows:
-
General - Increased basal metabolic rate, weight loss despite increase in or similar appetite
-
Skin - Warm, most, fine skin; increased sweating; fine hair; vitiligo; alopecia; pretibial myxedema
-
Head, eyes, ears, nose, and throat - Chemosis, conjunctival irritation, widening of the palpebral fissures, lid lag, lid retraction, proptosis, impairment of extraocular motion, visual loss in severe optic nerve involvement, periorbital edema
-
Neck - Upon careful examination, the thyroid gland generally is diffusely enlarged and smooth; a well-delineated pyramidal lobe may be appreciated upon careful palpation; thyroid bruits and, rarely, thrills may be appreciated; thyroid nodules may be palpable.
-
Chest - Gynecomastia, tachypnea; tachycardia; murmur; hyperdynamic precordium; S3, S4 heart sounds; ectopic beats; irregular heart rate and rhythm
-
Abdomen - Hyperactive bowel sound
-
Extremities - Edema, acropachy, onycholysis
-
Neurologic - Hand tremor (fine and usually bilateral), hyperactive deep tendon reflexes
-
Musculoskeletal - Kyphosis, lordosis, loss of height, proximal muscle weakness, hypokalemic periodic paralysis in persons of susceptible ethnic groups
-
Psychiatric - Restlessness, anxiety, irritability, insomnia, depression
Workup in Graves disease
Ultrasensitive (third-generation) TSH assays remain the best screening test for thyroid disorders. With the exception of TSH-induced hyperthyroidism, subnormal or suppressed TSH levels are seen in most patients with thyrotoxicosis.
Liver function test results should be obtained to monitor for liver toxicity caused by thioamides (antithyroid medications).
A complete blood count (CBC) with differential should be obtained at baseline and with the development of fever or symptoms of infection. Graves disease may be associated with normocytic anemia, low-normal to slightly depressed total white blood cell (WBC) count with relative lymphocytosis and monocytosis, and low-normal to slightly depressed platelet count. Thioamides may rarely cause severe hematologic side effects, but routine screening for these rare events is not cost-effective.
Radioactive iodine scanning and measurements of iodine uptake are useful in differentiating the causes of hyperthyroidism. In Graves disease, the radioactive iodine uptake is increased, and the uptake is diffusely distributed over the entire gland. [4]
Management of Graves disease
Treatment involves alleviation of symptoms and correction of the thyrotoxic state. Adrenergic hyperfunction is treated with beta-adrenergic blockade. Correcting the high thyroid hormone levels can be achieved with antithyroid medications that block the synthesis of thyroid hormones or by treatment with radioactive iodine.
Radioactive iodine is, in fact, the most commonly used therapy for Graves disease. Indications for radioactive iodine over antithyroid agents include a large thyroid gland, multiple symptoms of thyrotoxicosis, high levels of thyroxine, and high titers of TSI.
Thyroidectomy is not the recommended first-line therapy for hyperthyroid Graves disease in the United States, although it may be appropriate in the presence of a thyroid nodule that is suggestive of carcinoma or in patients less than age 5 years. [5]
Pathophysiology
In Graves disease, B and T lymphocyte-mediated autoimmunity are known to be directed at 4 well-known thyroid antigens: thyroglobulin, thyroid peroxidase, sodium-iodide symporter and the TSH receptor. However, the TSH receptor itself is the primary autoantigen of Graves disease and is responsible for the manifestation of hyperthyroidism. In this disease, the antibody and cell-mediated thyroid antigen-specific immune responses are well defined. Direct proof of an autoimmune disorder that is mediated by autoantibodies is the development of hyperthyroidism in healthy subjects by transferring TSH-receptor antibodies in serum from patients with Graves disease and the passive transfer of TSH-receptor antibodies to the fetus in pregnant women.
The thyroid gland is under continuous stimulation by circulating autoantibodies against the TSH receptor, and pituitary TSH secretion is suppressed because of the increased production of thyroid hormones. The stimulating activity of TSH-receptor antibodies is found mostly in the immunoglobulin G1 subclass. These thyroid-stimulating antibodies cause release of thyroid hormone and thyroglobulin that is mediated by 3,'5'-cyclic adenosine monophosphate (cyclic AMP), and they also stimulate iodine uptake, protein synthesis, and thyroid gland growth.
The anti-sodium-iodide symporter, antithyroglobulin, and antithyroid peroxidase antibodies appear to have little role in the etiology of hyperthyroidism in Graves disease. However, they are markers of autoimmune disease against the thyroid. Intrathyroidal lymphocytic infiltration is the initial histologic abnormality in persons with autoimmune thyroid disease and can be correlated with the titer of thyroid antibodies. Besides being the source of autoantigens, the thyroid cells express molecules that mediate T cell adhesion and complement regulation (Fas and cytokines) that participate and interact with the immune system. In these patients, the proportion of CD4 lymphocytes is lower in the thyroid than in the peripheral blood. The increased Fas expression in intrathyroidal CD4 T lymphocytes may be the cause of CD4 lymphocyte reduction in these individuals.
Viral infection is an environmental factor linked to Graves disease. The prevalence of enteroviral proteins, the upregulation of human leukocyte antigen (HLA) class I expression, and co-localization with antiviral response proteins such as Stat1, VP1, and PKR all indicate an association between Graves disease and viral infection. [6] Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has also been linked to the development of subacute thyroiditis and Graves disease. [7, 8]
Several autoimmune thyroid disease susceptibility genes are considered to be linked to Graves disease, including CD40, CTLA-4, the thyroglobulin gene (TG), the TSH-receptor gene (TSHR), PTPN22, FOXP3, CD25, and VDR. The RNASET2-FGFR1OP-CCR6 region at 6q27 and an intergenic region at 4p14 have also been associated with the disorder. [9, 10, 11, 12, 13, 13] Similarly, in a genome-wide association study of more than 1500 patients with Graves disease and 1500 controls, six susceptibility loci were found to be related to the condition: the major histocompatibility complex (MHC), TSHR, CTLA-4, FCRL3, the RNASET2-FGFR1OP-CCR6 region at 6q27, and the intergenic region at 4p14. [14]
A genetic predisposition to thyroid autoimmunity may interact with environmental factors or events to precipitate the onset of Graves disease. Moreover, TSHR and MHC class II variants were found to be strongly associated with persistently TSH receptor autoantibody (TRAb)–positive Graves disease. [15] In terms of epigenetic regulation, non-coding RNA molecules such as miR-23a-3p and lncRNA MEG3 may participate in the pathophysiology of Graves disease by disrupting Th17/Treg cell balance. [16]
Gut microbiota have been shown to be associated with autoimmune thyroid diseases. [17] Decreases in Bifidobacterium and Lactobacillus may be linked to such disorders, but microbiome data in Graves disease are still limited. [17, 16]
Graves disease patients have a higher rate of peripheral blood mononuclear cell conversion into CD34+ fibrocytes compared with healthy controls. These cells may contribute to the pathophysiology of ophthalmopathy by accumulating in orbital tissues and producing inflammatory cytokines, including tumor necrosis factor alpha (TNF-alpha) and interleukin-6 (IL-6). [18]
The TSH receptor is detectable in orbital tissues, but whether it has a pathogenetic role in Graves ophthalmopathy is unclear. The insulin-like growth factor-1 (IGF1) receptor is overexpressed in orbital fibroblasts, B cells, and T cells of patients with Graves ophthalmopathy, and patients with this eye disorder may have circulating immunoglobulins that bind to IGF1 receptors. Activation of IGF1R will increase hyaluronan synthesis and cytokine release. Using monoclonal antibodies to block IGF1R can reduce the expression levels of TSHR and IGF1R on fibrocytes and antagonize TSH-induced expression of inflammation genes (IL6, IL8, and TNFA).
Pathophysiologic mechanisms are shown in the image below.
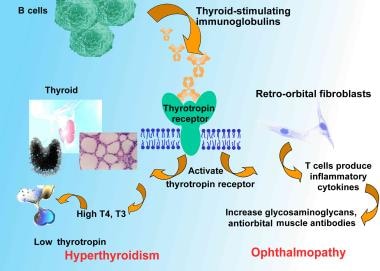 Pathophysiologic mechanisms of Graves disease relating thyroid-stimulating immunoglobulins to hyperthyroidism and ophthalmopathy. T4 is levothyroxine. T3 is triiodothyronine.
Pathophysiologic mechanisms of Graves disease relating thyroid-stimulating immunoglobulins to hyperthyroidism and ophthalmopathy. T4 is levothyroxine. T3 is triiodothyronine.
Epidemiology
Frequency
United States
Graves disease is the most common cause of hyperthyroidism in the United States. A study conducted in Olmstead County, Minnesota estimated the incidence to be approximately 30 cases per 100,000 persons per year. [19] The prevalence of maternal thyrotoxicosis is approximately 1 case per 500 persons, with maternal Graves disease being the most common etiology. Commonly, patients have a family history involving a wide spectrum of autoimmune thyroid diseases, such as Graves disease, Hashimoto thyroiditis, or postpartum thyroiditis, among others.
International
Among the causes of spontaneous thyrotoxicosis, Graves disease is the most common. Graves disease represents 60-90% of all causes of thyrotoxicosis in different regions of the world. In the Wickham Study in the United Kingdom, the incidence was reported to be 100-200 cases per 100,000 population per year. [20] The incidence in women in the UK has been reported to be 80 cases 100,000 per year. [21]
Mortality/Morbidity
If left untreated, Graves disease can cause severe thyrotoxicosis. A life-threatening thyrotoxic crisis (ie, thyroid storm) can occur. Long-standing severe thyrotoxicosis leads to severe weight loss with catabolism of bone and muscle. [22] Cardiac complications and psychocognitive complications can cause significant morbidity. Graves disease is also associated with ophthalmopathy, dermopathy, and acropachy.
Thyroid storm is an exaggerated state of thyrotoxicosis. [23] It occurs in patients who have unrecognized or inadequately treated thyrotoxicosis and a superimposed precipitating event such as thyroid surgery, nonthyroidal surgery, infection, or trauma. When thyroid storm was first described, the acute mortality rate was nearly 100%. In current practice, with aggressive therapy and early recognition of the syndrome, the mortality rate is approximately 20%. [24]
Long-term excess of thyroid hormone can lead to osteoporosis in men and women. The effect can be particularly devastating in women, in whom the disease may compound the bone loss secondary to chronic anovulation or menopause. Bone loss is accelerated in patients with hyperthyroidism. The increase in bone loss can be demonstrated by increased urinary pyridinoline cross-link excretion. Serum calcium and phosphate, plasma FGF-23 were significantly higher in the patients with Graves disease than in healthy control subjects, suggesting that FGF-23 is physiologically related to serum phosphate homeostasis in untreated Graves disease. [25]
Hyperthyroidism increases muscular energy expenditure and muscle protein breakdown. These abnormalities may explain the sarcopenia and myopathy observed in patients with hyperthyroid Graves disease.
Cardiac hypertrophy has been reported in thyrotoxicosis of different etiologies. Rhythm disturbances such as extrasystolic arrhythmia, atrial fibrillation, and flutter are common. Cardiomyopathy and congestive heart failure can occur. [26]
Psychiatric manifestations such as mood and anxiety disorders are common. [27] Subjective cognitive dysfunction is often reported by Graves disease patients and may be due to affective and somatic manifestations of thyrotoxicosis, which remit after treatment of Graves thyrotoxicosis. [28]
A study by Folkestad et al reported Graves disease and toxic nodular goiter to be a risk factors for dementia. The investigators found that every 6 months of reduced TSH was linked to a 16% rise in dementia risk in hyperthyroid individuals. [29]
Nonpitting edema is the most prevalent form of dermopathy (about 40%) and are primarily in the pretibial area. The nearly all (>95%) patients with dermopathy had ophthalmopathy. [30] Advanced forms of dermopathy are elephantiasis or thyroid acropachy. Severe acropachy can be disabling and can lead to total loss of hand function.
Progression of ophthalmopathy can lead to compromised vision and blindness. Visual loss due to corneal lesions or optic nerve compression can be seen in severe Graves ophthalmopathy.
In a study of 1128 patients with Graves ophthalmopathy, Kim et al found the prevalence of ocular hypertension (OHT) to be 6.8% and the prevalence of open-angle glaucoma (OAG) to be 1.6%. The prevalences were higher in patients over age 40 years, being 9.5% and 3.4%, respectively. The investigators also reported the prevalence of OHT in Graves ophthalmopathy to be associated with male sex, duration of the ophthalmopathy, a clinical activity score of 3 or above, extraocular muscle involvement, and lid retraction. Male sex and duration of the ophthalmopathy were associated with the prevalence of OAG in Graves ophthalmopathy. [31]
Maternal Graves disease can lead to neonatal hyperthyroidism by transplacental transfer of thyroid-stimulating antibodies. Approximately 1-5% of children of mothers with Graves disease (usually with high TSI titer) are affected. Usually, the TSI titer falls during pregnancy.
Elderly individuals may develop apathetic hyperthyroidism, and the only presenting features may be unexplained weight loss or cardiac symptoms such as atrial fibrillation and congestive heart failure.
Boelaert et al investigated the prevalence of and relative risks for coexisting autoimmune diseases in patients with Graves disease (2791 patients) or Hashimoto thyroiditis (495 patients). The authors found coexisting disorders in 9.7% of patients with Graves disease and in 14.3% of those with Hashimoto thyroiditis, with rheumatoid arthritis being the most common of these (prevalence = 3.15% and 4.24% in Graves disease and Hashimoto thyroiditis, respectively). Relative risks of greater than 10 were found for pernicious anemia, systemic lupus erythematosus, Addison disease, celiac disease, and vitiligo. The authors also reported a tendency for parents of patients with Graves disease or Hashimoto thyroiditis to have a history of hyperthyroidism or hypothyroidism, respectively. [32]
Race
In whites, autoimmune thyroid diseases are, based on linkage analysis, linked with the following loci: AITD1, CTLA4, GD1, GD2, GD3, HT1, and HT2. Different loci have been reported to be linked with autoimmune thyroid diseases in persons of other races.
Susceptibility is influenced by genes in the human leukocyte antigen (HLA) region on chromosome 6 and in CTLA4 on band 2q33. Association with specific HLA haplotypes has been observed and is found to vary with ethnicity.
Sex
As with most autoimmune diseases, susceptibility is increased in females. Hyperthyroidism due to Graves disease has a female-to-male ratio of 7-8:1.
The female-to-male ratio for pretibial myxedema is 3.5:1. Only 7% of patients with localized myxedema have thyroid acropachy.
Unlike the other manifestations of Graves disease, the female-to-male ratio for thyroid acropachy is 1:1.
Age
Typically, Graves disease is a disease of young women, but it may occur in persons of any age.
The typical age range is 20-40 years.
Most affected women are aged 30-60 years.
Although pediatric cases are rare, Beliard et al reported on Graves disease in a 12-month-old infant. [33]
Prognosis
The natural history of Graves disease is that most patients become hypothyroid and require replacement. Similarly, the ophthalmopathy generally becomes quiescent. On occasion, hyperthyroidism returns because of persisting thyroid tissue after ablation and high antibody titers of anti-TSI. Further therapy may be necessary in the form of surgery or radioactive iodine ablation.
A study by Tun et al indicated that in patients with Graves disease receiving thionamide therapy, high TSH receptor–stimulating antibody (TRab) levels at diagnosis of the disease and/or high TRab levels at treatment cessation are risk factors for relapse, particularly within the first two years. The study included 266 patients. [34]
A retrospective study by Rabon et al indicated that in children with Graves disease, antithyroid drugs usually do not induce remission, although most children who do achieve remission through these agents do not relapse. Of 268 children who were started on an antithyroid drug, 57 (21%) experienced remission, with 16 of them (28%) relapsing. [35]
A study by Song et al indicated that in patients with long-standing Graves disease, following a 2-year course of antithyroid drugs, the risk of developing diabetes mellitus is 1.18 times higher than that of controls. More specifically, the investigators reported that in patients who, following a 2-year course of antithyroid drugs, continued on such medications for at least 1 more year, with no radioactive iodine ablation, the risk for diabetes was 1.17 times higher. For those who at some point after the initial 24-month drug course underwent radioactive iodine ablation, the risk was 1.88 times higher. It was also found that the diabetes risk rose as the duration of antithyroid drug treatment increased. [36]
Patient Education
Awareness of the symptoms related to hyperthyroidism and hypothyroidism is important, especially in the titration of antithyroid agents and in replacement therapy for hypothyroidism.
Patients also should be aware of the potential adverse effects of these medicines. They should watch for fever, sore throat, and throat ulcers.
Patients also must be instructed to avoid cold medicines that contain alpha-adrenergic agonists such as ephedrine or pseudoephedrine.
-
Pathophysiologic mechanisms of Graves disease relating thyroid-stimulating immunoglobulins to hyperthyroidism and ophthalmopathy. T4 is levothyroxine. T3 is triiodothyronine.
-
Graves disease. Varying degrees of manifestations of Graves ophthalmopathy.








