Overview
Outcomes for burn patients have improved dramatically over the past 20 years, yet burns still cause substantial morbidity and mortality. [1, 2] Proper evaluation and management, coupled with appropriate early referral to a specialist, greatly help in minimizing suffering and optimizing results. [3, 4, 5]
Burn injury is a common cause of morbidity and mortality. [6] In the United States, approximately 1.25 million people with burns present to the emergency department each year. [7, 8] Among these, 63,000 have minor burn injuries that are treated primarily in the emergency department and an additional 6000 sustain major burn injuries that require hospital admission. [9, 10, 11] (See the image below.)
For excellent patient education resources, visit eMedicineHealth's First Aid and Injuries Center. Also, see eMedicineHealth's patient education article Thermal (Heat or Fire) Burns. [12]
 Initial evaluation and management of the burn patient. Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and tendency to result in hypertrophic scar formation vary enormously.
Initial evaluation and management of the burn patient. Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and tendency to result in hypertrophic scar formation vary enormously.
Initial Evaluation and Resuscitation
Before management of the burn wound can begin, the patient should be properly and completely evaluated. [4, 13, 5, 14, 15] Often, this is a brief effort, particularly in patients with small, uncomplicated wounds. In those with larger burns, evaluation of the wound is often of secondary importance. [16] As described by the American College of Surgeons Committee on Trauma, evaluation of the burn patient is organized into a primary survey and secondary survey. [17]
Primary survey
Burn patients should be systematically evaluated using the methodology of the American College of Surgeons Advanced Trauma Life Support course. This evaluation is described by the primary survey, with its emphasis on support of the airway, gas exchange, and circulatory stability. [18] First evaluate the airway; this is an area of particular importance in burn patients. Early recognition of impending airway compromise, followed by prompt intubation, can be lifesaving. [18] Obtain appropriate vascular access and place monitoring devices, then complete a systematic trauma survey, including indicated radiographs and laboratory studies.
Secondary survey
Burn patients should then undergo a burn-specific secondary survey, which should include a determination of the mechanism of injury, an evaluation for the presence or absence of inhalation injury and carbon monoxide intoxication, an examination for corneal burns, the consideration of the possibility of abuse, and a detailed assessment of the burn wound. [19]
Of particular importance is eliciting a detailed history upon first evaluation and transmitting this information with the patient to the next level of care. Inhalation injury is diagnosed based on a history of a closed-space exposure and soot in the nares and mouth. [20] Carbon monoxide intoxication is probable in persons injured in structural fires, particularly if they are obtunded; carboxyhemoglobin levels can be misleading in those ventilated with oxygen. [21] Persons with facial burns should undergo a careful examination of the cornea prior to the development of lid swelling that can compromise examination. [19] After evaluation of the burn wound, begin fluid resuscitation and make decisions concerning outpatient or inpatient management or transfer to a burn center (see American Burn Association burn center transfer criteria in Evaluation of the Burn Wound). [5, 22, 23]
Burn physiology
Tissue burn involves direct coagulation and microvascular reactions in the surrounding dermis that may result in extension of the injury. Large injuries are associated with a systemic response caused by a loss of the skin barrier, the release of vasoactive mediators from the wound, and subsequent infection. This results clinically in interstitial edema in distant organs and soft tissues, with an initial decrease in cardiac output and the metabolic rate. [24]
After successful resuscitation, a hypermetabolic response occurs, with near doubling of cardiac output and resting energy expenditure. Accelerated gluconeogenesis, insulin resistance, and increased protein catabolism accompany this response. Modification of this physiology through the administration of beta-adrenergic blockade, beta-adrenergic supplementation, nonsteroidal anti-inflammatory agents, recombinant growth hormone, androgenic steroids, and insulinlike growth factor 1 have been proposed to modify this physiology. Currently, data do not support the routine use of these therapies.
Fluid resuscitation
Burn patients demonstrate a graded capillary leak, which increases with injury size, delay in initiation of resuscitation, and the presence of inhalation injury for the first 18-24 hours after injury. Because the changes are different in every patient, fluid resuscitation can only be loosely guided by formulas. [25] The inherent inaccuracy of formulas requires continuous reevaluation and adjustment of infusions based on resuscitation targets. [26]
Most formulas recommend that all crystalloid be isotonic during the first 24 hours, generally Ringer lactate solution. Hypertonic saline has been recommended for resuscitation, but this practice has largely been abandoned because it is technically challenging and is not associated with improved clinical outcomes. In smaller children, whose gluconeogenetic capacity is immature, hypoglycemia is a threat and Ringer lactate solution with 5% dextrose should be added at a maintenance rate.
The modified Brooke or Parkland formulas are reasonable consensus formulas and are used to help determine the initial volume of infusion. Half of the total calculated 24-hour volume is administered in the first 8 hours post injury. Should the resuscitation be delayed, this volume is administered so that infusion is completed by the end of the eighth hour post injury. After 18-24 hours, capillary integrity generally returns and fluid administration should be decreased, following resuscitation endpoints. At this point, colloid administration is useful, generally 5% albumin in Ringer lactate solution. Increasingly, providers are replacing a portion of the calculated crystalloid with 5% albumin in patients with large deep burns. [27]
As a general rule, burns over less than 15% of the body surface area are not associated with an extensive capillary leak, and children with burns of this size can be treated with fluid administered at 150% of a calculated maintenance rate and close observation of their hydration status. Those who are able and willing to take fluid by mouth may be given fluid by mouth, with additional fluid administered intravenously at a maintenance rate.
Pigmented urine is commonly seen in the setting of high-voltage or very deep thermal injury. [12] This pigment should be cleared promptly to avoid renal failure. This can usually be achieved through the administration of additional crystalloid. The administration of bicarbonate may facilitate clearance of myoglobin by preventing its entry into the tubular cells. In rare circumstances, loop diuretics or mannitol can be useful, but this obscures urine output as a valid indicator of circulating volume.
Electrolyte levels should be carefully monitored and corrected. Cerebral edema and seizures can occur with severe hyponatremia, and rapid correction of hyponatremia may result in central pontine demyelinating lesions. Serum sodium, potassium, ionized calcium, phosphorous, and magnesium levels should be monitored and kept within physiologic range. Ideally, begin enteral feedings during resuscitation, except in patients with massive injuries or those who are underresuscitated and less likely to tolerate tube feedings because of ileus secondary to splanchnic underperfusion.
Evaluation of the Burn Wound
After the patient has been fully evaluated and stable hemodynamics and gas exchange are ensured, evaluate the burn wound in detail. [28] Evaluate burn wounds initially for extent, depth, and circumferential components. Decisions regarding the type of monitoring, wound care, hospitalization, and transfer are made based on this information. [22, 23] The American Burn Association burn center transfer criteria are as follows: [22]
-
Second- or third-degree burns greater than 10% total body surface area (TBSA) in patients younger than 10 years or older than 50 years [29]
-
Second- or third-degree burns greater than 20% TBSA in persons of other age groups
-
Second- or third-degree burns that involve the face, hands, feet, genitalia, perineum, or major joints
-
Third-degree burns greater than 5% TBSA in persons of any age group
-
Electrical burns, including lightening injury
-
Inhalational injury [20]
-
Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
-
Any patients with burns or concomitant trauma (eg, fracture) in which the burn injury poses the greatest risk of morbidity or mortality: In such cases, if the trauma poses the greater immediate risk, the patient may be treated initially in a trauma center until stable before being transferred to a burn center. Physician judgment is necessary in such situations and should be in concert with the regional medical control plan and triage protocols. [22]
-
A lack of qualified personnel or equipment for the care of children (transfer to facility with these qualities) [32]
Extent of burn
An accurate estimate of burn size is important for treatment and transfer decisions. Burn size or extent can be estimated in a number of ways. Perhaps most accurate is the age-specific chart based on the Lund-Browder diagram that compensates for the changes in body proportions with growth (see the image below). A burn is drawn on a cartoon figure, and an associated age-specific table is used to calculate the body surface area involved.
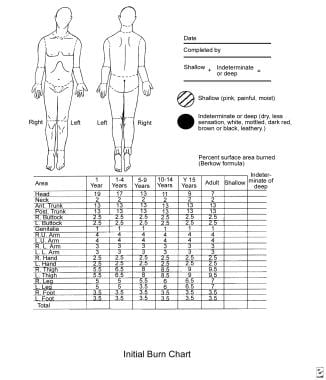 Initial evaluation and management of the burn patient. Burn size is best estimated using a chart that corrects for changes in body proportion with aging.
Initial evaluation and management of the burn patient. Burn size is best estimated using a chart that corrects for changes in body proportion with aging.
An alternative in adults is the "rule of nines." This is less accurate in children because their body proportions are different from those of adults. [35] For areas of irregular or nonconfluent burns, the palmar surface of the patient's hand can be used. [36] For a wide age range, the area of the palm without the fingers represents 0.5% of the body surface.
Burn depth
Burn depths are routinely underestimated during the initial examination. [37] Devitalized tissue may appear viable for some time after injury, and often, some degree of progressive microvascular thrombosis is observed on the wound periphery. Consequently, the wound appearance changes over the days following injury. Serial examination of burn wounds can be very useful.
Burn depth is classified as first, second, third, or fourth degree, as follows: [37]
-
First-degree burns are usually red, dry, and painful. Burns initially termed first-degree are often actually superficial second-degree burns, with sloughing occurring the next day.
-
Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and propensity to form hypertrophic scars (see the image below) vary enormously.
 Initial evaluation and management of the burn patient. Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and tendency to result in hypertrophic scar formation vary enormously.
Initial evaluation and management of the burn patient. Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and tendency to result in hypertrophic scar formation vary enormously.
-
Third-degree burns are generally leathery in consistency, dry, insensate, and waxy. These wounds will not heal, except by contraction and limited epithelial migration, with resulting hypertrophic and unstable cover. Burn blisters can overlie both second- and third-degree burns. The management of burn blisters remains controversial, yet intact blisters help greatly with pain control. Debride blisters if infection occurs. See the images below.
 Initial evaluation and management of the burn patient. Third-degree burns are usually leathery in consistency, dry, and insensate. These wounds do not heal.
Initial evaluation and management of the burn patient. Third-degree burns are usually leathery in consistency, dry, and insensate. These wounds do not heal.
 Initial evaluation and management of the burn patient. Management of burn blisters is controversial. Burn blisters occasionally obscure the presence of full-thickness wounds.
Initial evaluation and management of the burn patient. Management of burn blisters is controversial. Burn blisters occasionally obscure the presence of full-thickness wounds.
-
Fourth-degree burns involve underlying subcutaneous tissue, tendon, or bone. Usually, even an experienced examiner has difficulty accurately determining burn depth during early examination. As a general rule, burn depth is underestimated upon initial examination. [37]


Note circumferential, or near-circumferential, burn wounds because they may cause progressive extremity ischemia or interfere with ventilation as burn wound swelling increases. In such situations, timely escharotomy is essential. Perform extremity escharotomies as soon as peripheral perfusion is threatened. Do not wait until the extremity is overtly ischemic. Perform torso escharotomies as soon as ventilation appears compromised.
Burn Wound Infection
An ability to make the diagnosis of burn wound infection is important. A clinically focused set of burn wound infection definitions has recently been published and is summarized as follows:
-
Burn impetigo
Diagnostic points - Loss of epithelium from previously epithelialized surface; not related to local trauma
Treatment strategies - Regular cleaning of debris and exudate; topical antistaphylococcal antibiotics; grafting of chronically unstable areas of epithelium
-
Burn-related surgical wound infection
Diagnostic points - Infection in surgically created would that has not yet epithelialized; includes loss of any overlying graft or membrane
Treatment strategies - Regular cleaning of debris and exudate; systemic and topical antistaphylococcal antibiotics; grafting of chronically unstable areas of epithelium
-
Burn wound cellulitis
Diagnostic points - Infection occurs in uninjured skin surrounding a wound; signs of local infection progress beyond what is expected from burn-related inflammation
Treatment strategies - Systemic antibiotics directed against Streptococcus pyogenes; proper treatment of primary wound
-
Invasive burn wound infection
Diagnostic points - Infection occurs in unexcised burn and invades viable underlying tissue; diagnosis may be supported by results from histologic examination or quantitative culture
Treatment strategies - Systemic antibiotics directed against presumed pathogen; wound excision, with biologic closure when possible
Two of these, burn wound cellulitis and invasive burn wound infection, are seen with some regularity by clinicians outside a burn center environment.
Burn wound cellulitis (see the image below) usually manifests with progressive erythema, swelling, and pain in the uninjured skin around a wound. Usually, this is seen in the first few days after the burn occurred and is typically caused by S pyogenes. Infection can progress rapidly, but it is generally sensitive to penicillin. Excision of associated deep eschar can be essential to the successful treatment of cellulitis. Elevation to reduce edema is an important adjunct.
 Initial evaluation and management of the burn patient. Burn wound cellulitis manifests with increasing erythema, swelling, and pain in uninjured skin around the periphery of a wound.
Initial evaluation and management of the burn patient. Burn wound cellulitis manifests with increasing erythema, swelling, and pain in uninjured skin around the periphery of a wound.
Invasive burn wound infection (see the image below) is a rapid proliferation of bacteria in burn eschar that invades underlying viable tissues. A change in color, new drainage, and, occasionally, a foul or sickly sweet odor are clinical findings. Pseudomonal and other gram-negative species are common causes. This infection can be life-threatening and usually requires combined treatment with surgery and antibiotics.
 Initial evaluation and management of the burn patient. Invasive burn wound infection implies that bacteria or fungi are proliferating in eschar and invading underlying viable tissues. These wounds display a change in color, new drainage, and often a foul odor. These infections are life-threatening.
Initial evaluation and management of the burn patient. Invasive burn wound infection implies that bacteria or fungi are proliferating in eschar and invading underlying viable tissues. These wounds display a change in color, new drainage, and often a foul odor. These infections are life-threatening.
Fever and systemic toxicity commonly accompany both infections. Inspect burn wounds frequently to identify infection early. This is an important consideration in outpatient burn care. Someone must inspect the wounds managed in the outpatient environment to promptly detect infections. Errors in initial depth assessment are routine. Infections occur and must be treated in a timely manner. A wound monitoring plan is an essential part of burn care.
Burn Wound Management
Most burns are small; patients with small burns are appropriately treated in an outpatient setting if the burns do not involve critical areas such as the face, hands, genitals, or feet. [9, 11] The outpatient setting is the primary focus of this section. Outpatient burn management can be taxing and, when poorly performed, can cause unnecessary suffering and compromise long-term results. In some situations, the best plan is to coordinate outpatient management with the burn unit's team of doctors, nurses, and therapists because their expertise may facilitate attaining optimal outpatient results. However, most small burns can be properly managed by community-based providers with burn center consultation as needed. [11]
Selection for outpatient care
Several factors are relevant to the decision regarding the location of burn care. Airways must not be compromised. The wound must be small enough so that fluid resuscitation is unnecessary, which generally precludes outpatient care for burns over 10-15% of TBSA. The patient must be able to ingest adequate fluid orally. Typically, serious burns to the face, ears, hands, genitals, or feet should initially be managed in an inpatient setting.
The patient and family must be able to support an outpatient care plan. An adult caregiver should be available who can be with a child treated in an outpatient setting. A family member or visiting nurse must be available who can perform the necessary wound cleansing, inspection, and dressing applications because most patients cannot do this themselves. The family must have adequate transportation to return for clinic visits and unexpected emergency visits. If abuse is suspected, outpatient management is contraindicated. Finally, if the initial examination findings indicate that surgery is needed for a full-thickness wound area, the patient should be promptly admitted for surgery. [38] Despite all of these qualifications, most patients with smaller burns can be successfully treated in an outpatient setting.
Outpatient wound care strategies
Components of outpatient burn care include the following: [11]
-
Patient and family education
-
Wound cleansing
-
Choice of topical or membrane dressing [39]
-
Pain control
-
Early return instructions
-
Follow-up clinic visits
-
Long-term follow-up care
Wound cleansing and dressing techniques must be taught to the person who changes the dressings. Ideally, document this instruction.
The choice of the many medications or membranes to place on burn wounds remains unclear, but certain basic principles apply to all situations. Gently clean the wound of debris and exudate on a regular basis. This usually requires daily removal of accumulated exudate and topical medications. Small superficial burns managed in this setting present a low risk of infection, thus, a clean rather than sterile technique is reasonable. Patients may clean the burn with lukewarm tap water and mild soap.
Soaking dressings in lukewarm tap water may decrease the pain associated with their removal. Gently cleanse the wound with a gauze or clean washcloth, inspect for signs of infection, pat dry with a clean towel, and re-dress the patient. To manage infections promptly, teaching the patient and family to return promptly if they notice erythema, swelling, increased tenderness, odor, or drainage is important. The frequency of wound cleansing and dressing change is debated, but most small burns are managed adequately with daily cleansing and dressing.
Wound dressing, whether one is using topical medication or a wound membrane, should provide 4 benefits, including (1) prevention of wound desiccation, (2) control of pain, (3) reduction of wound colonization and infection, and (4) prevention of added trauma to the wound. [40] Most topical dressings for outpatient use have a viscous carrier that prevents wound desiccation and a broader antibacterial spectrum that reduces wound colonization. The addition of a gauze wrap minimizes soiling of both clothing and unburned skin and protects the wound from the external environment. A large number of excellent agents are available.
Superficial facial burns are commonly treated with a clear, viscous antibacterial ointment. Wounds around the eyes can be treated with heavy topical ophthalmic antibiotic ointments. [19] Treat deep burns of the external ear with mafenide acetate because it penetrates the eschar and prevents purulent infection of the cartilage. Appropriate wound care strategies address these principles.
Pain control in the outpatient setting can be difficult, and if pain and anxiety cannot be adequately managed at home, then hospitalization is appropriate. For most patients, an oral narcotic medication administered 30-60 minutes prior to a planned dressing change provides adequate pain control. Because most dressings are occlusive, pain control between dressing changes tends to be managed adequately without narcotics in most patients. Elaborate specific conditions may mandate an early return to the hospital. Particularly important are (1) pain and anxiety associated with wound care to the degree that wound care is compromised, (2) signs of infection, or (3) a wound that appears deeper than appreciated during the initial examination. Review wound care instructions with caregivers.
Inpatient management
The management plan for patients with large burns that require inpatient care is usually determined by the physiology of the burn injury. Management strategies for these patients are beyond the scope of this article yet generally require a coordinated approach that involves a specialized team. Hospitalization is divided into 4 general phases, including (1) initial evaluation and resuscitation, (2) initial wound excision and biologic closure, (3) definitive wound closure, and (4) rehabilitation and reconstruction.
Excision and grafting
Early excision and closure of full-thickness wounds changes the natural history of burn injury, avoiding the otherwise common occurrence of wound sepsis. [41] Wound size is the most important factor in determining the need for early operation because this correlates with the physiologic threat represented by the injury. These operations can be bloody and physiologically stressful, but the blood and stress can be minimized with proper planning and execution.
A prediction regarding the probability a wound will require operative management is of enormous practical value. Examination by an experienced burn surgeon remains the most reliable method, despite the many devices developed to measure burn depth or burn blood flow. The changes in wound appearance over the first few days after injury make serial examinations particularly useful tools in surgical planning.
Patients with small burns rarely develop overwhelming wound sepsis, and burn care providers often have the luxury of time to allow the wound to fully evolve, allowing accurate operative planning. An initial nonoperative approach to such wounds helps minimize the need for operation. Patients with larger injuries generally do better if their wound is addressed during the first few days after the burn occurred. If wounds cover more than 40% TBSA, this may require staged procedures. If the wounds involve more than 50% of the body surface, achieving immediate autograft closure is often impossible. When autograft material is exhausted, temporary biologic closure is achieved with human allograft or other temporary wound closure material. Wounds are later resurfaced with autograft when donor sites have healed.
Most wounds can be managed with layered excisions that optimize appearance and function. Sheet grafts are used whenever reasonable. Blood loss associated with these operations has been estimated in the past at 3.5-5% of the blood volume for every 1% of the body surface excised. However, less blood loss can be achieved through the use of extremity tourniquets, dilute epinephrine injection, and a brisk operative pace. Intraoperative hypothermia should be anticipated and prevented though operating room heating.
Skin substitutes
Temporary skin substitutes provide protection from mechanical trauma, a vapor barrier, and a physical barrier to bacteria. [42] These membranes contribute to a moist wound environment with a low bacterial density that is consistent with optimal wound healing. Split thickness human allograft remains the optimal temporary skin cover.
A number of membranes have been developed to effect permanent wound coverage, including epidermal, dermal, and composite substitutes. A sheet of autologous epithelial cells can be grown from a full-thickness skin biopsy specimen. These can be useful in patients with massive injury, but they are very fragile, expensive, and provide unreliable definitive cover. Dermal analogs include Integra R (Integra Life Sciences, Plainsboro, NJ) and AlloDerm R (LifeCell Corporation, The Woodlands, Tex); both require an associated epithelial autograft. Integra R is a bilayer material with an inner layer of 2-mm thick collagen isolated from bovine tissue and chondroitin-6-sulfate and an outer layer of 0.009-in polysiloxane polymer with vapor transmission characteristics similar to skin. Allogenic dermis designed to be combined with a thin epithelial autograft, AlloDerm R is another promising dermal analog. Hopefully, an autologous composite skin substitute will ultimately be developed.
Medications and Membranes
The choice of medication or membrane for a wound is a never-ending source of discussion and argument. Fortunately, most medications and membranes perform well if physicians carefully monitor wounds, keep them clean, prevent desiccation, and properly manage secondary infection.
A wide range of topical medications is available, including simple petrolatum, various antibiotic-containing ointments and aqueous solutions, and debriding enzymes. Some of the available topical medications and their characteristics are described in the lists below. All of them can be effective when used properly by experienced providers in a program of burn care that includes wound evaluation, regular cleansing, and monitoring.
Medications
Medications include the following:
-
Silver sulfadiazine - Broad antibacterial spectrum; painless application [43]
-
Aqueous 0.5% silver nitrate - Broad-spectrum coverage, including fungi; leeches electrolytes
-
Mafenide acetate - Broad antibacterial spectrum; penetrates eschar best
-
Petrolatum - Bland and nontoxic
-
Various debriding enzymes - Useful in selected partial-thickness wounds
-
Various antibiotic ointments - Useful in many superficial partial-thickness wounds
Membranes
Membranes include the following:
-
Porcine xenograft - Adheres to wound coagulum and provides excellent pain control
-
Split-thickness allograft - Vascularizes and provides durable temporary closure of wounds
-
Various hydrocolloid dressings - Provide vapor and bacteria barrier while absorbing wound exudate
-
Various impregnated gauzes - Provide vapor and bacteria barrier while allowing drainage
-
Various semipermeable membranes - Provide vapor and bacteria barrier
Acticoat (Westhaim Biomedical, Saskatchewan, Canada) - Nonadherent wound dressing that delivers a low concentration of silver for antisepsis
Biobrane (Dow-Hickman, Sugarland, Tex) - Synthetic bilaminate that facilitates fibrovascular tissue growth into inner layer and provides temporary vapor and bacteria barrier
Transcyte (Smith and Nephew, Largo, Fla) - Synthetic bilaminate that facilitates fibrovascular tissue growth into inner layer populated with allogenic fibroblasts and overlying layer that provides temporary vapor and bacteria barrier
AlloDerm R - Consists of cell-free allogenic human dermis; requires an immediate thin overlying autograft
Integra R - Provides scaffold for neodermis; requires delayed thin autograft
Wound membranes are different from medications and dressings in that they provide transient physiologic wound closure. This implies a degree of protection from mechanical trauma, vapor transmission characteristics similar to skin, and a physical barrier to bacteria. These membranes facilitate a moist wound environment with low bacterial density. They are commonly placed on clean superficial wounds while awaiting epithelialization. These membranes are mostly occlusive; therefore, they must be used with caution if wounds are not clearly clean and superficial. If an occlusive membrane is placed over devitalized tissue, submembrane purulence can occur with subsequent local and systemic sepsis.
Special Situations
Inhalation injury
The diagnosis of inhalation injury is primarily clinical, based on a history of closed-space exposure, facial burns, singed nasal hairs, and carbonaceous debris in the mouth and pharynx or sputum. [20] Chest radiograph findings are routinely normal until complications (usually infection) develop. Bronchoscopy findings may include carbonaceous debris, ulceration, or erythema, but these changes are not always apparent.
The clinical consequences of inhalation injury include upper airway edema, bronchospasm, small airway occlusion, increased dead space and intrapulmonary shunting, decreased lung and chest wall compliance, and infection. Management is supportive only. [44]
Pneumonia or tracheobronchitis occurs in at least 30% of patients with inhalation injuries, due to the loss of the ciliary clearance mechanism, small airway occlusion, alveolar flooding, and endotracheal intubation. Vigorous pulmonary toilet, with toilet bronchoscopy in selected patients, is a very important component of therapy. The role of tracheostomy in the management of inhalation injury is controversial. It can be very useful if particularly prolonged intubation or difficult weaning is anticipated or if unusually thick secretions are unmanageable through an endotracheal tube. Tracheostomy in children is associated with a higher incidence of serious structural problems that require prolonged cannulation and reconstruction and, ideally, is avoided whenever possible. [45]
Electrical burns
Compartment syndrome, cardiac arrhythmia, or myoglobinuria is uncommon in patients exposed to less than 500 volts, although patients sustaining midrange injuries (200-1000 V) can have destructive local injuries. High-voltage injuries are commonly associated with loss of consciousness, falls, fractures, myoglobinuria, compartment syndrome, and arrhythmia, and these individuals should be treated as trauma patients.
Chemical burns
Treatment of chemical exposures should begin with immediate removal of clothing and chemicals. [30, 31] First responders need to protect themselves from injury. Copious irrigation with tap water should then be performed for at least 30 minutes. Alkaline substances, less soluble in water, often take longer to clear. Consultation with personnel at the poison control center should be considered when evaluating anyone with a chemical burn. Adequate ocular irrigation can be facilitated by topical ocular anesthetics. With larger injuries, fluid resuscitation may be required. Some agents are associated with irritating fumes, which can result in airway compromise.
Toxic epidermal necrolysis
Toxic epidermal necrolysis is a systemic process triggered by a medication or viral syndrome that results in a separation at the dermal-epidermal junction. Both a cutaneous wound and a visceral wound develop, with variable degrees of dermal, mucosal, and conjunctival involvement. Endotracheal intubation is often required for airway protection. Wound care should be directed to prevent desiccation and superinfection, and nutritional support is important.
Facial burns
Especially in adolescents and adults, the deep sweat and sebaceous glands of the central face make it likely that most second-degree burns will heal well with adequate topical wound care. Many reasonable management options are available, including topical silver sulfadiazine or bland antibiotic ointments. [43] Burns around the eyes can be dressed with topical ophthalmic antibiotic ointments. [19] If grafting is a possibility, reserve thick donor skin with optimal color match for facial resurfacing. [46] Often, the "blush" areas, such as the upper back and shoulders, make good facial donor sites.
The most important point of early management of deeply burned ears is prevention of auricular chondritis. This is a serious complication in which the cartilage becomes infected and quickly liquefies. Twice-daily cleansing and the application of topical mafenide acetate, which penetrates the eschar, can minimize the condition. Subsequent management of the ear is based on the depth of injury.
Deep corneal burns are obvious during the physical examination. [19] The cornea has a clouded appearance. More subtle injuries can be detected only with topical fluorescein application. After facial edema resolves, lid retraction may occur with variable degrees of exposure of the globe or ectropion. When this is relatively mild, no intervention is required beyond ocular lubricants. Should keratitis occur, early lid release is advised.
Hand burns
Hand burns assume a high priority from the onset of care. [47] During the first 24-48 hours, adequate blood flow must be ensured. Regularly monitor consistency, temperature, and the presence of pulsatile flow (detectable using Doppler studies of the digital pulp). If blood flow is questionable, perform escharotomy or fasciotomy.
Splint hands in a position of function, ie, the metatarsophalangeal joints at 70-90°, interphalangeal joints in extension, first web space open, and wrist at 20° of extension. Elevate the hands to minimize edema, and have the patient perform range-of-motion exercises with a therapist twice daily. Deep dermal and full-thickness burns should undergo early excision and sheet autograft closure. Perform hand therapy throughout the healing period, stopping only in the few days immediately after grafting. If this is not performed, suboptimal long-term function results (see the image below).
 Initial evaluation and management of the burn patient. If hand positioning and therapy are ignored while overlying burns heal, poor long-term function may result.
Initial evaluation and management of the burn patient. If hand positioning and therapy are ignored while overlying burns heal, poor long-term function may result.
Initial evaluation and management of the burn patient. If hand positioning and therapy are ignored while overlying burns heal, poor long-term function may result.
Initial evaluation and management of the burn patient. If hand positioning and therapy are ignored while overlying burns heal, poor long-term function may result.
Rehabilitation
The final phase of burn care is rehabilitation and reconstruction. As survival has improved, this field has evolved rapidly, becoming highly specialized. Therapy should begin in the critical care setting; priorities include ranging, splinting, and antideformity positioning. Ranging is ideally performed twice daily, with the therapist taking all joints through a passive of range of motion. These activities help prevent the occurrence of many common contractures. As the seriously burned patient begins to recover, priorities include continuing passive ranging, increasing active ranging and strengthening, minimizing edema, pursuing activities of daily living, and preparing for work or play and school. [48]
Important aspects of rehabilitation after discharge include ongoing and progressive ranging and strengthening, postoperative therapy after reconstructive operations, and scar management. The most difficult hypertrophic scarring is seen in deep dermal burns that heal spontaneously in less than 3 weeks. Therapies to minimize hypertrophic scarring are begun as soon as burns are well healed and include scar massage, compression garments, topical silicone, steroid injections, and management of pruritus.
If they participate in a coordinated multidisciplinary burn aftercare program, most patients have satisfying long-term outcomes. The Life Impact Burn Recovery Evaluation (LIBRE) study found that survivors who sustained burns as children had long-term social participation outcomes similar to those of survivors who were burned as adults. [49]
Guidelines
Management of severe acute-phase thermal burns
Guidelines released in 2020, from a panel of experts brought together by organizations that included the French Society of Anesthesia, Critical Care and Perioperative Medicine (SFAR), provided recommendations for the management of severe acute-phase thermal burns in adults and children. These included, but were not limited to, the following suggestions [50] :
-
In hemodynamic management, use balanced crystalloid solutions
-
In hemodynamic management, the formula used in estimating the initial crystalloid infusion rate should at least include the body weight and total burned body surface area (BSA)
-
Basing changes on clinical and hemodynamic parameters, adjust the infusion rate as soon as possible in fluid resuscitation for severe burns
-
Patients with severe burns in whom the total burned BSA is over 30% should receive human albumin after the first 6 hours of management
-
Do not routinely intubate patients with burns involving the face or neck
-
If burns involve the entire face, consider intubation if the patient also demonstrates at least one of the following features: 1) a deep, circular neck burn; 2) symptoms of airway obstruction (ie, change in voice, stridor, laryngeal dyspnea); 3) a total burned BSA of 40% or greater
-
Do not routinely administer hydroxocobalamin after smoke inhalation
-
Restrict hydroxocobalamin administration to adults suffering from smoke inhalation in whom there is a high suspicion of severe cyanide poisoning and to children with smoke inhalation and signs of moderate to severe cyanide poisoning
-
In the absence of shock, burn cooling should be performed in adults with a total burned BSA of less than 20% and in children with a total burned BSA of less than 10%
-
Routinely prescribe thromboprophylaxis for severe burn patients in the initial phase
Management of acute pain in the adult burn patient
Clinical practice guidelines on the management of acute pain in the adult burn patient were released in 2020 by the American Burn Association. [51]
Elements of the pain assessment are as follows:
-
Perform several times daily.
-
Follow a protocol to ensure consistency in language.
-
If able, use pain assessment tools: patient-reported scales, Burn Specific Pain Anxiety Scale (BSPAS), Critical Care Pain Observation Tool (CPOT).
For opioid pain medications, the choice should be based on physiology, pharmacology, and physician experience. It should be individualized to the patient, with frequent adjustments to account for individual patient responses, the narrow therapeutic effects, and adverse effects. Use as few opiate equivalents as necessary for successful pain control. They should be used together with nonopioid and nonpharmacological measures. Educate patients about opioids and other pain medications and their roles in recovery.
The roles of nonopioid pain medications are as follows:
-
Acetaminophen: Use on all burn patients; monitor maximum daily dose.
-
NSAIDs: Consider use, owing to safety profile and efficacy; factors to consider include patient clinical picture (comorbidities) and surgeon preference.
-
Neuropathic pain agents (eg, gabapentin, pregabalin): Consider as adjuncts to opioids in those with neuropathic pain or whose pain is refractory to standard therapy.
-
Ketamine: Consider use for procedural sedation or in low doses as an adjunct to opioids in those who in whom reduced opioid consumption would be beneficial, in particular postoperatively.
-
Dexmedetomidine and clonidine: Recommended as pain management adjuncts; particular scenarios include patient signs of withdrawal and/or prominent anxiety; dexmedetomidine is a first-line choice for intubated burn patients.
-
Intravenous lidocaine: Not recommended as a first-line agent; however, it can be considered as a second- or third-line adjuvant.
-
Cannabinoids: Not recommended, owing to lack of evidence along with potential legal and political obstacles.
The use of regional anesthesia for burn pain management can potentially achieve improved pain relief, improved patient satisfaction, and a reduction in opioid use, without serious risks or complications.
Nonpharmacologic pain control techniques should be offered to every patient. The modalities for which the strongest evidence exists are hypnosis, cognitive-behavioral therapy, and virtual reality.
Questions & Answers
Overview
What is the morbidity and mortality of burn injuries?
What is included in the initial evaluation of burn patients?
What is the primary survey during the initial evaluation of the burn patient?
What is the secondary survey during the initial evaluation and resuscitation of the burn patient?
What is the physiology of burn injuries?
What is the role of fluid resuscitation in the initial evaluation of the burn patient?
What are the American Burn Association burn center transfer criteria?
How is burn size estimated in the initial evaluation of the burn patient?
How are burn depths classified?
How is burn impetigo diagnosed and treated?
How are burn-related surgical wound infections diagnosed and treated?
How is burn wound cellulitis diagnosed and treated?
How are invasive burn wound infections diagnosed and treated?
What are the clinical manifestations of burns?
What are is included in outpatient treatment of burn injuries?
What is included in inpatient treatment of burn injuries?
What is the role of excision and grafting in the treatment of the burn patient?
What is the role of skin substitutes in the treatment of the burn patient?
What is the role of medications in the treatment of the burn patient?
Which medications are used in the treatment of the burn patient?
Which wound membranes are used in the treatment of the burn patient?
What is the role of wound membranes in the treatment of the burn patient?
What is the initial evaluation and treatment of hand burns?
What is the initial evaluation and treatment of inhalation burns?
What is the initial evaluation and treatment of electrical burns?
What is the initial evaluation and treatment of chemical burns?
What is the initial evaluation and treatment of toxic epidermal necrolysis in burn patients?
What is the initial evaluation and treatment of facial burns?
What is the role of rehabilitation in the treatment of the burn patient?
-
Initial evaluation and management of the burn patient. Burn size is best estimated using a chart that corrects for changes in body proportion with aging.
-
Initial evaluation and management of the burn patient. Second-degree burns are often red, wet, and very painful. Their depth, ability to heal, and tendency to result in hypertrophic scar formation vary enormously.
-
Initial evaluation and management of the burn patient. Third-degree burns are usually leathery in consistency, dry, and insensate. These wounds do not heal.
-
Initial evaluation and management of the burn patient. Management of burn blisters is controversial. Burn blisters occasionally obscure the presence of full-thickness wounds.
-
Initial evaluation and management of the burn patient. Burn wound cellulitis manifests with increasing erythema, swelling, and pain in uninjured skin around the periphery of a wound.
-
Initial evaluation and management of the burn patient. Invasive burn wound infection implies that bacteria or fungi are proliferating in eschar and invading underlying viable tissues. These wounds display a change in color, new drainage, and often a foul odor. These infections are life-threatening.
-
Initial evaluation and management of the burn patient. If hand positioning and therapy are ignored while overlying burns heal, poor long-term function may result.
-
Initial evaluation and management of the burn patient. Estimating the burn area in an adult patient.
-
Initial evaluation and management of the burn patient. Estimating the burn area in a child.
-
Initial evaluation and management of the burn patient. Escharotomy incisions.
-
Partial-thickness burn.
-
A 2-year-old child with a scald burn to the hand.
-
Proper functional positioning for splinting of serious hand burns is the metacarpophalangeal joints are at 70-90° of flexion, the interphalangeal joints are in extension, the wrist is at 20° of extension, and the first web space is open.








