Practice Essentials
Adrenal masses are frequently discovered incidentally and are then termed adrenal incidentalomas (AIs). They are often found after performance of an imaging procedure that is unrelated to the adrenal gland. Usually, the patient has no signs of hormonal excess or obvious underlying malignancy. Incidence has been increasing proportional to the use of radiographic imaging, as shown in the images below. [1] Less commonly, AIs are discovered as part of the clinical workup for suspected adrenal disease (eg, Cushing syndrome). (See Workup, as well as Clinical Presentation.)

The differential diagnosis of AIs includes many primary, metastatic, benign, and malignant entities, most of which are not discussed at length here. (See Diagnosis)
Adrenal cortical adenoma is a common benign tumor arising from the cortex of the adrenal gland. It commonly occurs in adults, but it can be found in persons of any age. Adrenal cortical adenomas are not considered to have the potential for malignant transformation (see the images below).
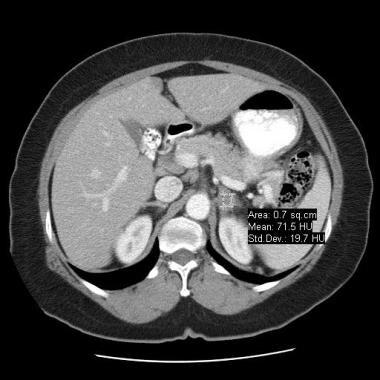
 Homogeneous, well-defined, 7-HU ovoid mass is seen in the right adrenal gland; this finding is diagnostic of a benign adrenal incidentaloma.
Homogeneous, well-defined, 7-HU ovoid mass is seen in the right adrenal gland; this finding is diagnostic of a benign adrenal incidentaloma.
Because adrenal metastases may be found in as many as 25% of patients with known primary lesions, radiologists frequently face the task of determining whether an adrenal mass is benign or malignant. The question can directly affect the clinical management of the case. For instance, the workup for an otherwise resectable lung cancer may reveal the presence of an adrenal mass and suggest the possibility of metastatic disease. (See Workup.)
The treatment for a hormonally active (functional) adrenal tumor is surgery. The treatment for a malignancy depends on the cell type, spread, and location of the primary tumor. [2] Nonfunctional adrenal cortical adenomas are not premalignant, and surgical excision is not indicated. (See Treatment and Management.)
Signs and symptoms of adrenal incidentaloma
Pheochromocytomalike symptoms include episodic attacks, palpitations, sweats, headaches, and abdominal pain, as well as labile hypertension. Pheochromocytomas (the most important hormonally silent AIs) should be considered in all AI cases because they are more common than previously thought, the diagnosis is often overlooked, and a failure to recognize them may lead to patient death.
Primary hyperaldosteronism includes hypertension and unprovoked hypokalemia. However, more patients are being identified who have normal potassium levels.
Patients with adrenal carcinoma report weight loss. Virilization is reported in women (for androgen-secreting tumors), and feminization in men (for estrogen-secreting tumors).
Cushing syndrome (reflecting cortisol-secreting adenomas) includes weight gain, weakness, depression, and bruising.
Workup in adrenal incidentaloma
Biochemical tests used in the assessment of AIs include evaluation of the following:
-
Pheochromocytoma - Urine and plasma free metanephrines
-
Primary aldosteronism - Plasma aldosterone-to-renin ratio
-
Adrenocortical carcinoma - Urine 17-ketosteroids
-
Cushing or "silent" Cushing syndrome - Overnight 1-mg dexamethasone test
The imaging modalities of choice in the evaluation of an adrenal mass are computed tomography (CT) scanning, magnetic resonance imaging (MRI), and positron-emission tomography (PET) scanning.
Adrenal fine-needle aspiration (FNA) helps to identify metastatic, systemic, and hemorrhagic disease of the adrenal glands. It cannot distinguish between benign and malignant primary adrenal tumors and should be used only when an AI cannot be diagnosed clinically or hormonally. [3]
Management
Conditions that do not warrant surgery include bilateral adrenal diseases such as corticotropin-dependent Cushing disease and bilateral hyperaldosteronism. Nonfunctional (hormonally silent) adrenal cortical adenomas are not premalignant, and surgical excision is not indicated.
The treatment for a hormonally active adrenal tumor is surgery. The treatment for a malignancy depends on the cell type, spread, and location of the primary tumor. [2]
No randomized trials have compared laparotomy versus laparoscopic adrenalectomy; however, abdominal laparotomy is preferred for bilateral disease, large masses (>10 cm), possible malignant disease, and pheochromocytoma.
Anatomy
The adrenal glands are located in the perirenal space near the upper pole of each kidney. Their appearance varies: they may be shaped like the letter H, L, Y, T, or V. Typically, they are less than 4 cm in length and less than 1 cm in width.
Pathophysiology
The biochemical mechanisms depend on the underlying cell type. The cellular mechanisms for primary adrenocortical tumorigenesis are just beginning to be understood.
Etiology
Some studies report an association with chromosomal and genetic abnormalities (genes coding for p53 and p57). Tumor markers are also present in other syndromes. The multiple endocrine neoplasia (MEN1) gene is linked to multiple endocrine neoplasia type 1. The aldosynthase/11-beta hydroxylase hybrid gene is associated with glucocorticoid-remediable hyperaldosteronism.
Another very rare cause of Cushing syndrome is adrenal-dependent macronodular hyperplasia associated with extremely large adrenal glands.
Epidemiology
Adrenal incidentalomas (AIs) are a common finding on cross-sectional abdominal images. In about 1-5% of all cases, abdominal computed tomography (CT) scans that are obtained for reasons other than the evaluation for possible adrenal neoplasm demonstrate an adrenal mass; most of these are AIs. The autopsy prevalence for AIs is 2-9% (see Table 1).
Table 1. Prevalence of AIs (Open Table in a new window)
Author |
Method |
Sample Size |
Prevalence, % |
Russl (1941) |
Autopsy (>1 cm) |
131/9000 |
1.5 |
Kokko (1967) [4] |
Autopsy (>5 mm) |
21/1495 |
1.5 |
Hedeland (1967) |
Autopsy (>2 mm) |
64/739 |
8.7 |
Glazer (1982) [5] |
CT scan |
16/2200 |
0.7 |
Abecassis (1985) [6] |
CT scan |
19/1459 |
1.3 |
Belldegrun (1986) [7] |
CT scan |
88/12000 |
0.7 |
Herrera (1991) [8] |
CT scan |
259/61054 |
0.4 |
Approximately 1-10% of CT scans and magnetic resonance images (MRIs) detect AIs that are 5 mm or larger. An Italian study of incidentally discovered AIs among subjects undergoing chest CT scan found that the prevalence of AIs was approximately 4%. [9]
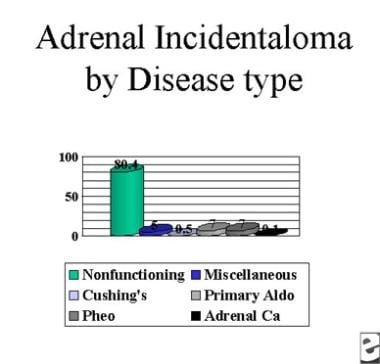
The most important hormonally silent AI is pheochromocytoma. They are present in approximately 1 in 1000 autopsies. If the prevalence of AIs is 10-100 in 1000, then 1-10% of AIs are pheochromocytomas, as noted in the image below.
A study by Falhammar et al of 94 cases of pheochromocytoma, as encountered at a single center, determined that 64% were identified as incidentalomas, while 32% were found in patients suspected of having a pheochromocytoma. In another 4% of cases, patients were screened for the lesion because they were known to have MEN2A. [10]
Demographic distribution for AI
Prevalence increases with age; the rate is less than 1% for patients younger than 30 years and is 7% for patients 70 years or older. Evidence suggests that the incidence in teenage girls is slightly higher than that of teenage boys, but no sex-related predilection is found in adults. AI prevalence is higher in white than in black people and in obese, diabetic, and hypertensive patients. [11]
Prognosis
Generally, the prognosis is excellent, but it depends on the type of underlying adrenal disease.
Approximately 85% of AIs are nonfunctional (hormonally silent) and benign. The other 15% of AIs are either functional (hormonally active) or malignant and require further evaluation and treatment to avoid medical complications. [12, 13, 14]
A multicenter, retrospective study by Herrera-Martínez et al indicated that mild autonomous cortisol secretion (MACS) from AIs is associated with increased comorbidities and mortality when adenomas outside the adrenal gland are also present. The investigators found, for example, that in persons with thyroid adenomas, those who also have AIs with MACS are more likely to experience hypertension, diabetes, and cerebrovascular complications than are those with nonfunctioning AIs. The cerebrovascular complication rates for these patients in the study were 18.5% and 9.1%, respectively, while the mortality rates were 6.2% and 0%, respectively. [15]
A multicenter, retrospective, observational study by Araujo-Castro et al indicated that the risk of nonfunctioning AIs developing autonomous cortisol secretion is greater when, at diagnosis, the serum cortisol post–dexamethasone suppression test level is higher. Using a 1-mg dexamethasone suppression test, the investigators found that the hazard ratio (HR) for such development increased by 6.44 for every μg/dL. It was also indicated that AIs are more likely to enlarge in female patients than in males, the HR being 10.71. In the study, 10.5% of nonfunctioning AIs developed autonomous cortisol secretion (here defined as a serum cortisol post–dexamethasone suppression test level of over 1.8 μg/dL), and 5.2% of AIs underwent significant growth, with the mean follow-up period being 41.3 months. [16]
Patients with a previous history of cancer have a clinical course dictated by the primary tumor. Patients with adrenal cortical carcinomas have poor clinical outcomes, usually a 2- to 5-year 50% overall survival rate.
Approximately 3-7 percent of AIs prove to be pheochromocytomas. [12, 13, 17] Pheochromocytomas may result in substantial complications, including death if not recognized. A 1981 series reported that less than one quarter of pheochromocytomas found post mortem were diagnosed ante mortem. [18] More than 90% of these patients had characteristic symptoms suggesting the unrecognized tumors were not silent. Many of the patients died of causes possibly related to the pheochromocytoma. Approximately 29% died unexpectedly during surgery, 27% died from cardiovascular causes, and 17% died from cerebrovascular causes.
Patient Education
If pertinent, patients should know the signs and symptoms of adrenal insufficiency. Clinical clues include nausea, abdominal pain, fever, and diarrhea.
-
Characteristics of adrenal masses and their malignant potential.
-
Differential diagnosis of adrenal mass
-
Pituitary-adrenal axis and cortisol-secreting adrenal mass.
-
Adrenal incidentaloma and disease type.
-
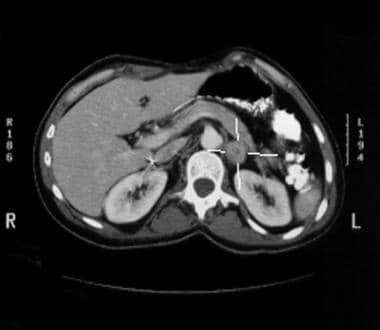
Left adrenal mass discovered incidentally.
-
Close-up of the left adrenal incidentaloma from the above image.
-
Homogeneous, well-defined, 7-HU ovoid mass is seen in the right adrenal gland; this finding is diagnostic of a benign adrenal incidentaloma.
-
Homogeneously enhancing ovoid mass is seen in the left adrenal gland.
Tables
Author |
Method |
Sample Size |
Prevalence, % |
Russl (1941) |
Autopsy (>1 cm) |
131/9000 |
1.5 |
Kokko (1967) [4] |
Autopsy (>5 mm) |
21/1495 |
1.5 |
Hedeland (1967) |
Autopsy (>2 mm) |
64/739 |
8.7 |
Glazer (1982) [5] |
CT scan |
16/2200 |
0.7 |
Abecassis (1985) [6] |
CT scan |
19/1459 |
1.3 |
Belldegrun (1986) [7] |
CT scan |
88/12000 |
0.7 |
Herrera (1991) [8] |
CT scan |
259/61054 |
0.4 |
Diagnosis |
Features |
Biochemical Tests |
Pheochromocytoma |
High blood pressure, catechol symptoms |
Urine and plasma free metanephrines |
Primary aldosteronism |
High blood pressure, low K+, low PRA* |
Plasma aldosterone-to-renin ratio |
Adrenocortical carcinoma |
Virilization or feminization |
Urine 17-ketosteroids |
Cushing or "silent" Cushing syndrome |
Cushing symptoms or normal examination results |
Overnight 1-mg dexamethasone test |
*Plasma renin activity |
||






