CMV Gastrointestinal Disease
After colitis, esophagitis is the most common gastrointestinal (GI) manifestation of cytomegalovirus (CMV) infection. [1] This condition has been reported in organ transplant patients, those undergoing long-term renal dialysis, patients with human immunodeficiency virus (HIV) infection or acquired immunodeficiency syndrome (AIDS), as well as in individuals with other debilitating diseases. [1] One case report has described an elderly diabetic, hypertensive man, who previously underwent renal transplantation and was receiving immunosuppressant agents, with esophageal and gastric ulceration and laboratory confirmation (by polymerase chain reaction) of synchronous CMV, herpes simplex virus, and Epstein-Barr virus infections. [2]
CMV GI disease was first described in the 1960s. The average time to the development of CMV esophagitis after solid organ transplantation is 5-7 months. Patients undergoing bone marrow transplantation may develop CMV disease much earlier, at an average of 2-3 months, with symptoms occurring as early as 10 days after an allogenic bone marrow transplantation. [3, 4]
Patients with CMV esophagitis may have superimposed CMV colitis (in which case, care at a skilled nursing facility may be necessary).
Individuals with HIV infection are at an increased risk for CMV esophagitis when their CD4+ lymphocyte counts fall to less than 100 cells/µL. In patients with HIV infection or AIDS, CMV infection is an opportunistic infection that signals a decline in patient immunity.
CMV esophagitis has been described in only a few patients who have been immunocompromised by conditions other than transplantation, HIV infection, or AIDS. Some cases have occurred in patients undergoing chemotherapy for esophageal cancer [5, 6] or other malignancies (eg, cancers of the lung, stomach, or ampulla of Vater; and lymphoma). [1]
At least one case of CMV esophagitis has been reported in a healthy host. [7] CMV esophagitis has been reported in a few immunocompetent patients. [8, 9] One of the patients was an elderly woman with Parkinson disease and aspiration pneumonia. [8]
Overview of Cytomegalovirus
Cytomegalovirus (CMV) is a member of the Herpesviridae family, along with herpes simplex viruses (HSVs) 1 and 2, Epstein-Barr virus, varicella-zoster virus, and others. CMV is a double-stranded deoxyribonucleic acid (DNA) virus with a protein coat and a lipoprotein envelope.
Similar to other herpesviruses, CMV is icosahedral and replicates in the host's nucleus. As with the other members of this family, CMV has the ability to produce a latent infection. Replication in the host cell is typically represented by large, intranuclear inclusion bodies and smaller cytoplasmic inclusions. An inclusion body is seen in the image below.
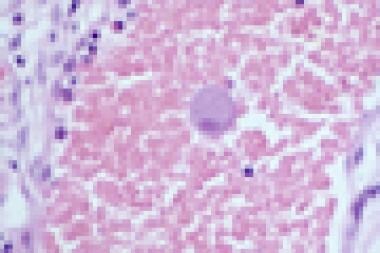 Characteristic giant cell with inclusion body in a patient with cytomegalovirus esophagitis.
Characteristic giant cell with inclusion body in a patient with cytomegalovirus esophagitis.
Studies have shown that 50%-80% of the world's population is seropositive for CMV. The two peaks for primary CMV infection occur in preschool children and young adults. With the advent of immunosuppressive medications and the increased incidence of human immunodeficiency virus (HIV) infection and acquired immunodeficiency syndrome (AIDS) in the early 1980s, a new class of CMV infection was described.
CMV retinitis, adrenalitis, pneumonia, colitis, and esophagitis are some of the conditions observed in immunocompromised hosts. [10] CMV is the third most common pathogen in patients with AIDS, superseded only by Pneumocystis carinii and Candida.
Patterns of CMV infection
Three major patterns of CMV infection are described.
The first is primary infection, in which the patient has never been exposed to the pathogen but becomes infected by a patient who is seropositive for the virus. This pattern accounts for 60% of cases. Primary infection in immunocompetent hosts causes few or no symptoms. Studies with in-situ hybridization have shown that CMV DNA can persist in a latent form in most organs of the body.
The second pattern, reactivation, occurs in a patient who is seropositive with a latent virus that becomes reactivated when the host's immune system becomes compromised. This occurs in 10%-20% of cases.
The third pattern is superinfection, which occurs in 20%-40% of cases. In this setting, a patient is seropositive for CMV and receives latently infected cells from another seropositive patient. The resulting CMV infection is from the latent donor cells, not the recipient cells.
Once a patient becomes infected, CMV can persist in the host tissues indefinitely. Humoral and cellular mechanisms work in concert to control CMV infections and maintain the latent phase. However, if the host's T-cell response becomes compromised by disease or iatrogenic causes, the latent virus can be reactivated to cause a variety of syndromes.
CMV Esophagitis Risk Factors and Complications
Risk factors that predispose individuals to cytomegalovirus (CMV) esophagitis include the following:
-
Human immunodeficiency virus (HIV) infection or acquired immunodeficiency syndrome (AIDS)
-
High- or low-dose corticosteroid therapy
-
Immunosuppressive therapy following transplantation
-
History of blood transfusion
-
Advancing age
-
Anything that can decrease an individual’s immunity
Potential complications of CMV esophagitis include the following:
-
Perforation (rarely)
-
Periesophageal pseudoaneurysms [13]
Epidemiology
Prevalence
Approximately 8%-28% of patients with acquired immunodeficiency syndrome (AIDS) who undergo esophagogastroduodenoscopy (EGD) for dysphagia or odynophagia are found to have cultures positive for cytomegalovirus (CMV) in tissues obtained from the esophagus. Approximately 38% of bone marrow transplant patients who undergo EGD for unexplained nausea and vomiting are positive for CMV esophagitis and/or small intestine involvement.
Race-, sex-, and age-related demographics in CMV esophagitis
CMV esophagitis has no race or documented sex predilection.
No reports on age-related predilection have been published. However, because immunocompetence generally decreases with age, older patients are at higher risk for developing CMV disease than are younger patients. In children, CMV is the third most common cause of infectious esophagitis after Candida albicans and herpes simplex virus (HSV). [14, 15]
Prognosis
With rapid diagnosis and proper antiviral therapy, the prognosis of patients with cytomegalovirus (CMV) disease has dramatically improved.
Morbidity and mortality in CMV esophagitis
Because CMV esophagitis occurs in immunocompromised hosts, the morbidity and mortality attributed to the esophagitis itself is difficult to quantitate.
Patients with CMV esophagitis may report severe dysphagia and/or odynophagia, preventing the already undernourished patient from obtaining much-needed nutrients. This can result in a progressive worsening of the patient's condition.
As the patient's condition worsens, the risk of disseminated CMV infection increases. Historically, the mortality rate associated with CMV disease in transplantation patients has been 85%. However, with the advent of the antiviral drug ganciclovir, mortality has been markedly reduced.
Differential Diagnosis in CMV Esophagitis
Conditions that mimic the symptoms of cytomegalovirus (CMV) esophagitis include the following:
The following conditions should also be considered in the differential diagnosis:
-
Aphthous ulcers or idiopathic ulcers (commonly seen in patients with acquired immunodeficiency syndrome [AIDS])
-
Drug-induced dysphagia
Presentation
Symptoms
Patients with cytomegalovirus (CMV) esophagitis may have symptoms in other organs or systems (eg, colon, eyes, liver, lungs). Therefore, patients may present with multiple symptoms unrelated to the esophagitis.
Unlike herpes simplex virus (HSV) infection, patients present with a more gradual onset of symptoms. [17] Nausea, vomiting, fever, epigastric pain, diarrhea, and weight loss are nonspecific symptoms, but they are more typical of CMV infection. In contrast, patients with HSV infection present with an abrupt symptomatic onset consisting of retrosternal chest pain and painful, difficult swallowing.
Keep in mind that CMV can coexist with HSV or any other cause of esophagitis; therefore, patient presentation may vary. Recipients of solid organ transplants may develop CMV disease 7-9 months after transplantation, whereas bone marrow transplant recipients develop such disease after 2-3 months.
Presenting symptoms of patients with CMV esophagitis include the following:
-
Difficult or painful swallowing (ie, dysphagia, odynophagia, retrosternal pain)
-
Nausea and vomiting
-
Abdominal pain
-
Fever
-
Diarrhea
-
Weight loss
-
Chest pain
-
Hemoptysis
Physical examination findings
Physical examination findings may include the following:
-
Adenopathy
-
Erythematous oropharynx
-
Ulcerated oropharynx (uncommon)
Antigen Detection and Culture
Antigen detection
Clinical specimens can be stained with specific immunofluorescent antibodies to detect viral antigens or viral DNA.
Culture
The most commonly used culture technique is the shell viral assay of cultured cells, in which the immediate early antigens are detected by the use of monoclonal antibodies. This reduces the time to positivity to 24-72 hours, whereas other cultures take days to weeks.
Wilcox et al reported that viral culture and brushings add little to the evaluation of esophageal ulcers in patients with acquired immunodeficiency syndrome (AIDS) over multiple biopsy specimens with routine histology. [18]
Esophagogastroduodenoscopy
Findings from routine imaging studies are nonspecific. Therefore, the imaging study of choice is esophagogastroduodenoscopy (EGD), which allows direct visualization and allows for biopsies that aid in the diagnosis. A definitive diagnosis is established in more than 70% of cases.
Not uncommonly, large, solitary, shallow ulcers or multiple discrete lesions appear in cytomegalovirus (CMV) esophagitis, especially in the distal esophagus. However, ulceration may not be present. For example, esophageal necrosis has also been reported in a kidney transplant patient, [19] and shallow erosions have been found in a liver transplant patient. [20]
The biopsy specimen should be taken from the base of the ulcer. Studies have shown that at least 10 biopsy specimens should be obtained to yield a significant result. Specimens should be submitted for histologic examination, antigen detection, and viral culture studies.
Histologic Findings
In patients with cytomegalovirus (CMV) esophagitis, histology of the affected specimens may show acute and chronic inflammation, vasculitis, and/or mucosal ulceration. Deep biopsy specimens are preferred. Histologic staining with Papanicolaou or hematoxylin and eosin stains may reveal classic findings that include giant cells (typically 25-35 µm) (as shown in the image below) with cytomegaly and large, ovoid, or pleomorphic nuclei with basophilic inclusions. These inclusions are known as owl's eyes because of their separation from the nuclear membrane by a halo. Immunochemistry is more specific than standard staining techniques. [21]
Characteristic giant cell with inclusion body in a patient with cytomegalovirus esophagitis.
Radiation esophagitis versus CMV esophagitis
Patients with radiation esophagitis generally exhibit nonspecific and nondiagnostic endoscopic changes (eg, erythema, ulceration). [16] In addition, tissue biopsies from the affected areas demonstrate not only variable inflammatory changes but also radiation-related atypia of the endothelial and stromal cells that mimic CMV cytopathic changes. However, the absence of immunostaining rules out CMV esophagitis. [16]
Other Diagnostic Studies
Other studies, such as antibody tests, qualitative or quantitative polymerase chain reaction (PCR) studies, or studies of blood or other body fluids, yield less diagnostic information for cytomegalovirus (CMV) esophagitis and may not indicate current active infection.
Borges et al reported that although PCR may have a role in diagnosing CMV and other infectious causes of esophagitis, the presence of multiple infections in immune-compromised hosts occasionally limits the utility of PCR. [22]
In a more recent study, Bernard et al indicate that quantitative PCR in conjunction with clinical and endoscopic findings may aid in the diagnosis of CMV gastrointestinal (GI) disease. [23] In their 3-year (2007-2010) retrospective study, the investigators assessed the records of 13 patients (median age, 81 years) diagnosed with CMV GI disease via quantitative PCR and found more than half (54%) of the apparently immunocompetent patients had underlying immune-modulating conditions. The mean value of CMV DNA load in GI biopsies was 3845 copies/μg total DNA (range, 15-15500 copies/μg; two patients were later diagnosed with adenocarcinoma), but Bernard et al noted that additional research is needed to interpret quantitative values. [23]
Medical Care
Patients with HIV infection
Studies have documented the profound effect of potent antiretroviral therapy (ART) on the natural history of human immunodeficiency virus (HIV) infection. Because most patients affected by cytomegalovirus (CMV) esophagitis have HIV infection, the increased use of these newer therapies has helped in the prevention and treatment of CMV disease.
Patients receiving ART have shown a decrease in HIV viral load, increased CD4+ lymphocyte counts, decreased hospitalization, and a decreased incidence of opportunistic infections, including CMV esophagitis. For these patients, therefore, aggressive treatment of HIV infection is key to treating and preventing CMV infection.
Intravenous ganciclovir is the treatment of choice for patients with HIV infection who are also infected with CMV. If ganciclovir is contraindicated or cannot be used, intravenous foscarnet is the second-line therapy. However, Gaduputi et al documented an increased resistance to foscarnet. [24]
Combination therapy with ganciclovir and foscarnet may be effective if monotherapy fails, but this is associated with significant toxicity.
The use of oral ganciclovir is increasing in patients who require long-term suppressive treatment. [25] Long-term prophylaxis with peroral ganciclovir is considered in patients with HIV infection who have CD4+ lymphocyte counts of less than 50 cells/µL.
Patients with immunosuppressive factors other than HIV infection
Potent antiviral agents, such as ganciclovir, are also essential in the treatment of patients with non-HIV causes of immunosuppression, such as transplantation, long-term steroid use, renal dialysis, or an iatrogenic source.
Evidence has suggested that patients with invasive disease may benefit from combined ganciclovir and immunoglobulin G (IgG)-CMV (Cytotec), although conclusive evidence is lacking. [26] Data have also indicated that oral valganciclovir is comparable in safety and efficacy to intravenous ganciclovir in liver transplant recipients. [27]
Discontinuation of steroid or immunosuppressive agents in these patients is discouraged if this will further compromise the patient's health. [28] However, tapering immunosuppression may allow the patients to redevelop their immunity.
CMV esophagitis does not require surgical intervention. However, gastrointestinal (GI) CMV disease may necessitate surgical intervention for diagnosis and management, particularly in pediatric patients with invasive CMV GI disease and those with acute or chronic GI complications from CMV disease. [29]
Medical Consultations
Multiple consultations should be obtained for patients with cytomegalovirus (CMV) esophagitis.
An ophthalmologist should be consulted to evaluate the patient for CMV retinitis. Patients should self-monitor their vision and report any changes in their acuity or in the presence of floaters.
A gastroenterologist should be asked to aid in the diagnosis and treatment.
Infectious disease experts can offer advice on the treatment of CMV infection and, possibly, human immunodeficiency virus (HIV) infection, if the patient is found to be HIV positive.
Drug-resistant strains may develop, which would require alternate therapies.
Maintenance Therapy and Prophylaxis
Maintenance therapy
Maintenance therapy may be considered in patients with cytomegalovirus (CMV) esophagitis, especially in persons requiring reinduction drug therapy for relapse.
Discontinuation of long-term maintenance therapy can be considered in patients with human immunodeficiency virus (HIV) infection in whom CD4+ T-lymphocyte counts have increased to more than 100-150 cells/µL and whose HIV plasma ribonucleic acid (RNA) levels have been suppressed.
Prophylaxis
CMV vaccines are under development. Prophylactic esophageal screening has not been beneficial.
Dietary and Activity-Related Considerations
Unless the patient is unable to take food by mouth secondary to odynophagia, no special nutritional requirements are needed for those with cytomegalovirus (CMV) esophagitis. However, if a patient is not able to take food by mouth, temporary peripheral nutrition may be necessary.
No limitations on patient activity are necessary.
Pertinent Patient Information
Patients with cytomegalovirus (CMV) esophagitis should be educated about the nature of their disease and the possibility of its recurrence.
Individuals infected with human immunodeficiency virus (HIV) or who have acquired immunodeficiency syndrome (AIDS), in particular, should be aware of the possibility of disease recurrence.
For patient education information, see HIV/AIDS and HIV Testing.
-
Characteristic giant cell with inclusion body in a patient with cytomegalovirus esophagitis.
Tables

What would you like to print?
- CMV Gastrointestinal Disease
- Overview of Cytomegalovirus
- CMV Esophagitis Risk Factors and Complications
- Epidemiology
- Prognosis
- Differential Diagnosis in CMV Esophagitis
- Presentation
- Antigen Detection and Culture
- Esophagogastroduodenoscopy
- Histologic Findings
- Other Diagnostic Studies
- Medical Care
- Medical Consultations
- Maintenance Therapy and Prophylaxis
- Dietary and Activity-Related Considerations
- Pertinent Patient Information
- Show All
- References




