Practice Essentials
Prostate cancer is the most common noncutaneous cancer in men, making the diagnosis and staging of this cancer of great medical and public interest. Although prostate cancer can be slow growing, the disease nonetheless accounts for more than 10% of cancer-related deaths in males, with 10s of thousands of men dying of prostate cancer each year (see the image below).
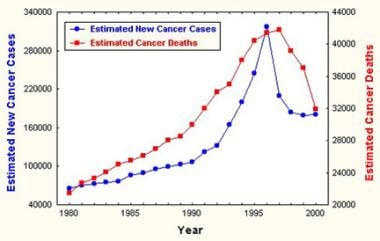 Estimated incidence of and mortality from prostate cancer. Courtesy of the American Cancer Society.
Estimated incidence of and mortality from prostate cancer. Courtesy of the American Cancer Society.
Screening controversies
Screening for prostate cancer, with prostate-specific antigen (PSA) evaluation and sometimes digital rectal examination (DRE), can detect asymptomatic cases and allow early diagnosis. However, there is controversy regarding screening.
Advocates of screening for prostate cancer believe that early detection is crucial to finding organ-confined disease and to reducing the likelihood of mortality. When symptoms develop or when DRE results become positive, most cases have already advanced beyond organ-confined disease. However, those who do not advocate screening worry that screening will detect cancers that are not biologically significant (ie, in patients who will die with prostate cancer rather than from it).
The American Cancer Society (ACS), [1] the American Urological Association (AUA), [2] and the National Comprehensive Cancer Network (NCCN), [3] have issued guidelines that differ on specific points but agree on the value of prostate cancer screening in selected populations, for patients who agree to screening after a discussion of the risks and benefits.
The U.S. Preventive Services Task Force (USPSTF) advises that in men aged 55 to 69 years, the decision of whether or not to undergo screening should be individualized. This is a grade C recommendation, meaning that there is at least moderate certainty that the net benefit is small. For men aged 70 years and older, the USPSTF recommends against PSA-based screening for prostate cancer. [4]
The European Society for Medical Oncology (ESMO) recommends against population-based PSA screening for prostate cancer on the grounds that it reduces prostate cancer mortality at the expense of overdiagnosis and overtreatment. [5]
Signs and symptoms
With the advent of PSA screening, patients with prostate cancer report the following local symptoms:
-
No symptoms (47%)
-
Urinary frequency (38%)
-
Urinary urgency (10%)
-
Decreased urine stream (23%)
-
Hematuria (1.4%)
Signs and symptoms of metastatic prostate cancer include the following:
-
Weight loss and loss of appetite
-
Bone pain, with or without pathologic fracture
-
Lower extremity pain and edema
-
Uremic symptoms
Diagnosis
Laboratory studies
-
PSA screening: Controversy exists regarding PSA level cutoffs and reference ranges
-
DRE: Serial examinations are best; clues to the patient’s condition in conjunction with PSA levels include presence of a nodule, as well as asymmetry, texture difference(s), and bogginess of the prostate, seminal vesicles, and adjacent organs
-
Biopsy and histologic examination: These aid in the diagnosis and help to determine the Gleason score; a biopsy can also help differentiate a cyst or calculus from cancer foci
Imaging studies
-
Computed tomography (CT) scanning: To assess extension into the bladder and lymph nodes for staging the cancer or for considering pretreatment lymph node sampling
-
Endorectal magnetic resonance imaging (MRI): To localize cancer within the prostate and seminal vesicles; to help in local staging
-
Bone scanning: To evaluate bone metastasis
-
MRI: To determine the etiology of questionable lesions found on bone scans
-
Transrectal ultrasonography: To examine the prostate for hypoechoic areas, which are commonly associated with cancers but are not specific enough for diagnostic purposes
Men with PSA levels above 10 ng/mL, high-grade histology (Gleason score of ≥7), or physical findings suggesting stage T3 disease should probably undergo a staging CT scan and bone scan. Neither CT scanning nor MRI can be used to determine if lymph nodes are reactive or contain malignant deposits, unless the nodes are significantly enlarged and a percutaneous biopsy can be performed.
Staging
Staging of prostate cancer is based on the following five key pieces of information [6] :
-
The extent of the primary tumor (T category)
-
Whether the cancer has spread to nearby lymph nodes (N category)
-
The absence or presence of distant metastasis (M category)
-
The PSA level at the time of diagnosis
-
The Grade Group, based on prostate biopsy (or surgery)
Overview
Since the adoption of widespread screening, prostate cancer is being diagnosed earlier in the disease course. Currently, most cases of prostate cancer are found because of abnormalities in a screening prostate-specific antigen (PSA) level or findings on digital rectal examination (DRE) rather than because of symptoms. In addition, prostate cancer can be an incidental pathologic finding when tissue is removed during transurethral resection to manage obstructive prostatic symptoms (see Benign Prostatic Hyperplasia [BPH]).
The American Cancer Society (ACS) estimated that 240,890 new cases of prostate cancer were diagnosed in the United States in 2011 and that 33,720 men died of the disease in that year. (See the chart below.) Comparable ACS estimates for 2023 are 288,300 new cases and 34,700 deaths. [7]
Estimated incidence of and mortality from prostate cancer. Courtesy of the American Cancer Society.
For more information, see the following:
Age- and race-related demographics
Prostate cancer is rarely diagnosed in men younger than 40 years, and it is uncommon in men younger than 50 years.
Prevalence rates of prostate cancer remain significantly higher in African-American men than in white men, while the prevalence in Hispanic men is similar to that of white men. Hispanic men and African-American men tend to present with more advanced disease, a situation that is most likely related to external (eg, income, education, insurance status) and cultural factors. In addition, African-American men generally have higher levels of testosterone, which may contribute to the higher incidence of carcinoma in that population. [8, 9]
Mutations that appear specific to, or more common in, African-American patients have been identified in aggressive prostate tumors. Further research will be needed to determine whether these mutations factor into the racial differences in incidence and clinical outcome that are seen in prostate cancer. [10, 11]
Differentials
Differential diagnoses of prostate cancer include the following:
-
Benign prostatic hyperplasia
-
Calculi
-
Prostatic cysts
-
Prostatic tuberculosis
-
Prostatitis
Patient education
Because of the advent of PSA screening, a greater number of men now require education about prostate cancer, including the risk of progression and how the disease is diagnosed, staged, and treated. A study by Hall et al found that 80% of primary care physicians discussed PSA screening with their male patients, with 64.1% encouraging the screening. [12]
For patient education information, see the Men's Health Center and the Cancer Center, as well as Prostate Cancer.
Relevant Anatomy
The prostate lies below the bladder and encompasses the prostatic urethra. It is surrounded by a capsule and is separated from the rectum by a layer of fascia termed the Denonvilliers aponeurosis. The position of the prostate in the male genitourinary tract is shown in the image below.
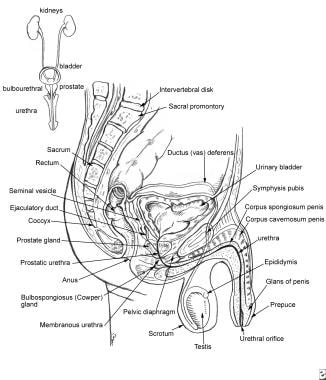
The blood supply to the base of the bladder and prostate is from the inferior vesical artery, which is derived from the internal iliac artery. The capsular branches of the inferior vesical artery help to identify the pelvic plexus arising from the S2-S4 and T10-T12 nerve roots.
The neurovascular bundle lies on either side of the prostate on the rectum. It is derived from the pelvic plexus and is important for erectile function.
Characteristics of Prostate Cancer
Ninety-five percent of prostate cancers are adenocarcinomas. In approximately 4% of men with prostate cancer, the neoplasm has transitional cell morphology and is thought to arise from the urothelial lining of the prostatic urethra.
In rare cases, the tumor has a neuroendocrine morphology; in such instances the neoplasm is believed to have arisen from the neuroendocrine stem cells that are normally present in the prostate or from aberrant differentiation programs during cell transformation.
Seventy percent of prostate cancers arise in the peripheral zone, 15-20% arise in the central zone, and 10-15% arise in the transition zone.
Screening Indications and Controversies
Prostate-specific antigen (PSA) measurement is an essential component of a modern screening program. Digital rectal examination (DRE) may also be performed.
The indications for screening are controversial. Advocates of screening believe that early detection is crucial to finding organ-confined disease and to reducing the likelihood of mortality. When symptoms develop or when DRE results become positive, most cases have already advanced beyond organ-confined disease. Those who do not advocate screening note that screening can detect cancers that are not biologically significant (ie, in patients who will die with prostate cancer rather than from it), and subject patients to the risks of unnecessary intervention.
The American Cancer Society (ACS) recommends that asymptomatic men with at least a 10-year life expectancy should be given an opportunity to make an informed decision with their health care provider after receiving information on the uncertainties, risks, and benefits of screening PSA evaluation. The recommended age at which men should receive this information varies by prostate cancer risk, as follows [1] :
-
Age 50 for those at average risk of developing prostate cancer
-
Age 45 for those at high risk, including African Americans and men with a first-degree relative (father, brother, son) diagnosed with prostate cancer before age 65
-
Age 40 for those at higher risk (more than one first-degree relative diagnosed with prostate cancer at an early age)
Men who decide to be screened should be tested with a PSA test. A DRE may also be done as a part of screening. If screening does not detect cancer, the time between subsequent screenings depends on the PSA results, as follows [1] :
-
< 2.5 ng/ml – Retesting may be done every 2 years
-
≥2.5 ng/ml – Retesting should be done annually
The National Comprehensive Cancer Network (NCCN) notes the importance of identifying aggressive prostate cancer while avoiding the detection of indolent disease. For men 45-75 years old at average risk, and men 40-75 years old at high risk, the NCCN recommends a discussion of screening risks and benefits, followed by a baseline PSA and consideration of a DRE, especially in men with an elevated PSA level. [3] Blacks/African Americans, men with germline mutations that increase the likelihood of prostate cancer, and those with suspicious family history are at high risk.
The NCCN recommends basing repeat testing intervals on PSA, DRE findings, and risk level, as follows:
-
PSA < 1 ng/mL, DRE normal (if done), in patients with average risk – 2-4 years
-
PSA 1-3 ng/mL, DRE normal (if done), in patients with average risk – 1-2 years
-
PSA ≤ 3 ng/mL, DRE normal (if done), in patients with high risk – 1-2 years
-
PSA < 4 ng/mL, DRE normal (if done), and no other indications for biopsy – 1-2 years
For patients with PSA levels above 3 ng/mL or very suspicious DRE results, the NCCN recommends repeat PSA, DRE, and workup for benign disease. Multiparametric MRI (mpMRI), if available, is strongly recommended, and measurement of biomarkers that improve the specificity of screening should be considered. [3] Similarly, for asymptomatic men with a PSA level of 3–10 ng/mL and a normal DRE, joint European guidelines strongly recommend prostate MRI to determine whether biopsy is indicated. [13]
American Urological Association (AUA) recommend against routine screening for the following groups [2] :
-
Any man with a life expectancy less than 10-15 years
-
Men under age 40 years
-
Men between ages 40 to 54 years at average risk
-
Men over age 70 years
For men 55 to 69 years of age, the AUA advises that the decision to undergo PSA screening involves weighing the benefits and risks. The guidelines strongly recommend the following [2] :
-
Shared decision-making for men age 55-69 years who are considering PSA screening, and proceeding based on patients’ values and preferences
-
A routine screening interval of 2 years or more in those men who have participated in shared decision-making and decided on screening.
In 2018, the US Preventive Services Task Force (USPSTF) revised its controversial 2012 recommendation against prostate cancer screening. Currently, the USPSTF advises that in men aged 55 to 69 years, the decision of whether or not to undergo screening should be individualized. This is a grade C recommendation, meaning that there is at least moderate certainty that the net benefit is small. For men aged 70 years and older, the USPSTF recommends against PSA-based screening for prostate cancer. [4]
The USPSTF concluded that currently available data are insufficient to support a separate, specific recommendation on PSA-based screening for prostate cancer in African-American men or in men with a family history of prostate cancer. While acknowledging the higher risk of prostate cancer in those groups, the USPSTF also notes the significantly higher risk of major infections after prostate biopsy in black men than white men, and the potential for harm in men with relatives whose prostate cancer was overdiagnosed. The USPSTF suggests that men with a positive family history who are most likely to benefit from screening are those with a first-degree relative who had advanced prostate cancer at diagnosis, who developed metastatic prostate cancer, or who died of prostate cancer. [4]
Current guidelines from the European Society for Medical Oncology (ESMO) recommend against population-based PSA screening for prostate cancer, on the grounds that it reduces prostate cancer mortality at the expense of overdiagnosis and overtreatment. The ESMO also recommends against testing for prostate cancer in asymptomatic men over the age of 70 years. [5]
Contrasting study data
Data from a Canadian study showed that from 1989-1996, the mortality rate was lower in a PSA-screened cohort than in a control group. Research from Tyrol, Austria, also indicated that screening can aid in reducing disease-specific mortality.
These beneficial effects are likely due to the fact that treatment, rather than observation, may enhance disease-specific survival. This was indicated in a Scandinavian study, which reported that radical prostatectomy was associated with significantly reduced disease-specific mortality, compared with watchful waiting. (No difference in overall survival was noted.) [14]
However, a US study, the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial, compared patients who received annual screening (the study offered PSA tests for 6 years and DREs for 4 years) with patients who did not undergo yearly testing and found no screening-related improvement in mortality. [15] Conversely, the European Randomized Study of Screening for Prostate Cancer (ERSPC) did show a decreased mortality in the trial's PSA-screened group; however, this multicenter study was flawed. [16]
Similar to the American study, a randomized trial comparing Swedish men allocated to screening every third year with those who received no screening showed no difference in prostate cancer–specific survival. [17] The issue remains unresolved.
US data have shown a decrease of 1% per year since 1990 in the prostate-cancer mortality rate, which coincides with the advent of PSA screening. Other theories have been proposed to account for the decrease; these include changing treatment practices and artifacts in mortality rates secondary to the changing incidence of prostate cancer.
Discontinuation of screening
In a 2010 study, Tang et al concluded that in the 75- to 80-year age group, discontinuation of PSA screening may be safe in African-American men with an initial PSA measurement of less than 6.0 ng/mL and in Caucasian men with an initial PSA measurement of less than 3.0 ng/mL. The investigators found that men in these groups are unlikely to develop high-risk prostate cancer or to die from prostate cancer. [18]
The NCCN advises that, although very few men over the age of 75 benefit from PSA testing, a clinically significant number may develop aggressive cancers that pose significant risk if they are not detected before they produce symptoms. For that reason, testing may be considered in select patients who are very healthy and have little or no comorbidity, but clinicians may consider raising the threshold for biopsy to a PSA level of > 4 ng/mL. [3]
As noted above, the USPSTF and ESMO recommend against PSA-based screening for prostate cancer for men aged 70 years and older. [5, 4]
Prostate Cancer Symptoms
Local signs and symptoms
In the pre-PSA era, patients with prostate cancer commonly presented with local symptoms. Urinary retention developed in 20-25% of these patients, back or leg pain developed in 20-40%, and hematuria developed in 10-15%. Currently, with PSA screening, 47% of cases are diagnosed in asymptomatic patients. In symptomatic patients, the most common complaints are urinary frequency (38%), decreased urine stream (23%), urinary urgency (10%), and hematuria (1.4%). However, none of these symptoms is unique to prostate cancer; each can arise from various other ailments.
Metastatic signs and symptoms
Metastatic symptoms include weight loss and loss of appetite; bone pain, with or without pathologic fracture (because prostate cancer, when metastatic, has a strong predilection for bone); and lower extremity pain and edema due to obstruction of venous and lymphatic tributaries by nodal metastasis. Uremic symptoms can occur from ureteral obstruction caused by local prostate growth or retroperitoneal adenopathy secondary to nodal metastasis.
Prostate-Specific Antigen Screening
Elevated PSA level
PSA is a single-chain glycoprotein that has chymotrypsinlike properties. The upper limit of normal for PSA is 4 ng/mL. Some advocate age-related cutoffs, such as 2.5 ng/mL for the fifth decade of life, 3.5 ng/mL for the sixth decade of life, and 4.5 ng/mL for the seventh decade of life. Others advocate race-specific reference ranges. Using data from screening studies, some have advocated upper limits of normal of 2.5 ng/mL instead of 4 ng/mL.
If the physician believes that an elevated PSA level may be due to infection, 4-6 weeks of antibiotics are provided, and then the PSA level is rechecked.
PSA velocity
PSA velocity is calculated using at least 3 PSA levels measured over a period of at least 18 months. A PSA velocity of 0.35 ng/mL/y when the PSA is ≤2.5 ng/mL, and of 0.75 ng/mL/y when the PSA is 4–10 ng/mL, have traditionally been used to prompt a prostate biopsy. However, evidence suggests in men younger than 50 years whose PSA is 4–10 ng/mL, a PSA velocity of 0.6 ng/mL/y may be a more appropriate threshold. PSA velocity is not useful in patients with PSA values above 10 ng/mL. [3]
Studies of PSA velocity have yielded varying results, and its value for screening remains controversial. For example, American Cancer Society guidelines do not recommend using the PSA velocity as part of screening for prostate cancer. [1]
Percentage of free PSA
The measurement of bound and free PSA can help to differentiate mildly elevated PSA levels caused by cancer from elevated levels resulting from benign prostatic hyperplasia. The lower the ratio of free-to-total PSA, the higher the likelihood of cancer. (Free PSA is reported as a percentage.) For example, among men with greater than 25% free PSA, only 8% are found to have cancer at prostate biopsy.
In contrast, more than half of men with less than 10% free PSA are found to have cancer at biopsy. While cutoffs may be used, the percentage of free PSA is usually employed as an additional factor in making an informed recommendation for or against biopsy. Generally, these percentages are useful in patients who have a PSA level in the range of 4-10 ng/mL.
This information is most useful in men with very large glands or in whom 1 biopsy result has already been negative. In healthy men with a PSA level of 4-10 ng/mL, many recommend biopsy without the additional free-PSA test or consider a trial of antibiotic therapy for 4-6 weeks before repeating the PSA test. (If antibiotic therapy quickly lowers the PSA level to within the reference range, the cause of the prior elevation is less likely to be prostate cancer, and the PSA test should be repeated within a few months.)
Biomarker measurement
In men with PSA levels > 3 ng/mL, several biomarker tests are available that can be used to further define the probability of clinically significant prostate cancer, and thus the need for biopsy. These include the Prostate Health Index (PHI), our kallikrein score test (4Kscore Test), SelectMDx, and ExoDx Prostate Test (EPI). [3]
Prostate Health Index
The PHI test is a diagnostic blood test that combines free and total PSA and the (-2) pro-PSA isoform (p2PSA). The PHI test is intended to reduce the number of unnecessary prostate biopsies in PSA-tested men. In prospective multicenter studies, the PHI test outperformed free and total PSA for detection of prostate cancer and improved prediction of clinically significant prostate cancer in men with a PSA of 2 or 4 ng/mL to 10 ng/mL. [19] The PHI test was approved by the US Food and Drug Administration (FDA) in 2012. [20]
Four kallikrein score test
The 4Kscore test measures free, intact, and total PSA and kallikrein-like peptidase 2. Like the PHI test, the 4Kscore test is intended to reduce the number of unnecessary prostate biopsies in PSA-tested men. It received FDA approval in 2021. [21] In a head-to-head comparison study, the PHI test and the 4Kscore test performed similarly. [5]
SelectMDx
SelectMDx testing uses measurement of mRNA expression levels of HOXC6 and DLX1 in urine after prostate massage, in combination with clinical risk factors, to predict presence or absence of high-grade prostate cancer. In a validation study, 35% of patients awaiting initial biopsy had a negative SelectMDx result, and in those patients, 95% of the biopsies showed no or low-grade prostate cancer. [22] Combining SelectMDx with multiparametric MRI can further improve predictive accuracy. [22] The FDA has determined that approval of SelectMDx was unnecessary.
ExoDx Prostate Test
The EPI uses the expression levels from three genes (PCA3, ERG, and SPDEF) in urine to calculate a risk score for high-grade prostate cancer. The urine sample for the test can be collected without prior digital rectal exam or prostate massage. The EPI risk score is independent of clinical variables. A score below the validated cut-point of 15.6 has a 91% negative predictive value for high-grade prostate cancer. [23] The ExoDx test was granted FDA Breakthrough Designation in 2019.
Digital Rectal Examination
DREs are examiner dependent, and serial examinations are best. Various factors are considered when a DRE is performed. A nodule is important, but findings such as asymmetry, difference in texture, and bogginess are important clues to the patient's condition and should be considered in conjunction with the PSA level. Change in texture over time can offer important clues about the need for intervention.
Pay careful attention to the prostate’s consistency, along with the seminal vesicles and adjacent organs. Such observation can be help to detect the disease’s spread to other structures, the results of which can be as follows:
-
Overdistention of the bladder due to outlet obstruction
-
Lower extremity lymphedema
-
Supraclavicular adenopathy
-
Lower extremity deep venous thrombosis
-
Cancer cachexia
-
Neurologic findings secondary to cord compression - Other subtle neurologic findings, such as paresthesias or wasting, are uncommon
Cysts and stones cannot be accurately differentiated from cancer based on DRE findings alone; therefore, maintain a high index of suspicion if the DRE results are abnormal.
If cancer is detected, the DRE findings form the basis of clinical staging of the primary tumor using the TNM staging system.
In most patients who are diagnosed with prostate cancer, however, the DRE results are normal and the PSA readings are abnormal.
Biopsy Studies
Physical examination findings alone cannot reliably differentiate a cyst or calculus from cancer foci. Therefore, a biopsy is warranted in these circumstances, to aid in the diagnosis and to determine the Gleason score.
Before the biopsy, antibiotics are administered and an enema is often provided, with a short course of antibiotics administered after the biopsy as well. Coagulation tests are not routinely performed, but patients are instructed to stop aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) 10 days prior to the biopsy. Many, but not all, physicians use lidocaine prior to the biopsy.
Transrectal ultrasound (TRUS)-guided prostate biopsy has been the standard approach. TRUS is used to examine the prostate for hypoechoic areas, which are commonly associated with cancers (see the image below). However, TRUS-guided biopsy fails to detect approximately 20% of significant prostate cancer cases, and may over-detect clinically insignificant prostate cancer.
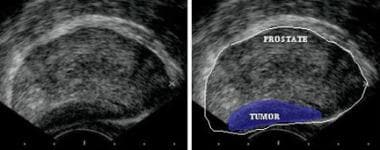 Transrectal sonogram of the prostate showing a hypoechoic lesion in the peripheral zone of the gland that is suggestive of cancer.
Transrectal sonogram of the prostate showing a hypoechoic lesion in the peripheral zone of the gland that is suggestive of cancer.
The over-detection of clinically insignificant or low-risk cancer of the prostate by systemic or standard 12-core TRUS biopsy technique spurred the development of a more targeted approach to obtaining prostate biopsy. MRI-TRUS fusion biopsy uses software that superimposes images obtained from MRI onto real-time ultrasound for a targeted biopsy of the prostate. This approach has shown potential in improving detection of clinically significant prostate cancer when compared with systemic prostate biopsy.
In a phase III trial that included 105 patients, MRI-TRUS fusion–guided biopsy detected prostate cancer that was missed by standard 12-core biopsy in 14.3% of cases, of which 86.7% were clinically significant, and upgraded 23.5% of cancers deemed clinically insignificant on 12-core biopsy to clinically significant prostate cancer. [37]
A prospective study in 1003 patients demonstrated the superior accuracy of MRI-TRUS fusion targeted biopsy compared with standard systemic biopsy for detection of high-risk prostate disease (Gleason score ≥4+3). [38] Targeted biopsy diagnosed 30% more high-risk cancers than did standard biopsy (173 vs 122 cases, P < 0.001) and 17% fewer low-risk cancers (213 vs 258 cases, P < 0.001) (28). When standard and targeted biopsy were combined, an additional 103 cases were diagnosed, mostly of low-risk disease. [38]
In a retrospective review by Sankineni et al of 33 patients with sub-capsular lesions evaluated by standard 12-core TRUS-guided biopsy and MRI-TRUS fusion–guided biopsy, 24 patients were found to have cancerous sub-capsular lesions, which are commonly aggressive tumors. [39] Although 19 of the 24 cases were confirmed by fusion-targeted biopsy and standard TRUS-guided biopsy; however, five lesions were identified only by fusion-targeted biopsy. [39]
A systematic review and meta-analysis concluded that the use of MRI-TRUS fusion–guided targeted biopsy increases the detection of clinically significant, higher-risk prostate cancer while lowering the detection of lower-risk disease. [24]
One disadvantage of MRI-TRUS fusion-guided biopsy is the cost of software. [40] In a retrospective study, Alberts et al used the Rotterdam Prostate Cancer Risk Calculator (RPCRC) to evaluate its potential in avoiding unnecessary MRI imaging. [41] In 122 patients who underwent multiparametric MRI (mpMRI) with subsequent MRI-TRUS fusion-guided biopsy after initially having negative TRUS, RPCRC could have avoided 62 (51%) mpMRI’s after a negative TRUS-guided random biopsy performed because of PSA level and/or digital rectal examination findings. [41]
With the growing acceptance of active surveillance protocols for men with localized disease, more patients are undergoing active surveillance for management of their prostate cancer. MRI-TRUS fusion-guided biopsy has the potential to add diagnostic value in identifying candidates for active surveillance.
Hu et al used targeted biopsy to determine whether Epstein criteria (Gleason score 6 or less, 2 or fewer cores positive, and 50% or less of any core) were sufficient for identifying candidates for active surveillance.
[42]
Targeted biopsy with mpMRI-TRUS fusion was performed in 113 patients undergoing active surveillance.
[42]
The likelihood of reclassification in lesions with grades 4 or 5 on mpMRI based on Standards of Reporting for MRI targeted biopsy studies (START) was 45% and 100%, respectively.
[42]
These rates of reclassification show the potential utility of targeted fusion biopsy for identifying candidates for active surveillance protocols.
The number of biopsy specimens that should be obtained is debated. Sextant- versus 12- versus 18-core biopsy protocols are published in the literature. The 12- or 18-core protocols yield more specimens from the lateral regions and usually sample the transition zone. Several studies have demonstrated an increase in the cancer detection rate, but others have not. The NCCN recommends extended-pattern biopsy with six sextant medial cores and six cores from the lateral peripheral zone, along with lesion-directed sampling of palpable nodules and sites corresponding to suspicious images. [3]
In men with a negative biopsy result, epigenetic profiling with the ConfirmMDx assay (MDxHealth, Irvine, CA) may help to distinguish patients who have a true negative biopsy from those at risk for occult cancer. ConfirmMDx is a commercially available assay that assesses methylation markers of prostate cancer (GSTP1, APC, and RASSF1) to distinguish histologically benign biopsy cores from patients diagnosed with no cancer, low-volume cancer (Gleason score 6), or higher-volume cancer (Gleason score 7). The assay has a negative predictive value of 90%, but a positive predictive value of only 28%. [25]
PCA3 is a prostate-specific, non-coding messenger RNA biomarker that is detectable in urine sediments obtained after three strokes of prostatic massage during DRE. A urine test for PCA3 (Progensa PCA3) is commercially available and is approved for use in men with negative biopsies to help determine whether repeat biopsy is needed. A negative PCA3 test result, considered together with clinical and other laboratory information, would argue against repeat biopsy. [19]
In patients with a persistently elevated PSA level in the face of negative biopsy results, the literature supports repeating the biopsy once or twice. Among cancer cases, 31% were detected on repeat biopsy and 39% were detected if the PSA value was greater than 20 ng/mL. If all of the biopsy results are negative, a repeat round of biopsies has been suggested when the PSA increases by 25% from the level at which the last biopsies were performed.
According to European guidelines, indications for repeat biopsy after a previously negative biopsy are as follows [19] :
-
Rising and/or persistently elevated PSA
-
Suspicious findings on DRE (5-30% cancer risk)
-
Atypical small acinar proliferation (ie, atypical glands suspicious for cancer; 40% risk
-
High-grade prostatic intraepithelial neoplasia (HGPIN) at ≥3 biopsy sites (~30% risk)
-
A few atypical glands immediately adjacent to HGPIN (~50% risk)
The guidelines recommend that repeat biopsies after negative biopsies be performed with MRI targeting.
Further workup depends on the clinical staging. A higher clinical stage of cancer determined by DRE findings, PSA level, and Gleason score (as determined by biopsy) correlates with an increased risk of extraprostatic spread, and these tests are considered key factors in determining the staging workup and predicting patient prognosis.
Bul et al studied the factors predicting reclassification from low-risk to higher-risk prostate cancer in men undergoing active surveillance and found a significant association between an increase in risk classification and the number of initial positive biopsy cores obtained. However, patient age, clinical stage, total number of biopsy cores, and PSA did not significantly influence the outcome. (Although a PSA doubling time of under 3y also had a significant link to reclassification to higher risk. [26] )
Histologic Findings
Gleason score
The most commonly used system for classifying the histologic characteristics of prostate cancer is the Gleason scoring system, which uses the glandular architecture within the tumor.
The predominant pattern and the second-most common pattern (seen in the image below) are each given a grade of between 1 and 5. The Gleason score is the sum of these 2 grades. Scoring based on the 2 most common patterns is an attempt to factor in the considerable heterogeneity within cases of prostate cancer. In addition, this scoring method was found to be superior for predicting disease outcomes compared with using the individual grades alone.
 Histologic scoring system (the Gleason scoring system) showing the 2 most common patterns seen on biopsy specimens in prostate cancer.
Histologic scoring system (the Gleason scoring system) showing the 2 most common patterns seen on biopsy specimens in prostate cancer.
Grades are based on the extent to which the epithelium assumes a normal glandular structure. A grade of 1 indicates a near-normal pattern, and grade 5 indicates the absence of any glandular pattern (less malignant to more malignant). This scheme of grading histologic features greatly depends on the skill and experience of the pathologist and is subject to some degree of individual variation.
Gleason scores range as follows:
-
Score of 2-4 - Considered low grade or well differentiated
-
Score of 5-7 - Considered moderate grade or moderately differentiated
-
Score of 8-10 - Considered high grade or poorly differentiated
Although the change in glandular architecture represented by the Gleason score is currently the most widely used and correlative histologic parameter, it is not the only histologic change that can be observed in prostate cancers. Indeed, notable changes in cell and nuclear morphology, neuroendocrine differentiation, and vascularity can be observed and may have great prognostic significance.
Grade groups
The grade grouping system was introduced in 2013, and has been adopted by the NCCN. Like the Gleason score, the Grade Group is derived from needle-core biopsies in patients with suspected prostate cancer or analysis of a radical-prostatectomy specimen. However, in contrast with the three risk tiers defined by the Gleason score, the Grade Group distinguishes five risk groups based on the core with the worst grade, as follows:
-
Grade Group 1 - Gleason 3+3
-
Grade Group 2 - Gleason 3+4
-
Grade Group 3 - Gleason 4+3
-
Grade Group 4 – Gleason 8
-
Grade Group 5 - GS 9-10
In a study of 8052 patients, grade grouping at biopsy and radical prostatectomy demonstrated better discrimination of recurrence-free survival between individual risk groups than Gleason score risk groups, with Grade Groups 2, 3, 4, and 5 each incrementally associated with increased risk. [27]
Perineural invasion
Perineural invasion is an indicator of invasiveness and is considered in terms of which side should possibly undergo a nerve-sparing procedure, as well as whether a patient might benefit more from high- or low-risk brachytherapy.
Prostatic intraepithelial neoplasia
Prostatic intraepithelial neoplasia (PIN) represents the putative precancerous end of the morphologic continuum of cellular proliferations within prostatic ducts, ductules, and acini.
Two grades of PIN are identified. Low-grade PIN is mild dysplasia. High-grade PIN encompasses moderate and severe dysplasia. High-grade PIN is considered by most to be a precursor of invasive carcinoma. Men with high-grade PIN alone can be started on finasteride and monitored closely.
The continuum that culminates in high-grade PIN and early invasive cancer is characterized by basal cell layer or basement membrane disruption, progressive loss of secretory differentiation markers, increasing nuclear and nucleolar abnormalities, increasing proliferative potential, and increasing variation in deoxyribonucleic acid (DNA) content (aneuploidy).
Clinical studies suggest that PIN predates a carcinoma by 10 or more years. [28] The clinical importance of recognizing PIN is based on its strong association with carcinoma. Studies claim that men with high-grade PIN in a prostate biopsy specimen have a 35-50% chance of being diagnosed with prostate cancer after a subsequent biopsy. [29] Atypical small acinar proliferation (ASAP) has also been associated with higher cancer detection rates.
The identification of PIN in prostate biopsy specimens warrants further searching for concurrent invasive carcinoma. In most men, this means repeat biopsies if the PSA level changes significantly. The same may also be true for ASAP findings after biopsy.
Evaluation of findings
Men with PSA levels below 10 ng/mL and low- or moderate-grade histology (Gleason score < 7) with no findings or minimal findings on physical examination may proceed to surgery or brachytherapy without further studies.
CT Scanning, MRI, and Bone Scanning
Men with PSA levels above 10 ng/mL, high-grade histology (Gleason score of 7 or higher), or physical findings that suggest stage T3 disease should probably undergo a staging computed tomography (CT) scan and bone scan. CT scanning is the one modality with evidence-based guidelines. The CT scan can be used to evaluate extension into the bladder and lymph nodes to help stage the patient's cancer or to consider lymph node sampling prior to treatment.
According to the National Comprehensive Cancer Network (NCCN), technetium-99m-methyl diphosphonate (MDP) bone scan is indicated in the initial evaluation of patients at high risk for skeletal metastases, as indicated by any of the following [30] :
-
T1 disease, PSA ≥20
-
T2 disease, PSA ≥10
-
Gleason score ≥8
-
T3/T4 disease
-
Symptoms suggestive of osseous metastasis
The NCCN recommends pelvic CT or magnetic resonance imaging (MRI) in patients with any of the following:
-
T3 disease
-
T4 disease
-
T1-T2 disease and nomogram-indicated probability of lymph node involvement >10%
Conventional endorectal MRI is helpful for localizing cancer within the prostate and seminal vesicles and for local staging. Dynamic, contrast-enhanced MRI and MR spectroscopic imaging are complementary in local staging, but their use is currently limited to a research setting.
Diffusion-weighted MRI appears to improve detection of transition-zone prostate cancer. In a retrospective study of 156 prostate cancer patients before they underwent radical prostatectomy, the addition of diffusion-weighted endorectal magnetic resonance imaging (MRI) to T2-weighted imaging improved not only the detection of transition zone prostate cancer but also the evaluation of tumor aggressiveness. [31] At the (individual) patient and sextant (localization) levels, there was improvement in the areas under the receiver operating characteristic curves. There was also an inverse correlation between tumor apparent diffusion coefficients and tumor Gleason scores in the transition zone. [31]
Guidelines from the NCCN [30] and the European Association of Urology [19] note that evidence supports the use of multiparametric MRI (mpMRI)—that is, the combination of T2-weighted images with diffusion-weighted imaging, dynamic contrast enhanced imaging, or H1-spectroscopy—in prostate cancer staging. The advantages of mpMRI include the following [30] :
-
Detection of large and poorly differentiated tumors (ie, Gleason score ≥7)
-
T staging: Detection of extracapsular extension, with high negative predictive values in low-risk men
-
N staging: MpMRI is equivalent to CT scan
-
M staging: MpMRI outperforms bone scan and targeted x-rays for M staging, with 98-100% sensitivity and specificity
Although MRI is superior to bone scanning in evaluating bone metastasis, it is impractical for routine total-body surveys. Instead, it is used to determine the etiology of questionable lesions found on bone scans. Bone-scan examples are seen below.
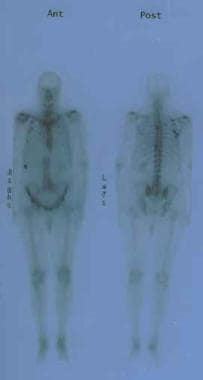 Anterior and posterior bone scans of a patient with prostate cancer, with metastasis to the 12th rib and thoracic spine represented by the increased uptake of isotope.
Anterior and posterior bone scans of a patient with prostate cancer, with metastasis to the 12th rib and thoracic spine represented by the increased uptake of isotope.
Neither CT scanning nor MRI can be used to determine if lymph nodes are reactive or contain malignant deposits, unless the nodes are significantly enlarged and a percutaneous biopsy can be performed.
Despite the wealth of literature regarding the lack of use that imaging studies have in men with low-risk disease, more than one third of patients with low-risk prostate cancer in a SEER (Surveillance, Epidemiology, and End Results program)–Medicare analysis underwent imaging studies. [32]
Positron Emission Tomography
American Urological Association/Society of Urologic Oncology (AUA/SUO) guidelines recommend positron emission tomography (PET) with prostate-specific membrane antigen (PSMA) as the preferred technique for assessing patients with PSA recurrence after failure of local therapy, as an alternative to conventional imaging, or in the setting of negative conventional imaging. [50] National Comprehensive Cancer Network (NCCN) guidelines recommend PET imaging for detection of bone metastatic disease when results of an initial bone scan are equivocal, or as an alternative to a bone scan. [30]
PSMA is a glycoprotein that is native to prostate epithelial cells and overexpressed 100–1,000-fold by prostate cancer cells. It is expressed principally on the cell surface and thus is readily accessible for binding of antibodies or low-molecular-weight ligands, which can be labeled with radionuclides such as gallium-68 or fluorine-18 to form a radiotracer detectable by PET. The ProstaScint scan used a murine monoclonal antibody radiolabeled with indium-111 for this purpose; however, use and acceptance of Prostascint was limited by concerns over its accuracy and image quality, and production of ProstaScint was discontinued in the United States in 2018. [51]
Flotufolastat F 18 (Posluma) is indicated for PET imaging of PSMA-positive lesions in men with prostate cancer with suspected metastasis who are candidates for initial definitive therapy, or those with suspected recurrence based on elevated PSA. Flotufolastat is an optimized PSMA-targeted molecule labeled with fluorine-18; it binds with PSMA on the surface of cells that express PSMA and is then internalized. Approval was based on the SPOTLIGHT and LIGHTHOUSE studies, in which flotufolastat F 18 detected recurrence and metastatic lesions in newly diagnosed men and those with undetectable metastasis at baseline with conventional imaging. [33, 34]
Fluciclovine F 18 (Axumin) is approved for PET imaging in men with suspected prostate cancer recurrence. It is an F 18–labeled synthetic amino acid taken up preferentially by prostate cancer cells. Approval was based on a comparative trial with 11C-choline, in which sensitivities for 11C-choline and fluciclovine F 18 were 32% vs 37%, specificities 40% vs 67%, accuracies 32% vs 38%, and positive predictive values (PPVs) 90% vs 97%. [35] In a second trial, the diagnostic performance of fluciclovine PET/CT in recurrent prostate cancer was superior to that of CT, and fluciclovine PET/CT provided better delineation of prostatic from extraprostatic recurrence. [36]
Staging of Prostate Cancer
The American Joint Committee on Cancer (AJCC) tumor/node/metastasis (TNM) classification and staging system for cancer are provided below. [43]
Primary tumor
Clinical tumor staging is as follows:
-
TX - Primary tumor cannot be assessed
-
T0 - No evidence of primary tumor
-
T1 - Clinically inapparent tumor not palpable
-
T1a - Tumor incidental histologic finding in 5% or less of tissue resected
-
T1b - Tumor incidental histologic finding in more than 5% of tissue resected
-
T1c - Tumor identified by needle biopsy (because of elevated PSA level); tumors found in 1 or both lobes by needle biopsy but not palpable
-
T2 - Tumor is palpable and confined within prostate
-
T2a - Tumor involves up to half of one lobe
-
T2b - Tumor involves more than half of one lobe but not both lobes
-
T2c - Tumor involves both lobes
-
T3 - Extraprostatic tumor that is not fixed or does not invade adjacent structures
-
T3a - Extracapsular extension (unilateral or bilateral)
-
T3b - Tumor invading seminal vesicle(s)
-
T4 - Tumor fixed or invading adjacent structures other than seminal vesicles (eg, bladder neck, external sphincter, rectum, levator muscles, pelvic wall)
Pathologic tumor staging is as follows (note that there is no pathologic T1 classification):
-
pT2 - Organ confined
-
pT3 - Extraprostatic extension
-
pT3a - Extraprostatic extension (unilateral or bilateral) or microscopic invasion of the bladder neck
-
pT3b - Seminal vesicle invasion
-
pT4 - Tumor is fixed or invades adjacent structures other than seminal vesicles (eg, external sphincter, rectum, bladder, levator muscles, pelvic wall)
Regional lymph nodes
Clinical lymph node staging is as follows:
-
NX - Regional lymph nodes not assessed
-
N0 - No regional lymph node metastasis
-
N1 - Metastasis in one or more regional lymph nodes
Pathologic lymph node staging is as follows:
-
pNX - Regional nodes not sampled
-
pN0 - No positive regional nodes
-
pN1 - Metastases in regional node(s)
Regional lymph nodes are assessed via surgical removal or through biopsy of the pelvic lymph nodes, including the obturator chain. The surgical boundaries include the bifurcation of the common iliac, the obturator nerve, and the node of Cloquet.
Distant metastasis
Distant metastasis staging is as follows:
-
M0 - No distant metastasis
-
M1 - Distant metastasis
-
M1a - Nonregional lymph node(s)
-
M1b - Bone(s)
-
M1c - Other site(s), with or without bone disease
Stage groupings
Staging of prostate cancer is based on the following five key pieces of information [6] :
-
The extent of the primary tumor (T category)
-
Whether the cancer has spread to nearby lymph nodes (N category)
-
The absence or presence of distant metastasis (M category)
-
The PSA level at the time of diagnosis
-
The Grade Group, based on prostate biopsy (or surgery); see Histologic Findings, above.
Table. Prognostic Groups for Prostate Cancer (Open Table in a new window)
Group |
Tumor |
Node |
M |
PSA (ng/mL) |
Grade Group |
Stage I |
cT1a-c |
N0 |
M0 |
< 10 |
1 |
cT2a |
N0 |
M0 |
< 10 |
1 |
|
pT2 |
N0 |
M0 |
< 10 |
1 |
|
Stage IIA |
cT1a-c |
N0 |
M0 |
10 to < 20 |
1 |
cT2a |
N0 |
M0 |
10 to < 20 |
1 |
|
pT2 |
N0 |
M0 |
10 to < 20 |
1 |
|
cT2c |
N0 |
M0 |
< 20 |
1 |
|
Stage IIB |
T1-2 |
N0 |
M0 |
< 20 |
2 |
Stage IIC |
T1-2 |
N0 |
M0 |
< 20 |
3 |
T1-2 |
N0 |
M0 |
< 20 |
4 |
|
Stage IIIA |
T1-2 |
N0 |
M0 |
≥ 20 |
1-4 |
Stage IIIB |
T3-4 |
N0 |
M0 |
Any |
1-4 |
Stage IIIC |
Any T |
N0 |
M0 |
Any |
5 |
Stage IVA |
Any T |
N1 |
M0 |
Any |
Any |
Stage IVB |
Any T |
Any N |
M1 |
Any |
Any |
Dess et al developed and validated a novel clinical prognostic stage group system for nonmetastatic prostate cancer that outperformed older systems. The new system classifies patients into nine staging groups, on the basis of scores derived from six variables: age, T category, N category, Gleason grade, pretreatment PSA level, and percentage of positive core biopsy results. [44]
Risk classification
Guidelines from the European Society for Medical Oncology (ESMO) recommend classifying localized prostate cancer as follows, in order to guide prognosis and therapy [5] :
-
Low risk: T1–T2a and Gleason score ≤6 and PSA ≤10
-
Intermediate risk: T2b and/or Gleason score 7 and/or PSA 10-20
-
High risk: ≥T2c or Gleason score 8-10 or PSA >20
The ESMO recommends that patients with intermediate- or high-risk disease have nodal staging using CT, MRI, choline positron emission tomography/CT (PET/CT), or pelvic nodal dissection. Patients with intermediate- or high-risk disease should be staged for metastases using technetium bone scan and thoracoabdominal CT scan, whole-body MRI, or choline PET/CT. [5]
Recent Advances: Molecular Markers
Currently, risk stratification for men who have recently been diagnosed with prostate cancer by biopsy is accomplished with the combination of PSA level, clinical stage, and Gleason score or Grade Group. The limitation of using these parameters for risk stratification is that collectively they do not address specific biologic features of prostate cancer—specifically, the aggressiveness of tumor cells. In addition, many studies have shown that localized prostate malignancy can vary in potential for progression in different patients, despite similar risk-stratifying characteristics.
This problem has sparked the advent of research and use of biological/genomic assays to help risk-stratify men diagnosed with localized prostate cancer. The theory behind utilizing genomic assays is to identify genes in biopsy specimens that potentiate cellular proliferation.
Cooperberg et al aimed to validate the application of the cell cycle progression (CCP) score in identifying men at risk for recurrent disease after radical prostatectomy. [45] The CCP score identifies genes that promote cellular proliferation. In this study, the CCP score was compared with the Cancer of the Prostate Risk Assessment post-Surgical (CAPRA-S score), which risk-stratifies recurrence after prostatectomy based on pre-procedural PSA, Gleason score, and clinical staging, and has been shown to have good accuracy. [45]
The CCP score predicted recurrence with a hazard ratio (HR) of 2.1 per unit increase in score. [45] In addition, the CCP score found an HR of 2.3 in some men with CAPRA-S scores of 0-2 (low risk of recurrence). Improved accuracy in predicting 10-year progression was noted when CCP score was combined with CAPRA-S score. [45]
In a similar study, Cuzick et al applied the CCP score to men with localized prostate cancer diagnosed by transurethral resection of the prostate (TURP). [46] The primary endpoint of the study was time to death. CCP score was found to be the most important variable and strongest prognostic factor for predicting time to death from prostate cancer. [46]
Klein et al assessed the use of Decipher, a 22-biomarker assay, on tissue retrieved from radical prostatectomy (RP) specimens from 1987 to 2008 for predicting the rate of recurrence. Within a cohort of 57 patients with preoperative diagnostic needle biopsy specimens, the primary objective was to validate biopsy-based Decipher for prediction of metastasis within 10 years of RP. [47] Biopsy-based Decipher was shown to be a significant predictor of recurrence within 10 years of RP, based on univariate and multivariate analysis, and was also a significant predictor of primary Gleason grade 4 or greater and rapid metastatic disease, two secondary endpoints of the study. [47]
In a review highlighting advantages and limitations of genomic testing, Falzarano et al note the vast variety of new testing available for aiding in diagnosis and risk stratification for prostate cancer. [48] In addition to the Prolaris/CCP score and Decipher, other genomic assays mentioned in the review include the following:
-
Confirm MDx
-
PCMT
-
Oncotype DX
-
Promark
Advantages of Confirm MDx and PCMT include a high negative predictive value (NPV), which reduces the need for repeat biopsies. [48] Limitations of Confirm MDx and PCMT are their inability to distinguish aggressive from indolent disease, which is a strength of the CCP score and Oncotype DX. [48] As described above, Decipher is unique in that it is a predictor of metastatic disease after RP. [48]
A systematic review by Olleik et al concluded that in men who have had a positive prostate biopsy, the use of active surveillance can be guided by ProMark, OncotypeDX, and Prolaris testing, and MRI. In patients who have undergone prostatectomy, the decision to add adjuvant therapy can be aided by use of NADiA ProsVue, Decipher, and Prolaris. To improve prediction of biopsy outcome and thus reduce the number of unnecessary biopsies, PHI, 4Kscore, and MRI can be used prior to initial and repeat biopsies, and ConfirmMDx and Progensa PCA3 can be used prior to repeat biopsies. [49]
Questions & Answers
Overview
Which men have the highest prevalence of prostate cancer?
Which conditions are included in the differential diagnoses of prostate cancer?
What is included in patient education about prostate cancer?
How prevalent is prostate cancer?
How does the approach to prostate cancer screening vary among guidelines?
What are the signs and symptoms of prostate cancer?
What are the signs and symptoms of metastatic prostate cancer?
What is the role of lab tests in the workup of prostate cancer?
What is the role of imaging studies in the workup of prostate cancer?
Which factors are used to state prostate cancer?
What is the anatomy of the male genitourinary tract relevant to prostate cancer?
What are the characteristics of prostate cancer tumors?
What are the components of prostate cancer screening?
When is prostate cancer screening indicated?
What are the ACS guidelines on prostate cancer screening?
What are the NCCN guidelines on prostate cancer screening?
What are the AUA guidelines on prostate cancer screening?
What are the USPSTF guidelines on prostate cancer screening?
What is the efficacy of prostate cancer screening?
When should prostate cancer screening be discontinued?
Which clinical history findings are characteristic of prostate cancer?
Which clinical history findings are characteristic of metastatic prostate cancer?
Which prostate-specific antigen (PSA) levels suggest prostate cancer?
Which prostate-specific antigen (PSA) velocity finding should prompt a prostate biopsy?
What is the role of free prostate-specific antigen (PSA) measurement in prostate screening?
What is the role of the Prostate Health Index (PHI) test in prostate cancer screening?
What is the role of a digital rectal exam (DRE) in prostate cancer screening?
What is the role of biopsy in the workup of prostate cancer?
When is repeat biopsy indicated in the diagnosis of prostate cancer?
What is prostatic intraepithelial neoplasia (PIN) in prostate cancer?
What is the Gleason score for prostate cancer?
What is the range of Gleason scores for prostate cancer?
What is grade grouping system for prostate cancer?
What is the role of perineural invasion in treatment selection for prostate cancer?
Which findings in the workup of prostate cancer prompt immediate surgery or brachytherapy?
What is the role of CT scans in the workup of prostate cancer?
What is the role of MDP bone scan in the workup of prostate cancer?
What are the NCCN guidelines for pelvic CT or MRI in the workup of prostate cancer?
What is the role of MRI in the workup of prostate cancer?
What are the limitations of imaging studies in the workup of prostate cancer?
What are the clinical tumor stages of prostate cancer?
What are the pathologic tumor stages of prostate cancer?
What are the clinical lymph node stages of prostate cancer?
What are the pathologic lymph node stages of prostate cancer?
What are the distant metastatic stages of prostate cancer?
How is prostate cancer staged?
What are the ESMO risk classifications of prostate cancer?
What are the limitations of prostate cancer risk stratification?
What is the role of biologic assays in prostate cancer risk stratification?
What is the role of genomic assays in prostate cancer diagnosis and screening?
What is the role of PET scanning in the workup of prostate cancer?
What is the role of ProstaScint scanning in the workup of prostate cancer?
What is the role of TRUS in the workup of prostate cancer?
What is the role of MRI-TRUS fusion biopsy in the workup of prostate cancer?
-
Estimated incidence of and mortality from prostate cancer. Courtesy of the American Cancer Society.
-
Relevant anatomy of the male pelvis and genitourinary tract.
-
Transrectal sonogram of the prostate showing a hypoechoic lesion in the peripheral zone of the gland that is suggestive of cancer.
-
Anterior and posterior bone scans of a patient with prostate cancer, with metastasis to the 12th rib and thoracic spine represented by the increased uptake of isotope.
-
Histologic scoring system (the Gleason scoring system) showing the 2 most common patterns seen on biopsy specimens in prostate cancer.
Tables
Group |
Tumor |
Node |
M |
PSA (ng/mL) |
Grade Group |
Stage I |
cT1a-c |
N0 |
M0 |
< 10 |
1 |
cT2a |
N0 |
M0 |
< 10 |
1 |
|
pT2 |
N0 |
M0 |
< 10 |
1 |
|
Stage IIA |
cT1a-c |
N0 |
M0 |
10 to < 20 |
1 |
cT2a |
N0 |
M0 |
10 to < 20 |
1 |
|
pT2 |
N0 |
M0 |
10 to < 20 |
1 |
|
cT2c |
N0 |
M0 |
< 20 |
1 |
|
Stage IIB |
T1-2 |
N0 |
M0 |
< 20 |
2 |
Stage IIC |
T1-2 |
N0 |
M0 |
< 20 |
3 |
T1-2 |
N0 |
M0 |
< 20 |
4 |
|
Stage IIIA |
T1-2 |
N0 |
M0 |
≥ 20 |
1-4 |
Stage IIIB |
T3-4 |
N0 |
M0 |
Any |
1-4 |
Stage IIIC |
Any T |
N0 |
M0 |
Any |
5 |
Stage IVA |
Any T |
N1 |
M0 |
Any |
Any |
Stage IVB |
Any T |
Any N |
M1 |
Any |
Any |

What would you like to print?
- Practice Essentials
- Overview
- Relevant Anatomy
- Characteristics of Prostate Cancer
- Screening Indications and Controversies
- Prostate Cancer Symptoms
- Prostate-Specific Antigen Screening
- Digital Rectal Examination
- Biopsy Studies
- Histologic Findings
- CT Scanning, MRI, and Bone Scanning
- Positron Emission Tomography
- Staging of Prostate Cancer
- Recent Advances: Molecular Markers
- Questions & Answers
- Show All
- Media Gallery
- Tables
- References




