Background
Familial adenomatous polyposis (FAP) is the most common adenomatous polyposis syndrome. It is an autosomal dominant inherited disorder characterized by the early onset of hundreds to thousands of adenomatous polyps throughout the colon. If left untreated, all patients with this syndrome will develop colon cancer by age 35-40 years. In addition, an increased risk exists for the development of other malignancies. See the image below.
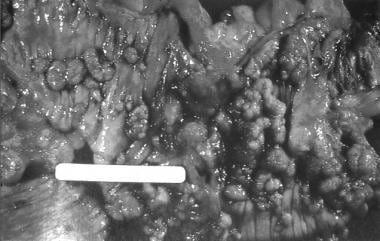 Colectomy specimen obtained from a patient with familial adenomatous polyposis. Note the presence of numerous synchronous adenomatous polyps lining the luminal surface.
Colectomy specimen obtained from a patient with familial adenomatous polyposis. Note the presence of numerous synchronous adenomatous polyps lining the luminal surface.
See Benign or Malignant: Can You Identify These Colonic Lesions?, a Critical Images slideshow, to help identify the features of benign lesions as well as those with malignant potential.
The genetic defect in FAP is a germline mutation in the adenomatous polyposis coli (APC) gene. Syndromes once thought to be distinct from FAP are now recognized to be, in reality, part of the phenotypic spectrum of FAP. [1]
Syndromes with a germline mutation in the APC gene include FAP, Gardner syndrome, some families with Turcot syndrome, and attenuated adenomatous polyposis coli (AAPC). Gardner syndrome is characterized by colonic polyposis typical of FAP, along with osteomas (bony growth most commonly on the skull and the mandible), dental abnormalities, and soft tissue tumors. Turcot syndrome is characterized by the colonic polyposis that is typical of FAP, along with central nervous system tumors (medulloblastoma). AAPC is characterized by fewer colonic polyps (average number of polyps, 30-35) as compared with the classic FAP. The polyps also tend to develop at a later age (average age, 36 y), and they tend to involve the proximal colonic area. [2]
In considering the spectrum of polyposis syndromes, patients with multiple adenomatous polyps most likely have FAP (or one of its variants), AAPC, or MYH-associated polyposis (MAP). If a patient with a suspected polyposis syndrome undergoes genetic testing and does not have an APC gene mutation, MYH gene testing should be performed to assess for MAP, as 10%-20% of patients who do not have an APC gene mutation have biallelic MYH gene mutations. [3]
The phenotype of MAP is often indistinguishable from FAP or AAPC, with patients having usually 10-100 polyps but sometimes more than 100. The age of onset of MAP is usually in patients older than 45 years, and patients often present symptomatically, with colorectal carcinoma commonly found at the time of the diagnosis. This is in part because there is usually no family history given the autosomal recessive inheritance pattern of MAP. Duodenal polyps can be found in up to one fifth of patients. [4] There is no increased risk of other types of cancers associated with this syndrome.
Pathophysiology
The APC gene is a tumor suppressor gene that is located on band 5q21. [5] Its function is not completely understood but has been shown to play a part in metaphase chromosome alignment. [6] Normal APC protein promotes apoptosis in colonic cells. Its most important function may be to sequester the growth stimulatory effects of b-catenin, a protein that transcriptionally activates growth-associated genes in conjunction with tissue-coding factors. Mutations of the APC gene result in a truncated/nonfunctional protein.
The resultant loss of APC function prevents apoptosis and allows b-catenin to accumulate intracellularly and to stimulate cell growth with the consequent development of adenomas. As the clonal expansion of cells that lack APC function occurs, their rapid growth increases the possibility for other growth-advantageous genetic events to occur. This causes alterations in the expression of a variety of genes, thereby affecting the proliferation, differentiation, migration, and apoptosis of cells.
Ultimately, enough genetic events transpire that allow the adenomatous polyps to become malignant in patients with FAP. This process is similar to that which occurs in sporadic adenomas. As a result, APC is considered the gatekeeper of colonic neoplasia. Its mutation/inactivation is the initial step in the development of colorectal cancer in patients with FAP.
Germline (ie, inherited) mutations of the APC gene, as is the case with FAP, result in cells containing one mutated copy and one normal copy of the gene. Patients inherit one mutated APC allele from an affected parent, and adenomas develop as the second allele from the unaffected parent becomes mutated or lost. Consequently, every colonic epithelial cell in patients with FAP has one mutated APC allele. Inactivation of the remaining normal copy of the APC gene, by deletion or mutation, completely removes the tumor suppressive function of APC, thus initiating the growth of adenomatous polyps. Inactivation of the second APC allele occurs frequently in the colon, resulting in the development of numerous adenomas.
A retrospective study of outcomes in 492 patients with polyposis found that the age at polyposis onset and years of survival differed significantly by genotype, although the age of onset of colorectal cancer did not. [7] Patients with a mutation in APC 0-178 or 312-412 developed polyposis later and survived longer, whereas patients with mutations in APC 1249-1549 developed polyposis earlier and did not survive as long.
Etiology
FAP is caused by a germline mutation of the APC tumor suppressor gene, located on band 5q21. Most mutations of the APC gene are nonsense or frameshift mutations, leading to truncation of the APC protein (nonfunctional protein).
More virulent forms of FAP are associated with a mutation in exon 15 between codons 1250 and 1464, the middle portion of the gene. [8]
In patients with AAPC, mutations of the APC gene occur at the extreme amino terminus of the protein.
Epidemiology
United States data
Estimates vary from 1 case in 6,850 persons to 1 case in 31,250 persons.
International data
The frequency is constant worldwide.
Race-, sex-, and age-related demographics
FAP has been described in all races, and males and females are equally affected (1:1).
The average age of onset of polyposis in FAP is 16 years, whereas the average age of onset for colorectal cancer is 39 years.
The average age of onset for polyps in AAPC is 36 years, and the average age of onset for cancer in AAPC is 54 years. These patients have fewer polyps (approximately 30 polyps) compared to patients with FAP.
Prognosis
Patients with untreated FAP have a median life expectancy of 42 years. Life expectancy is extended greatly in those treated with colectomy.
Upper gastrointestinal cancers and desmoid tumors are the most common causes of death in patients who have undergone colectomy. This is why surveillance programs, especially after colectomy, are essential. Colectomy only addresses the risk of colon cancer development.
The cumulative probability of developing any type of noncolorectal cancer, mostly periampullary tumors, is 11% by age 50 years and 52% by age 75 years.
Morbidity/mortality
The principal cause of mortality is colorectal cancer, which develops in all patients unless they are treated. The mean age at which colorectal cancer develops in patients with classic FAP is 39 years. Patients with adenomatous polyposis itself often are asymptomatic.
The second reported lethal complication of FAP is diffuse mesenteric fibromatosis and is referred to as a desmoid tumor. It involves intra-abdominal organs and vessels, causing gastrointestinal obstruction and constriction of veins, arteries, and ureters. Desmoid tumors are reported in 4%-32% of patients. Even after the appropriate surgical treatment of FAP, 20% of patients may develop desmoid tumors after colectomy. Studies have not found a correlation between specific APC mutation sites and desmoid tumor development. [9] Risk factors include a positive family history. The mortality from these tumors is 10%-50%. The second most common malignancy in patients with FAP is adenocarcinoma of the duodenum and the papilla of Vater. It affects as many as 12% of patients.
Rarer cancers associated with FAP include medulloblastomas (Turcot syndrome), hepatoblastoma, thyroid cancer, gastric cancer, pancreatic cancer, and adrenal cancer. [10]
Complications
Complications of FAP include the following:
-
Colorectal cancer (100% in untreated patients)
-
Duodenal or periampullary adenocarcinoma (4%-12%)
-
Desmoid formation (as many as 20%, typically postcolectomy)
-
Other cancers, including medulloblastoma, hepatoblastoma, thyroid cancer, gastric cancer, pancreatic cancer, and adrenal cancer
-
Development of rectal cancer in patients with a retained rectum
-
Colectomy specimen obtained from a patient with familial adenomatous polyposis. Note the presence of numerous synchronous adenomatous polyps lining the luminal surface.







