Practice Essentials
Human metapneumovirus (hMPV) is a non-segmented single negative-stranded RNA-enveloped virus classified in the Pneumovirinae subfamily of the Paramyxoviridae family. hMPV infection has clinical features that range from mild upper respiratory tract infections (URTIs) to lower respiratory tract infections (LRTIs) complicated by significant wheezing, leading to life-threatening bronchiolitis and pneumonia, in all age groups. This virus is second only to the respiratory syncytial virus (RSV) as the most commonly identified cause of pediatric LRTI.
Signs and symptoms
Infection with hMPV causes a broad spectrum of respiratory illness, from mild symptoms to severe cough, bronchiolitis, and pneumonia. The clinical symptoms are similar to those seen with RSV infection and may also include the following:
-
Fever
-
Cough
-
Rhinorrhea
-
Dyspnea, tachypnea, chest retraction and wheezing
Bronchiolitis, with or without pneumonia, is the most common presentation of hMPV illness. Other reported syndromes have included the following [1, 2, 3, 4, 5, 6, 7] :
-
Asthma exacerbation
-
Otitis media
-
Pneumonitis
-
Flulike illness
-
Community-acquired pneumonia
-
COPD (chronic obstructive pulmonary disease) exacerbation
See Clinical Presentation for more detail.
Diagnosis
Laboratory testing
-
Quantitative reverse-transcriptase polymerase chain reaction of respiratory secretions: This is the most sensitive method for hMPV diagnosis; also useful to quantify viral load in research settings
-
Enzyme-linked immunoassay (ELISA): Note that seropositivity is nearly universal after early childhood, making definitive serologic diagnosis reliant on seroconversion or a 4-fold titer increase on serial samples
-
Immunofluorescence testing
-
Rapid antigen test using lateral-flow immunochromatography with gold colloid-conjugated hMPV antibodies less sensitive test (70.6% sensitivity and 95.5% specificity)
It is difficult to grow hMPV in cell culture; therefore, this is method is no longer a timely mode of diagnosis. Isolation is possible in a limited number of cell lines and requires trypsin supplementation.
Imaging studies
Chest radiography is generally not helpful. Findings in patients with significant lower respiratory tract disease are indistinguishable between hMPV and other causes of viral pneumonia or bronchiolitis. Immunosuppressed persons, such as stem cell transplant or organ transplant recipients, may require CT scanning to clarify upper respiratory versus lower respiratory infection.
See Workup for more detail.
Management
There is no specific antiviral therapy available for hMPV infection; therefore, most treatment is supportive. Hospitalization, supplemental oxygen, and mechanical ventilation may be necessary in severe hMPV infections. In severely immunosuppressed persons, oral, inhaled or IV ribavirin can be considered. [8, 9, 50]
See Treatment and Medication for more detail.
Background
Human metapneumovirus (hMPV), like human respiratory syncytial virus (RSV), is classified in the Pneumovirinae subfamily of the Paramyxoviridae family. However, hMPV is most closely genetically related to avian metapneumovirus (formerly called turkey rhinotracheitis virus). These two viruses are classified in the genus Metapneumovirus, with hMPV the first in this genus to cause disease in humans. Although it is hypothesized that the human virus originated from birds, the serological evidence that hMPV has been widespread in humans since at least 1958 suggests a zoonotic divergence before this time. [8, 10]
hMPV was first described in 2001 by researchers in the Netherlands. hMPV was identified in stored nasopharyngeal samples from children with respiratory illness using reverse transcription-polymerase chain reaction (RT-PCR) amplification techniques. [8] Genome had 88% homology with avian metapneumovirus serotype C, able to replicate in monkeys but not in birds. [8] Since this initial report, hMPV has been identified in countries on all continents except Antarctica.
hMPV is a non-segmented, single negative-stranded RNA-enveloped virus with 2 antigenically distinct groups: A and B, that further subdivided into 5 sublineages (or clades) based on G and F gene variations: A1, A2a, A2b, B1, and B2. [56, 51]
Phylogenetic tree showing sequence analysis of human metapneumovirus (hMPV)
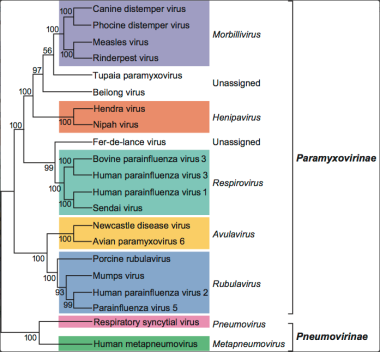 Phylogenetic analysis of the L-proteins of members of the family Paramyxoviridae. Courtesy of ICTV 9th Report on Virus Classification and Taxon Nomenclature (2011) [https://talk.ictvonline.org/ictv-reports/ictv_9th_report/negative-sense-rna-viruses-2011/w/negrna_viruses/200/paramyxoviridae-figures].
Phylogenetic analysis of the L-proteins of members of the family Paramyxoviridae. Courtesy of ICTV 9th Report on Virus Classification and Taxon Nomenclature (2011) [https://talk.ictvonline.org/ictv-reports/ictv_9th_report/negative-sense-rna-viruses-2011/w/negrna_viruses/200/paramyxoviridae-figures].
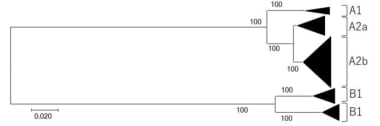 Phylogenetic tree of human metapneumovirus (hMPV) strains. Courtesy of Microorganisms [Nao N, Saikusa M, Sato K, et al. Recent Molecular Evolution of Human Metapneumovirus (HMPV): Subdivision of HMPV A2b Strains. Microorganisms. 2020 Sep;8(9):1280. Online at: https://www.mdpi.com/2076-2607/8/9/1280.].
Phylogenetic tree of human metapneumovirus (hMPV) strains. Courtesy of Microorganisms [Nao N, Saikusa M, Sato K, et al. Recent Molecular Evolution of Human Metapneumovirus (HMPV): Subdivision of HMPV A2b Strains. Microorganisms. 2020 Sep;8(9):1280. Online at: https://www.mdpi.com/2076-2607/8/9/1280.].
Pathophysiology
Data on hMPV pathophysiology based on human studies have been reported. Two prospective studies from Argentina have quantified cytokine levels in nasal washes taken from subjects with hMPV infection and compared these with cytokine levels in RSV and influenza. They found that hMPV infection produces a low level of innate and adaptive cytokine response, although with a greater bias toward a Th2 response than the comparator viruses. [12, 13]
Multiple animal models have been used to study the pathophysiology of hMPV. Chimpanzees have been the only animal to demonstrate symptomatology consistent with human disease. [14] However, respiratory tract viral replication of hMPV has been demonstrated in cynomolgus macaques, cotton rats, and BALB/c mice, in addition to other small rodents. [15, 16, 17, 18]
Studies of cytokine response in BALB/c mice have shown findings that are consistent with those of the human studies cited above, showing a weak innate cytokine response that corresponds with lower levels of pulmonary inflammation than with RSV infection. [19]
Studies of cellular immune responses to hMPV in mice demonstrated the importance of CD4+ regulatory T cells (Treg) at different time points. Treg depletion before hMPV infection leads to a reduction of hMPV-specific CD8+ T cells and delay virus clearance due to shifting of the immune response towards cytokine production and increasing of CD4+ T cell. Contrary, in mice with Treg depletion 2 days since inoculation, a number of hMPV-specific CD8+ T cells was the same but with stronger functioning, emphasizing the crucial role of priming the adaptive immune response to hMPV infection. [57]
Studies on viral time course in an experimental mouse model of hMPV infection demonstrate a peak of viral titers between day 3 to day 14 after hMPV infection. [58] While most models show clearance of the virus by postinfection day 10-14, some studies report shedding of hMPV up to 180 days in BALB/c mice following infection. The significance of this viral persistence in relation to human disease is unknown. [18, 20]
Two recent studies have examined the significance of hMPV viral load, as assessed by real-time PCR, on illness parameters. One study showed that increased viral loads correlated with lower respiratory tract illness and hospitalization. [21] Another study found that an increasing viral load was associated with increased fever, increased bronchodilator use, and increased length of hospitalizations, independent of age and underlying chronic illness. This study also evaluated viral loads in RSV illness and did not find this same correlation with disease severity, suggesting a different pathology mechanism between these two related viruses. [22]
hMPV induces weak memory response due to poor T and B cell memory immunity. The possible mechanism of weak memory response is the insufficient activation of naive CD4+ T cells due to secretion of soluble molecules by an hMPV-infected dendritic cell that down-modulate T-cell activation. [59] Therefore, reinfection is possible throughout life. [60]
Epidemiology
hMPV is considered ubiquitous. This belief is based on the widespread detection of infection, as well as the high prevalence of antibodies against the virus in all age groups. Seroconversion typically occurrs during the first 24 months after weaning of maternal antibodies. By age 24 months, 52% of children had detected hMPV antibodies. [62] In children 2 to 5 years seropositivity reaching 80%. [63, 24] By age 10 years and older, 100% of patients were seropositive. [8, 23, 24] Reinfection of hMPV is common throughout life with equal rates as initial infection. [64]
The incubation period may vary but averages between 3 and 5 days from exposure. [51] hMPV is detected throughout the year, with a peak incidence from late winter to early spring, later than the seasonal peak of RSV and influenza during the entire period studied. In the northern hemisphere, the hMPV peak tends to be from January to March; in the southern hemisphere, the peak is from June to July. [51] An increase in the incidence of hMPV is reported with increasing distance from the equator. [65]
The largest 20 years of surveillance study showed that hMPV was detected by a real-time reverse-transcriptase polymerase chain reaction in up to 5% of children with upper respiratory infections who were prospectively followed from birth until 5 years of age, with variation from year to year. [25] Other prospective, population-based surveillance studies in children < 5 years of age demonstrated that hMPV was detected in 6% of hospitalized children, 7% of children seen in ED, and 1% of asymptomatic controls. [68]
Many studies indicate that hMPV is the second most commonly identified cause of pediatric lower respiratory illness, behind only RSV. The proportion of hMPV in children with lower respiratory tract infection was reported at 8.9% in a prospective cohort study of children aged < 3 years in Peru. [70] In studies conducted in all age groups, results demonstrated that children and adults hospitalized with pneumonia had hMPV detected in 12.6% and 3.8%, respectively. [66] The same study reported codetection of hMPV with other pathogens in 42% in children and 24% in adults. In patients >50 years of age hospitalized with acute respiratory illness hMPV was detected in 4.5% of cases. [67]
hMPV infection was reported in high-risk adult populations, including those with chronic obstructive pulmonary disease (COPD), elderly patients, and immunocompromised patients. [1, 2, 3] Multiple outbreaks in healthcare facilities have been detailed in the literature, not only from infected residents but also from asymptomatic shedding of the virus in nonresidents. [54]
hMPV has been documented as a significant cause of illness in transplant recipients. Studies have linked hMPV with idiopathic pneumonia, fulminant respiratory failure, and high mortality rates in stem cell transplant recipients. [27, 28] Additionally, in one study, hMPV was found in 10% of lung transplant recipients with acute respiratory tract infections, similar to the rate of RSV detection. [29] Thus, transplant patients appear to be at significant risk for severe hMPV illness.
Mortality/Morbidity
Risk factors for severe hMPV disease appear to be similar to those for severe RSV disease and include prematurity, heart disease, pulmonary disease, immunocompromise, organ or stem cell transplantation. [27, 28, 4, 71] hMPV infection in lung transplant recipients can lead to permanent lung graft dysfunction and increased morbidity. [52]
Little is known about the sequelae of hMPV illness. However, a small study of premature infants infected with hMPV did show increased airway resistance at follow-up. [36]
-
Phylogenetic tree showing sequence analysis of human metapneumovirus (hMPV).
-
Phylogenetic tree of human metapneumovirus (hMPV) strains. Courtesy of Microorganisms [Nao N, Saikusa M, Sato K, et al. Recent Molecular Evolution of Human Metapneumovirus (HMPV): Subdivision of HMPV A2b Strains. Microorganisms. 2020 Sep;8(9):1280. Online at: https://www.mdpi.com/2076-2607/8/9/1280.].
-
Phylogenetic analysis of the L-proteins of members of the family Paramyxoviridae. Courtesy of ICTV 9th Report on Virus Classification and Taxon Nomenclature (2011) [https://talk.ictvonline.org/ictv-reports/ictv_9th_report/negative-sense-rna-viruses-2011/w/negrna_viruses/200/paramyxoviridae-figures].









