Background
The term coronary artery anomaly refers to a wide range of congenital abnormalities involving the origin, course, and structure of epicardial coronary arteries. By definition, these abnormalities occur in less than 1% of the general population. [1] Coronary artery anomalies are frequently found in association with other major congenital cardiac defects. This article, however, is focused on isolated coronary artery anomalies (ie, in the absence of other major congenital cardiac defects). In adults, the clinical interest in coronary anomalies relates to their occasional association with sudden death, myocardial ischemia, congestive heart failure, or endocarditis. In addition, presence of coronary artery anomalies may, at times, create challenges during coronary angiography, percutaneous coronary interventions, and coronary artery surgery. [2, 3, 4, 5]
Pathophysiology
Normal coronary artery anatomy
The coronary arteries are the only branches of the ascending aorta, and they supply blood to all structures within the pericardial cavity. Usually, the 2 coronary artery ostia are located in the center of the left and right (anterior) sinuses of the aortic valve. The posterior sinus of the aortic valve contains no coronary ostium and is often designated as the noncoronary sinus.
Left coronary artery
The left coronary artery originates from an ostium located within the left coronary sinus of the aorta, and, after a single initial trunk (left main coronary artery) of variable length and size, it gives rise to the left anterior descending (LAD) and left circumflex (LCx) coronary artery branches. The LAD coronary artery runs along the anterior interventricular sulcus, provides several superficial (diagonal) and multiple deep (septal perforator) branches, and usually reaches the cardiac apex. In some individuals, a diagonal branch may have a very proximal takeoff such that the left main (LM) gives rise to 3 instead of 2 branches. In this case, the additional artery arising from the LM originates in between the LAD and the LCx coronary arteries and is called the ramus intermedius coronary artery. This artery provides blood supply to the anterior left ventricular free wall.
The LCx coronary artery runs in the left atrioventricular groove and usually has 1 or more branches that reach the obtuse margin of the heart (obtuse marginals). The LAD coronary artery supplies blood to the anterior left ventricular wall through its diagonal branches, the anterior two thirds of the interventricular septum through its septal perforator branches, and commonly the cardiac apex by its terminal branches. The LCx coronary artery supplies blood to the left ventricular lateral and posterior walls through its obtuse marginal branches.
Right coronary artery
The right coronary artery (RCA) originates from an ostium located within the right coronary sinus of the aorta and runs in the right atrioventricular groove to reach the crux (junction of the atrioventricular groove and the posterior interventricular sulcus) of the heart. It supplies blood to the inferior (diaphragmatic) left ventricular wall and often the posterior one third of the interventricular septum as well as the free wall of the right ventricular through its right ventricular (acute marginal) branches. The posterior descending branch of the RCA supplies blood to the posterior one third of the interventricular septum. A posterolateral branch of the RCA provides blood supply to the basal most portion of the posterolateral left ventricular wall.
Arterial dominance [6]
Left or right coronary artery dominance is determined by the origin of the atrioventricular nodal artery at the crux of the heart (see above). The atrioventricular node artery originates from the RCA in approximately 90% of the population and LCx coronary artery in the remaining 10%. The dominant coronary artery also gives off the posterior descending coronary artery that runs in the posterior interventricular sulcus and provides septal perforator branches to the posterior one third of the interventricular septum. In some individuals, both the RCA and the LCx reach the crux and jointly give rise to the posterior descending coronary artery. In such cases, the coronary arterial system is referred to as codominant.
Variations in normal coronary artery anatomy
Absence of the left main coronary artery with separate origin of the LAD and LCx coronary arteries from the left coronary sinus of the aorta has been described in roughly 1% of patients undergoing angiography and is considered a normal variant. [1] In addition, one or more infundibular (conal) arteries may arise from separate ostia in the aorta. As many as 5 separate conal artery ostia have been reported in otherwise normal hearts. [7] Minor variations in the location of ostia within the coronary sinuses of the aorta are observed frequently and are of no clinical significance. A variation in normal coronary artery anatomy is shown below.
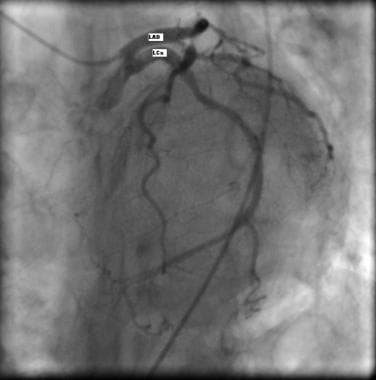 Coronary angiography showing separate origin of the left anterior descending (LAD) and left circumflex (LCx) coronary arteries from the left coronary sinus of the aorta (absent left main).
Coronary angiography showing separate origin of the left anterior descending (LAD) and left circumflex (LCx) coronary arteries from the left coronary sinus of the aorta (absent left main).
Anomalous coronary arteries
The list below presents a classification of major isolated coronary artery anomalies. As seen, coronary artery anomalies may involve abnormalities of number, origin and/or course, termination, or structure of the epicardial coronary arteries.
Normal variations include the following:
-
Absent left main (separate origin of LAD and LCx from the left coronary sinus)
-
Minor variations in position of ostia within the coronary sinus
-
Separate origin of conal branches
Abnormal numbers includes the following:
-
Duplication of the LAD
-
Duplication of the RCA (single or double ostium)
Anomalous origins include the following:
-
Origin from pulmonary trunk
-
Origin from left/right ventricle
-
Origin from bronchial/internal mammary/subclavian/right carotid/innominate artery
-
High takeoff (>1 cm above sinotubular junction)
Anomalous origins include the following:
-
Solitary ostium: (1) From right coronary sinus (RCA continues as LCx and LAD, RCA gives off LM, RCA gives off LAD and LCx) and (2) From left coronary sinus (LM gives off LAD, LCx, and RCA, LCx continues as RCA, LCx gives off RCA, LAD gives off RCA)
-
Origin of LAD from RCA
-
Origin of LCx from RCA
-
Origin of LAD from right coronary sinus
-
Origin of LCx from right coronary sinus
-
Origin of RCA from left coronary sinus
Anomalous courses includes the anomalous artery which takes 1 of 4 aberrant pathways, as follows:
-
A ( A nterior to right ventricular outflow tract)
-
B ( B etween aorta and pulmonary trunk)
-
C (Through the Crista supraventricularis)
-
D ( D orsal to the aorta)
Anomalous courses also include the following:
-
Intramyocardial course (myocardial bridging)
-
Tangential proximal course within the wall of the aorta
Anomalous terminations include the following:
-
Fistulas to right/left ventricle
-
Fistulas to right/left atrium
-
Fistulas to coronary sinus
-
Fistulas to pulmonary artery
Abnormal coronary structures include the following:
-
Stenosis
-
Atresia
-
Hypoplasia
The following section provides more detailed discussion of the above.
Abnormal number
In some individuals, certain left ventricular territories may be supplied by more than one coronary artery. Duplications of the LAD coronary artery, LCx coronary artery, and RCA have been reported.
Dual LAD coronary artery
Dual LAD coronary artery [8] consists of one short and another long artery and has been classified into several different subtypes.
In the most common form (type I), the short and long LAD coronary arteries originate from the normal LAD coronary artery proper. The shorter artery then runs in the anterior interventricular sulcus and terminates abruptly long before reaching the apex. The longer artery, however, runs on the anterior epicardial surface of the left ventricle and returns to the anterior interventricular sulcus in its distal one third and then continues on to the apex. All diagonal branches originate from the longer artery.
In the type II variety, the long LAD coronary artery courses over the anterior surface of the right rather than the left ventricle.
In the type III dual LAD coronary artery, the long artery has, at least partly, an intramyocardial (bridging) course. Unlike types I and II, the septal perforators arise from the long LAD and the diagonals arise from the short LAD coronary artery.
In the type IV variety, the short LAD coronary artery arises from the LM coronary artery and the long artery anomalously arises from the RCA and courses to the left side anterior to the right ventricular outflow tract.
In relatively recent years, with the more widespread use of coronary computed tomographic angiography (CTA), additional variations of dual LAD have been described. In one report, a variant of type IV was detailed in where the anomalous long LAD originated independently from the right coronary sinus and reached the distal anterior interventricular sulcus by coursing through the crista supraventricularis portion of the setum (type V). [9]
Duplications of the RCA
Duplications of the RCA [10, 11] have been reported with both single and double ostium in the right coronary sinus. The duplicate vessels may course together in the right atrioventricular groove and/or have separate courses with one coursing on the epicardial surface of the right ventricle. Both vessels give rise to right ventricular branches and generally 1 of the 2 gives off the posterior descending coronary artery.
We have reported duplication of the LCx, [12] or otherwise described as aberrant origin of one OM branch from the LAD, ramus intermedius, or diagonal branch of the LAD, in a case series of 24 patients. In the image below, the anomalous OM courses parallel to the LCx coronary artery and supplies blood to the acute margin of the left ventricle.
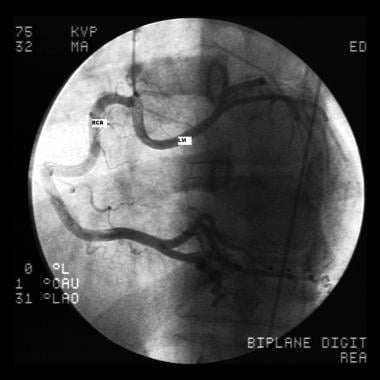 Coronary angiography showing the anomalous origin of the left main (LM) coronary artery from proximal right coronary artery (RCA) with subsequent retroaortic (dorsal [type D]) course to the left side.
Coronary angiography showing the anomalous origin of the left main (LM) coronary artery from proximal right coronary artery (RCA) with subsequent retroaortic (dorsal [type D]) course to the left side.
Anomalous origin
Abnormalities of the origin of coronary arteries with subsequent normal epicardial course relate to the anomalous location of one or both coronary ostia. These include the origin of LM, LAD, LCx, or RCA from the pulmonary trunk. [1] In addition, coronary arteries may originate directly from the left or right ventricles; the bronchial, internal mammary, subclavian, right carotid, or innominate arteries; the aortic arch; or the descending thoracic aorta. [1] High takeoff of the left or right coronary ostia, defined as the location of the ostium of the left or right coronary artery more than 1 cm above the sinotubular junction, has been described. [13, 14] See the images below.
 Selective left coronary artery angiogram demonstrating anomalous origin of obtuse marginal (OM) coronary artery from proximal left anterior descending (LAD) coronary artery. LM=left main, LCx=left circumflex.
Selective left coronary artery angiogram demonstrating anomalous origin of obtuse marginal (OM) coronary artery from proximal left anterior descending (LAD) coronary artery. LM=left main, LCx=left circumflex.
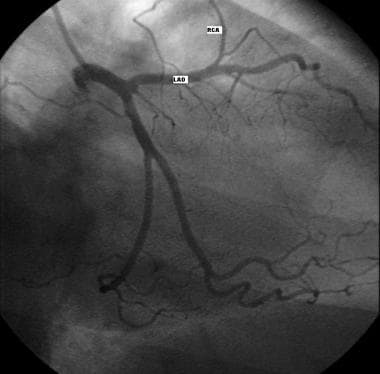 Coronary angiography showing the anomalous origin of the right coronary artery (RCA) from the left anterior descending (LAD) coronary artery with subsequent anterior course (anterior [type A]) to the right atrioventricular groove.
Coronary angiography showing the anomalous origin of the right coronary artery (RCA) from the left anterior descending (LAD) coronary artery with subsequent anterior course (anterior [type A]) to the right atrioventricular groove.
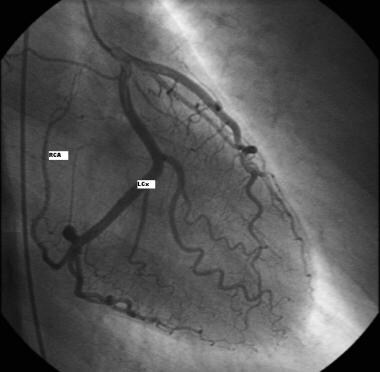 Coronary angiography showing the origin of the right coronary artery (RCA) as the continuation of the left circumflex (LCx) coronary artery.
Coronary angiography showing the origin of the right coronary artery (RCA) as the continuation of the left circumflex (LCx) coronary artery.
Anomalous origin and course
Single coronary artery
The entire coronary artery system may originate from a single ostium (solitary coronary ostium or single coronary artery) in the aorta. This solitary ostium is either located in the left or right coronary sinus of the aorta. When the LM coronary artery originates from the proximal RCA, or vice versa, the anomalous artery takes 1 of 4 aberrant pathways to reach its proper vascular territory. These pathways are designated as type A (A nterior to the right ventricular outflow tract), type B (B etween the aorta and pulmonary trunk), type C (C ristal, coursing through the crista supraventricularis portion of the septum), and type D (D orsal or posterior to the aorta). [15]
Single coronary arteries may also include the separate origin of the LAD and LCx coronary arteries from the proximal RCA. In this case, the LAD coronary artery takes one of the type A, B, or C pathways, and the LCx coronary artery takes either the B or D pathway. The LCx coronary artery may also originate from the distal RCA. In that case, the LCx coronary artery is merely a continuation of the RCA in the posterior atrioventricular groove. Overall, a total of 20 possible variations of single coronary artery have been described. [16]
Origin from opposite coronary sinus
Both the left and right coronary arteries may arise from separate ostia located in the same, either left or right, sinus of the aorta. In such cases, the anomalous vessels take 1 of the 4 possible courses to reach their proper territories similar to what was described above for the single coronary artery (types A-D). [17] In the absence of congenital heart disease, anomalous origin of coronary arteries from noncoronary sinus is not reported. [18]
Anomalous course
Otherwise normal coronary arteries may have an intramyocardial course (ie, myocardial bridge). This particular abnormality involves a variable length of the vessel and is observed most commonly in the proximal portion of the LAD coronary artery. [1]
Anomalous termination
Major epicardial coronary arteries may terminate abnormally into one of the cardiac chambers, the coronary sinus, or the pulmonary trunk and, thus, produce fistulas. These fistulas can originate from the left coronary artery system (50-60%), right coronary artery system (30-40%), or both (2-5%). Most fistulas (90%) drain into the right heart. [1]
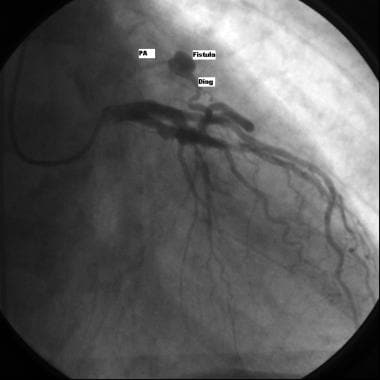 Coronary angiography showing the presence of a fistula originating from a diagonal (diag) branch of the left anterior descending coronary artery with anomalous communication with the pulmonary artery (PA).
Coronary angiography showing the presence of a fistula originating from a diagonal (diag) branch of the left anterior descending coronary artery with anomalous communication with the pulmonary artery (PA).
Abnormal coronary structure
Both congenital stenosis and atresia of the coronary arteries have been described. [1] Congenital epicardial coronary artery stenosis is usually caused by a membrane or a fibrotic ridge. Coronary artery atresia is characterized by the presence of an ostial dimple in the left or right aortic sinus that terminates in a cordlike fibrotic structure without a patent lumen. Atresia may also involve individual major epicardial coronary arteries. Hypoplastic coronary arteries have small luminal diameter (usually < 1 mm) and reduced length. [1] The latter is often associated with the absence of the posterior descending coronary artery.
Epidemiology
United States data
Coronary artery anomalies are observed in 0.3-1.3% of patients undergoing diagnostic coronary angiography, in approximately 1% of routine autopsy examinations, and in 4-15% of young people who experience sudden death. In the general population, the incidence of a single coronary artery is approximately 0.024%, whereas coronary artery fistulas are found in 0.2% of patients undergoing coronary angiography. Coronary artery fistulas are present in 0.002% of all patients with congenital heart disease. Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is reported in 0.0003% of the general population. This anomaly is responsible for 18% of all cases of congestive heart failure in children younger than 2 years.
Sex- and age-related demographics
No differences have been reported in incidence of specific coronary artery anomalies among male and female subjects.
Origin of left main coronary artery from the pulmonary trunk manifests during early infancy. Other significant coronary anomalies usually result in symptoms during young adult life. The remaining anomalies generally are clinically silent and may be discovered incidentally during noninvasive or invasive diagnostic testing for unrelated symptoms. [19, 20]
Prognosis
Most coronary artery anomalies are clinically silent and do not affect the outcome of patients. Certain anomalies are associated with sudden death, myocardial ischemia (including acute myocardial infarction [21] ), congestive heart failure, or endocarditis at an early age.
Morbidity/mortality
Most coronary artery anomalies are clinically silent and do not affect the quality of life or life span of the affected individuals. Specific forms of anomaly, such as the origin of the left main coronary artery from the pulmonary trunk, the aberrant course of the arteries between the great vessels in association with anomalous and slitlike ostium, and large coronary artery fistulas, may be associated with sudden death, myocardial ischemia, congestive heart failure, or endocarditis. Hypoplastic coronary arteries and high take-off of coronary ostia have been occasionally reported to have been associated with sudden death. The exact incidence of these associated clinical events is not known. [1, 2, 3, 4, 5]
A study by Krupinski et al indicated that the incidence of high-risk coronary artery features tends to be greater in association with an anomalous origin of the right, rather than left, coronary artery. The study included more than 50 patients diagnosed by computed tomography (CT) scanning with an abnormal origin of the right (16 patients), left (13 patients), or left circumflex (22 patients) coronary artery. Although 15 of the right coronary artery patients had a slitlike orifice, only three patients total in the other two groups had this feature. [22]
In addition, 15 of the right coronary artery patients had an intramural course, compared with three total in the other two groups, and whereas 11 of the right coronary artery patients had an interarterial course, none of the other patients did. Moreover, only 3 patients in the left coronary artery group presented with chest pain, compared with 25 patients total in the right and circumflex coronary artery groups. The investigators also found that five of the right coronary artery patients experienced cardiac events during follow-up, compared with four total in the left and circumflex coronary artery groups. [22]
Etiology
The exact pathogenetic mechanisms for development of congenital coronary artery anomalies are not well understood. According to extensive embryologic studies, formation of a normal coronary arterial system depends on multiple morphologic features, including formation of cardiac sinusoids, development of coronary buds on embryologic aortopulmonary trunk, and selective connection between the two systems. Any malformation within these systems may lead to development of coronary artery anomalies.
Congenital heart diseases
Some congenital heart diseases are found in association with coronary artery anomalies. These associations are especially strong in the following:
-
Truncus arteriosus, single coronary artery, and anterior coronary trunk crossing the outflow tract of the right ventricle
-
Transposition of the great arteries and ectopic origin of coronary ostia
-
Pulmonary valve atresia with intact ventricular septum and solitary coronary artery or coronary artery fistula draining into the right ventricle
-
Double outlet right ventricle and unpredictable coronary anatomy
-
Isolated aortic valve anomalies (such as bicuspid aortic valve) and ectopic origin of ostia, left coronary artery dominance, high takeoff of the left coronary artery, and shortening of the left main trunk
-
Tetralogy of Fallot and ectopic origin of the coronary arteries or coronary artery fistula draining into the pulmonary trunk
Familial clustering
Isolated reports of specific coronary artery anomalies occurring in family members have been reported. However, to date, no definitive data on coronary inheritance pattern have been reported in humans. [23]
-
Coronary angiography showing separate origin of the left anterior descending (LAD) and left circumflex (LCx) coronary arteries from the left coronary sinus of the aorta (absent left main).
-
Coronary angiography showing the anomalous origin of the left main (LM) coronary artery from proximal right coronary artery (RCA) with subsequent retroaortic (dorsal [type D]) course to the left side.
-
Selective left coronary artery angiogram demonstrating anomalous origin of obtuse marginal (OM) coronary artery from proximal left anterior descending (LAD) coronary artery. LM=left main, LCx=left circumflex.
-
Coronary angiography showing the anomalous origin of the right coronary artery (RCA) from the left anterior descending (LAD) coronary artery with subsequent anterior course (anterior [type A]) to the right atrioventricular groove.
-
Coronary angiography showing the origin of the right coronary artery (RCA) as the continuation of the left circumflex (LCx) coronary artery.
-
Coronary angiography showing the presence of a fistula originating from a diagonal (diag) branch of the left anterior descending coronary artery with anomalous communication with the pulmonary artery (PA).





