Practice Essentials
A glucagonoma is a rare neuroendocrine tumor that originates almost exclusively in the pancreas and probably accounts for 1% of all neuroendocrine tumors. Malignant glucagonomas are islet cell pancreatic tumors that are discovered because of glucagonoma syndrome (in which the glucagonoma autonomously secretes glucagon), because of local mass effects, or incidentally. [1] Glucagonomas originate from the alpha-2 cells of the pancreas. Unregulated production (overproduction) of peptide hormones and growth factors, which are not normally expressed in the tissue of origin, is characteristic of neuroendocrine tumors. Abnormal production of these bioactive peptides can lead to significant systemic toxic consequences and to the promotion of further tumor growth. [2, 3]
In 75-80% of cases, the glucagonoma starts in malignant form, and in 50% of these cases, metastasis exists at diagnosis. The tumor's presence is characterized by glucagon overproduction, weight loss, hyperglycemia, diabetes mellitus, hypoaminoacidemia, normochromic and normocytic anemia, and necrolytic migratory erythema (NME), which is the most characteristic clinical sign (as opposed to symptom) of this pathology. NME presents as phlogistic damage to tissues in areas exposed to friction and pressure. See the image below.
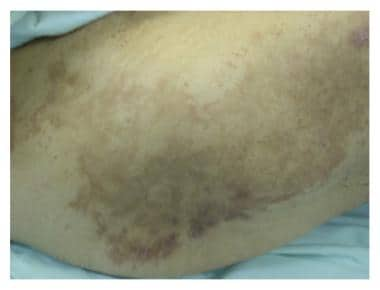 Necrolytic migratory erythema over the back with areas of healing and hyperpigmentation. Courtesy of Case Reports in Surgery (https://www.hindawi.com/journals/cris/2016/1484089/).
Necrolytic migratory erythema over the back with areas of healing and hyperpigmentation. Courtesy of Case Reports in Surgery (https://www.hindawi.com/journals/cris/2016/1484089/).
Another noteworthy feature of glucagonoma syndrome is a high rate of thromboembolic complications and consequent pulmonary embolism; this is dangerous for many patients, who can succumb to it. As NME may be the only manifestation during the development of glucagonomas that is malignant, its early recognition and correct diagnosis is very important for a better prognosis. [4]
Glucagonomas that are not associated with glucagonoma syndrome are diagnosed in various ways. The tumor may appear as a malignant pancreatic tumor discovered because of local growth, with or without metastases, or the tumor may be associated with insulinoma or gastrinoma. Glucagonoma may also occur as a single microadenoma found incidentally at autopsy in elderly patients. Similar to other islet cell tumors, the primary and metastatic lesions are slow growing.
The vast majority of glucagonomas are sporadic (80%) with the remainder associated with multiple endocrine neoplasia type 1 (MEN1), an inherited tumor predisposition syndrome, or Mahvash disease, an extremely rare cause of familial pancreatic α-cell hyperplasia and glucagonoma due to inactivating mutations in the glucagon receptor (GCGR) gene. [5]
The causes of sporadic glucagonomoas remain unknown, and it is noteworthy that some cases of NME without glucagonoma have been reported. [6] It has been suggested that in such patients, hyponutrition, especially that resulting from a lack of vitamins and minerals, causes differentiation/proliferation modifications of keratinocytes. [7, 8]
Treatment may vary by stage of disease. If possible, surgical resection and debulking procedures are performed, as resection is the only curative therapy. Somatostatin analogs (eg, octreotide, octreotide long-acting) are used in patients with unresectable glucagonomas. In patients with diffuse metastases, antineoplastic drugs may be useful for palliating symptoms. See Treatment and Medication.
Pathophysiology
Although the relationship between hyperglucagonemia and necrolytic migratory erythema (NME) is not clear, elevated glucagon serum levels can be found at the same time as this cutaneous manifestation of the disease. Glucagon is a peptidic hormone mostly produced from alpha-2 cells of the pancreas and, in smaller amounts, from amine precursor uptake and decarboxylation (APUD) cells in gastric and duodenal mucosa. Three known forms of this hormone exist:
-
The pancreatic form contains 29 amino acids and has a molecular weight of 3485 daltons.
-
The gastric form contains 29 amino acids and has a molecular weight of 3500 daltons.
-
The enteric form, or enteroglucagon, contains a polypeptidic chain, has a high molecular weight, and is biologically and chemically different from other hormones, although it cross-reacts with them.
Glucagon is secreted under the influence of various factors. The most important of these is the reduced blood concentration of glucose. Acetylcholine and catecholamines elevate serum levels of glucagon and somatostatin; serotonin reduces these levels. Physiologic glucagon activity includes the following:
-
Glycogenolysis activation with contemporary glycolysis inhibition and activation of the gluconeogenesis
-
Stimulation of lipolysis and catecholamine secretion
-
Inhibition of gastric secreting activity, pancreatic secreting activity, and gastrointestinal motility
-
Stimulation of urinary excretion of water and phosphates, as well as of sodium, calcium, and magnesium ions
Hyperglycemia linked to glucagonoma is a consequence of the glycogenolytic and gluconeogenic effects of glucagon. Similarly, glucagon excess (or relative glucagon excess) can be observed in diabetes mellitus and its complication, diabetic ketoacidosis.
Glucagon secretion by a tumor is independent of feedback control mechanisms; the subsequent increase in glucagon concentration in the blood produces characteristic symptoms. Diabetes mellitus occurs in patients with glucagonoma because of the lack of equilibrium between insulin production and glucagon production (which occurs when high serum levels of glucagon and normal levels of insulin exist or when insulin production is reduced and a normal glucagon level is present). However, glucagon may not induce hyperglycemia directly unless the metabolism of glucose by the liver is directly compromised.
Another factor affecting glucagon secretion may be variation in the molecular species of glucagon that is present in each case, and the biologic potency of these molecular species of glucagon. Weight loss is due to the action of glucagon on lipid and protein metabolism; increased caloric expenditure, as determined by the proteic catabolism; and the consequent increase of gluconeogenesis and ureagenesis. This mechanism is probably also responsible for the anemia and hypoaminoacidemia observed in some patients with glucagonoma. Thromboembolism, occasionally observed in patients, is attributable to the production of a molecule similar to coagulation factor X by tumor cells.
Although many theories about the pathogenesis of NME exist, the process of pathogenesis is not explained with certainty. According to one theory, NME can be caused by a tryptophan loss in cutaneous tissues because of the excess circulating glucagon. The amino acid tryptophan is responsible for the function of niacin (pellagra prevention vitamin), which regulates cell turnover, capillary tone, and the maturation of the epidermis and mucosal epithelia.
According to another theory, NME is related to the hypoalbuminemia due to glucagon excess; in fact, albumin acts as a carrier for zinc and essential fatty acids. Zinc carries out a fundamental role in the maintenance of cutaneous trophism. The mineral is also responsible for the linoleic acid desaturation and is therefore involved in prostaglandin synthesis, which could determine phlogistic damage to tissues in areas exposed to friction and pressure if it occurs in excess. NME may also occur in areas of cutaneous trauma.
Epidemiology
A study by Yao and colleagues, based on an analysis of the Surveillance, Epidemiology, and End Results (SEER) program database between 1973–2003, reported the occurrence of a total of 2705 cases of endocrine pancreatic tumors in the United States. According to these authors, the incidence of glucagonoma is very low, with islet cell neoplasms accounting for 1.3% of pancreatic cancers. [9]
Glucagonoma probably accounts for 1% of all neuroendocrine tumors. The annual incidence rate is estimated at 1 case per 20 million population, but that is probably an underestimation because of the relative lack of specificity of the symptoms. Autopsy studies have reported the incidence of islet cell tumors with glucagon-expressing cells at approximately 1%, supporting the assertion that many of these tumors are undiagnosed and may be associated with subclinical disease. [10]
No race prevalence is known for glucagonoma. The frequency of glucagonoma in males and females is nearly equal, although a greater incidence has been reported in females. Most patients with glucagonoma are in the sixth decade of life, with a mean age of 55 years and an age range of 19-84 years.
Prognosis
The rate of survival after 5 years is difficult to determine because of the small number of patients who develop the disease. Glucagonomas have a slow rate of growth. Most cases start with nonspecific symptoms and the average delay in diagnosis has been reported to be 3 years. [11] Approximately 50% of cases have metastases at diagnosis; for patients in whom metastasis has occurred, the prognosis is poor. Metastasis is principally to the liver or the locoregional lymph nodes.
Like other islet cell neoplasms, glucagonomas may overproduce multiple hormones, each of which can have clinical manifestations. Insulin is the second-most-common hormone secreted by these tumors. Others include (in order of frequency) adrenocorticotropic hormone (ACTH), pancreatic polypeptide, and parathyroid hormone (PTH) or substances with activity similar to PTH, such as gastrin, serotonin, vasoactive intestinal polypeptide (VIP), and melanocyte-stimulating hormone (MSH).
-
A section of a glucagonoma mass with several fiber bundles and solid cellular strands (125 X). Courtesy of Professor Pantaleo Bufo, University of Foggia, Italy.
-
A section of a glucagonoma mass with irregular aspects of fiber bundles and cellular strands (400 X). Courtesy of Professor Pantaleo Bufo, University of Foggia, Italy.
-
Bland embolization of the right hepatic artery in a patient with metastatic neuroendocrine tumors: Part 1. Courtesy of Memorial Sloan-Kettering Cancer Center.
-
Bland embolization of the right hepatic artery in a patient with metastatic neuroendocrine tumors: Part 2. Courtesy of Memorial Sloan-Kettering Cancer Center.
-
Postprocedure computed tompgraphy scans after bland embolization of the right hepatic artery in a patient with metastatic neuroendocrine tumors. Courtesy of Memorial Sloan-Kettering Cancer Center.
-
Necrolytic migratory erythema over the back with areas of healing and hyperpigmentation. Courtesy of Case Reports in Surgery (https://www.hindawi.com/journals/cris/2016/1484089/).
-
Necrolytic migratory erythema. Courtesy of Rare Tumors (SAGE Publications Ltd) (http://www.pagepress.org/journals/index.php/rt/article/view/rt.2009.e6/1169).






