Practice Essentials
Large-bowel obstruction (LBO) is an emergency condition that requires early identification and intervention. It is important to distinguish colonic obstruction from ileus, as well as to distinguish true mechanical obstruction from pseudo-obstruction; treatment differs. See the image below.
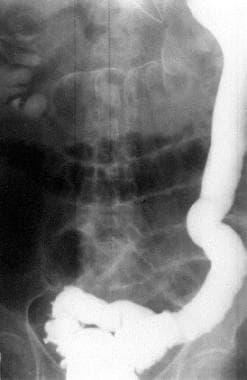 Large-Bowel Obstruction. Contrast study demonstrates colonic obstruction at the level of the splenic flexure, in this case due to carcinoma. Radiograph courtesy of Charles J McCabe, MD†.
Large-Bowel Obstruction. Contrast study demonstrates colonic obstruction at the level of the splenic flexure, in this case due to carcinoma. Radiograph courtesy of Charles J McCabe, MD†.
See Can't-Miss Gastrointestinal Diagnoses, a Critical Images slideshow, to help diagnose the potentially life-threatening conditions that present with gastrointestinal symptoms.
Signs and symptoms
A history of bowel movements, flatus, obstipation, and associated symptoms should be obtained. Complaints in patients with LBO may include the following:
-
Abdominal distention
-
Nausea and vomiting
-
Crampy abdominal pain
Other symptoms that may be diagnostically significant include the following:
-
Abrupt onset of symptoms (suggestive of an acute obstructive event)
-
Chronic constipation, long-term cathartic use, and straining at stools (suggestive of diverticulitis or carcinoma)
-
Changes in stool caliber (strongly suggestive of carcinoma)
-
Recurrent left lower quadrant abdominal pain over several years (suggestive of diverticulitis, a diverticular stricture, or similar problems)
Assessment of symptoms should attempt to distinguish the following:
-
Complete obstruction vs partial obstruction vs ileus
-
Colonic lesion development history
-
Obstruction secondary to intussusception
-
Obstruction secondary to acute colonic pseudo-obstruction (ACPO), or Ogilvie syndrome
Although a complete physical examination is necessary, the examination should place special emphasis on the following key areas:
-
Abdomen (inspection, auscultation, percussion, and palpation): Evaluate bowel sounds, tenderness, rigidity, guarding, and any mass or fullness
-
Inguinal and femoral regions: In particular, look for a possible incarcerated hernia
-
Rectum: Assess anal patency (in a neonate), contents of anal vault, and stool consistency; perform fecal occult blood testing as appropriate
See Presentation for more detail.
Diagnosis
The following laboratory studies may be helpful:
-
Complete blood count (CBC)
-
Hematocrit
-
Prothrombin time (PT)
-
Type and crossmatch
-
Serum chemistries
-
Serum lactate (if bowel ischemia is a consideration)
-
Urinalysis
-
Stool guaiac test
Imaging modalities that may be considered are as follows:
-
Plain radiography (flat and upright)
-
Contrast radiography with enema
-
Computed tomography (CT): This is the imaging modality of choice if a colonic obstruction is clinically suspected; contrast-enhanced CT can help distinguish between partial and complete obstruction, ileus, and small-bowel obstruction
See Workup for more detail.
Management
Initial therapy in patients with suspected LBO includes the following:
-
Volume resuscitation
-
Appropriate preoperative broad-spectrum antibiotics
-
Timely surgical consultation
-
Consideration of a nasogastric tube for severe colonic distention and vomiting
The following are emergencies that call for surgical intervention:
-
Closed loop obstructions
-
Bowel ischemia
-
Volvulus
Ileus is treated as follows:
-
Correction of fluid and electrolyte imbalances
-
Treatment of the underlying disorder
-
If the patient is vomiting, nasogastric decompression
-
Cessation of medications that slow colonic motility, if possible
Acute colonic pseudo-obstruction is treated as follows:
-
In the absence of perforation, conservative management (bowel rest, hydration, and management of underlying disorders) for the first 24 hours
-
If conservative management fails, neostigmine or colonoscopic decompression
-
For refractory cases or in the presence of perforation, surgical intervention
Volvulus is treated as follows:
-
For a sigmoid volvulus, in the absence of peritoneal signs, endoscopic reduction and decompression
-
For recurrence after decompression, surgical resection
-
For cecal or transverse colon volvulus, surgical resection and anastomosis; for poor surgical candidates, endoscopic detorsion and decompression
Intussusception is treated as follows:
-
Contrast enema (barium or air; much more likely to succeed in children than in adults)
-
If signs suggest peritonitis or perforation or contrast enema is unsuccessful, surgery
Colonic masses and strictures are treated as follows:
-
Endoscopic dilation and stenting of colonic obstruction (either as palliation or as preparation for surgical resection)
-
Surgery (left colon): Resection without primary anastomosis or resection with primary anastomosis and intraoperative lavage
-
Surgery (right colon): Right colectomy and primary anastomosis between the ileum and the transverse colon
Diverticular disease is treated as follows:
-
For persistent obstruction despite appropriate medical management, surgery
-
For recurrent disease, elective colonic resection
See Treatment and Medication for more detail.
Background
Large-bowel obstruction (LBO) is an emergency condition that requires early identification and intervention. The etiology of this condition is age-dependent, and it can result either from mechanical interruption of the flow of intestinal contents (see the following image) or from dilatation of the colon in the absence of an anatomic lesion (pseudo-obstruction). Causes include neoplasms, inflammatory processes (diverticulitis), strictures, fecal impaction or volvulus.
 Large-Bowel Obstruction. Abdominal (kidney-ureter-bladder [KUB]) film of a patient with obstipation. Dilatation of the colon is associated with large-bowel obstruction. Radiograph courtesy of Charles J McCabe, MD†.
Large-Bowel Obstruction. Abdominal (kidney-ureter-bladder [KUB]) film of a patient with obstipation. Dilatation of the colon is associated with large-bowel obstruction. Radiograph courtesy of Charles J McCabe, MD†.
It is important to distinguish colonic obstruction from ileus and to differentiate between true mechanical obstruction and pseudo-obstruction. Treatment differs. [1]
Colonic obstruction is more common in elderly individuals as a consequence of the higher incidence of neoplasms and other causative diseases in this population. [2] In neonates, colonic obstruction may be caused by an imperforate anus or other anatomic abnormalities. Obstruction may also be secondary to meconium ileus. In the pediatric population, Hirschsprung disease can resemble colonic obstruction.
See also Ogilvie Syndrome, Ileus, Constipation, Small Bowel Obstruction, and Intussusception.
Pathophysiology
The prevalence of mechanical large-bowel obstruction (LBO) increases with age, as does that of its main causes, colon cancer and diverticulitis. Sigmoid volvulus and cecal volvulus are also potential causes of this disorder. [3]
Mechanical LBO causes bowel dilatation above the obstruction, which in turn, causes mucosal edema and impaired venous and arterial blood flow to the bowel. Bowel edema and ischemia increase the mucosal permeability of the bowel, which can lead to bacterial translocation, systemic toxicity, dehydration, and electrolyte abnormalities. Bowel ischemia can lead to perforation, fecal soilage of the peritoneal cavity, and dead bowel.
In cases of closed loop obstructions, such as colonic obstruction in the presence of a closed ileocecal valve or incarcerated hernia, this process may be accelerated.
The pathophysiology of acute colonic pseudo-obstruction (ACPO), or Ogilvie syndrome, is not clear, but it is thought to result from an autonomic imbalance, which results from decreased parasympathetic tone or excessive sympathetic output. [1, 4] This condition usually occurs in the setting of a wide range of medical or surgical illnesses. If it goes untreated, colonic ischemia or perforation can occur. ACPO is characterized by a loss of peristalsis and results in the accumulation of gas and fluid in the colon. The right colon and cecum are most commonly involved. The risk of perforation for ACPO ranges from 3% to 15%. [5]
Etiology
The most common causes of large-bowel obstructions (LBO) are colon carcinoma and volvulus. [6] Approximately 60% of mechanical LBOs are caused by malignancies, 20% are caused by diverticular disease, and 10% are the result of colonic volvulus. [1, 7, 8] The most common causes of adult large-bowel obstruction are as follows:
-
Neoplasm (benign or malignant)
-
Stricture (diverticular or ischemic)
-
Volvulus (colonic, sigmoid, cecal)
-
Intussusception, usually with an identifiable anatomic abnormality in adults but not in children
-
Impaction or obstipation
Uncommon causes of LBOs include inflammatory bowel disease, hernia, adhesion, endometriosis, [9] intussusception, and functional disorders of the colon. [10]
Neoplasms and diverticular disease
Obstructions caused by tumors tend to have a gradual onset and result from tumor growth narrowing the colonic lumen.
Diverticulitis is associated with muscular hypertrophy of the colonic wall. Repetitive episodes of inflammation cause the colonic wall to become fibrotic and thickened, leading to luminal narrowing.
Volvulus
A colonic volvulus results when the colon twists on its mesentery, which impairs the venous drainage and arterial inflow. Symptoms of this condition are usually abrupt. The cecum and sigmoid colon are most commonly affected.
Volvulus typically occurs in elderly, debilitated individuals; patients living in an institutionalized setting; or patients with a history of chronic constipation. Volvulus may also be seen during pregnancy, most commonly occurring in the third trimester when the gravid uterus displaces the colon. [11]
Intussusception
Intussusception is primarily a pediatric disease; however, it is estimated that 5-16% of all intussusceptions in the Western world occur in adults. Two thirds of adult intussusception cases are caused by tumors. Two main types of intussusception affect the large bowel: enterocolic and colocolic.
Enterocolic intussusceptions involve both the small bowel and the large bowel. These are composed of either ileocolic intussusceptions or ileocecal intussusceptions, depending on where the lead point is located.
Colocolic intussusceptions involve only the colon. They are classified as either colocolic or sigmoidorectal intussusceptions.
Acute colonic pseudo-obstruction (Ogilvie syndrome)
ACPO (Ogilvie syndrome) has many etiologies. ACPO is a functional obstruction; it is typically seen in elderly or debilitated patients who are hospitalized with severe medical or traumatic illnesses. Medications that decrease intestinal motility are also associated with this disorder. In a retrospective review of more than 1400 cases of ACPO, the most common predisposing conditions were operative and nonoperative trauma (11%), infections (10%), and cardiac disease (10-18%). [12, 13]
Prognosis
Mortality is determined by the patient's overall medical condition and the presence of any comorbidities that may influence the patient's surgical risk. If large bowel obstruction is treated early, the outcome is generally good. Mortality is higher in patients who have developed bowel ischemia or perforation. After surgical decompression, the prognosis is determined by the underlying disease. In general, overall mortality for large-bowel obstruction is 20%, which increases to 40% if there is colonic perforation.
Mortality for acute colonic pseudo-obstruction (ACPO; Ogilvie syndrome) is 15% with early care; it increases to 36% if colonic ischemia or perforation develops. [5]
In a retrospective study, long-term outcomes of self-expandable metallic stenting for malignant colorectal obstruction in 42 elderly patients were excellent (97.6%), with shorter stents yielding longer event-free survival. [14]
-
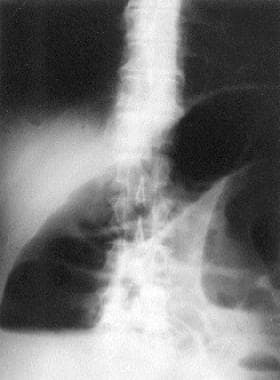
Large-Bowel Obstruction. This chest radiograph demonstrates free air under the diaphragm, indicating bowel perforation in a patient with large-bowel obstruction. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Abdominal (kidney-ureter-bladder [KUB]) film of a patient with obstipation. Dilatation of the colon is associated with large-bowel obstruction. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Gastrografin study in a patient with obstipation reveals colonic obstruction at the rectosigmoid level. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Contrast study demonstrates colonic obstruction at the level of the splenic flexure, in this case due to carcinoma. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Abdominal (kidney-ureter-bladder [KUB]) radiograph depicting massive dilatation of the colon due to a cecal volvulus. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Contrast study of patient with cecal volvulus. The column of contrast ends in a "bird's beak" at the level of the volvulus. Radiograph courtesy of Charles J McCabe, MD†.
-
Large-Bowel Obstruction. Massive dilatation of the colon due to a sigmoid volvulus. Radiograph courtesy of Charles J McCabe, MD†.









