Background
Ehrlichiosis is an infection of white blood cells that affects various mammals, including mice, cattle, dogs, deer, horses, sheep, goats, and humans. [1, 2]
 Female Lone Star tick, Amblyomma americanum, found in the southeastern and Midatlantic United States. It is a vector of several zoonotic diseases, including human monocytic ehrlichiosis and Rocky Mountain spotted fever. Courtesy of the CDC/Michael L. Levin, PhD.
Female Lone Star tick, Amblyomma americanum, found in the southeastern and Midatlantic United States. It is a vector of several zoonotic diseases, including human monocytic ehrlichiosis and Rocky Mountain spotted fever. Courtesy of the CDC/Michael L. Levin, PhD.
Ehrlichia/Anaplasma are tiny (0.2-2 µm) obligate, intracytoplasmic, gram-negative bacteria that resemble Rickettsia; divide by binary fission; and multiply within the cytoplasm of infected white blood cells. Clusters of Ehrlichia multiply in host monocyte vacuoles (phagosomes) to form large, mulberry-shaped aggregates called morulae.
Ehrlichia inclusion bodies, such as morulae, are visible in the cytoplasm of infected mononuclear phagocytic cells after 5-7 days. The type of ehrlichiosis that develops varies and depends on the infecting species and the type of leukocyte infected. Human granulocytic anaplasmosis (HGA), formerly known as human granulocytic ehrlichiosis (HGE), is caused by Anaplasma phagocytophilum, which infect granulocytes. In contrast, human monocytic ehrlichiosis (HME) is caused by Ehrlichia chaffeensis, which infects monocytes.
HGA and HME cause the same clinical manifestations. Therefore, the term ehrlichiosis is used for both types of infections. The total duration of illness for HME and HGA is unknown. No chronic cases have been reported at this time.
Table. Characteristics of HME Versus HGA (Open Table in a new window)
|
Human monocytic ehrlichiosis (HME) |
Human granulocytic anaplasmosis (HGA) |
Cell type Affected |
Monocytes |
Granulocytes |
Organism |
E chaffeensis |
A phagocytophilum |
Vector |
Amblyomma americanum (Lone Star tick) |
Ixodes scapularis (black-legged tick), Ixodes pacificus (Western black-legged tick) in California, Ixodes ricinus in Europe, and probably Ixodes persulcatus in parts of Asia |
Location |
Southeastern and south-central United States |
Wisconsin and Minnesota, less active in New York and Connecticut, also California |
Rash |
30% of adults, 60% of children |
Rare |
Prognosis |
~3% mortality |
< 1% mortality |
In 2008, the ehrlichiosis case definition was divided into four classifications:
- Ehrlichia chaffeensis infection
- Ehrlichia ewingii infection
- Anaplasma phagocytophilum infection
- Undetermined ehrlichiosis/anaplasmosis
In 2009, a new Ehrlichia species was identified in patients in the upper Midwest area.
-
This species was previously called “ E. muris-like agent” (EMLA), but is now referred to as E. muris eauclairensis. No death has been reported with infection caused by this species. [3]
Because the tick vector and geographic range for HGA is the same as that for Lyme disease, rarely the 2 may coexist in the same patient; doxycycline is effective therapy for both.
In October 2008, a report was made of an apparent nosocomial infection with A phagocytophilum that was transmitted from blood donated by an infected woman who had spent time in Minnesota just prior to donating.
The major antigenic determinants of Ehrlichia are surface membrane proteins. These antigenic proteins are complex and consist of thermolabile and thermostable components. In terms of kilodalton (kd) molecular weight, the key protein bands associated with HME are the 27-, 29-, and 44-kd bands. The major antigenic determinants associated with HGA include the 40-, 44-, and 65-kd bands.
In 1999, Buller et al reported 4 incidents of ehrlichiosis in Missouri due to Ehrlichia ewingii. [4] The associated disease may be clinically indistinguishable from infection caused by E chaffeensis or A phagocytophilum; however, laboratory testing can distinguish these incidents from HGA and HME.
Go to Tick Removal and Tick-Borne Diseases for complete information on these topics.
See 7 Bug Bites You Need to Know This Summer, a Critical Images slideshow, for helpful images and information on various bug bites.
Patient education
Educate patients in endemic ehrlichiosis areas to take proper precautions when traveling through wooded and/or tick-infested areas.
For patient education information, see Ticks.
Etiology
Ehrlichia and Anaplasma species, members of the family Rickettsiae, are gram-negative, obligate, intracellular coccobacilli that resemble Rickettsia species. All 3 are forms of Alphaproteobacteria.
Like Rickettsia, Ehrlichia organisms gain access to the blood via a bite from an infected tick. A americanum (Lone Star tick, seen in the image below) is the principle tick vector of E chaffeensis and is the primary vector of human monocytic ehrlichiosis (HME). A phagocytophilum may be transmitted from Ixodes persulcatus ticks and possibly Dermacentor variabilis (dog tick/wood tick).
Female Lone Star tick, Amblyomma americanum, found in the southeastern and Midatlantic United States. It is a vector of several zoonotic diseases, including human monocytic ehrlichiosis and Rocky Mountain spotted fever. Courtesy of the CDC/Michael L. Levin, PhD.
The primary target cell for HME is the macrophage, and the primary target for human granulocytic anaplasmosis (HGA) is the granulocyte. Intracellular infection is established within phagosomes, most often found in macrophages in the liver, spleen, lymph nodes, bone marrow, lung, kidney, and CNS.
HME and HGA are more severe in those with impaired splenic function.
Individuals considered to be at risk for ehrlichiosis include the following:
-
From a review of the national surveillance data, cases of ehrlichiosis are more frequently reported in men than in women.
-
People aged 60-69 years account for the highest number of cases.
People with compromised immune systems (eg, resulting from cancer treatments, advanced HIV infection, prior organ transplants, or some medications) might be at increased risk for severe disease. [5]
Epidemiology
Occurrence in the United States
The distribution of ehrlichiosis in the United States mirrors the tick distribution and appropriate mammalian vectors (eg, white-footed mouse, white-tailed deer). Ehrlichiosis occurs where mammalian hosts are in contact with the appropriate tick vector (ie, A americanum,D variabilis,Ixodes ticks).
 Map of the United States showing the distribution of the Lone Star Tick, which is the principle vector for ehrlichiosis.
Map of the United States showing the distribution of the Lone Star Tick, which is the principle vector for ehrlichiosis.
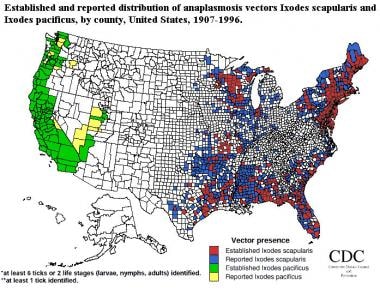 Established and reported distribution of anaplasmosis vectors Ixodes scapularis and Ixodes pacificus, by county, in the United States from 1907-1996. Courtesy of the Division of Vector-Borne Infectious Diseases at the Centers for Disease Control and Prevention.
Established and reported distribution of anaplasmosis vectors Ixodes scapularis and Ixodes pacificus, by county, in the United States from 1907-1996. Courtesy of the Division of Vector-Borne Infectious Diseases at the Centers for Disease Control and Prevention.
Most cases of ehrlichiosis in the United States occur in California and Texas and in the southeast and northeast regions of the country, with some cases occurring in the north-central states west of the Great Lakes.
In 2016, 4 states (Missouri, Arkansas, New York, Virginia) accounted for 50% of all reported cases of ehrlichiosis in the United States. [5]
Ehrlichiosis is a seasonal disease observed mainly from April to September. In 1999, ehrlichiosis became reportable to the US Centers for Disease Control and Prevention (CDC). In 2005, 786 cases of human granulocytic anaplasmosis (HGA) were reported. The 3 states that reported the most cases were New York (221 cases), Minnesota (186 cases), and Wisconsin (155 cases). [6, 7] In 2006, 646 cases of HGA were reported. The 3 states that reported the most cases were New York (235 cases), Minnesota (177 cases), and Wisconsin (49 cases). [8]
In the year 2000, only 200 cases of ehrlichiosis were reported, whereas more than 1,377 cases were reported in 2016. [5]
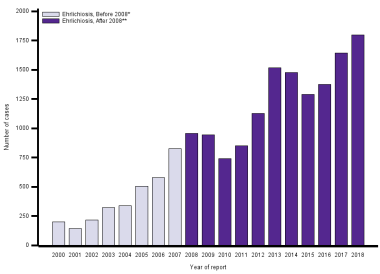 This graph shows the number of US ehrlichiosis cases caused by Ehrlichia chaffeensis and reported to the CDC from 2000 to 2018. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/).
This graph shows the number of US ehrlichiosis cases caused by Ehrlichia chaffeensis and reported to the CDC from 2000 to 2018. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/).
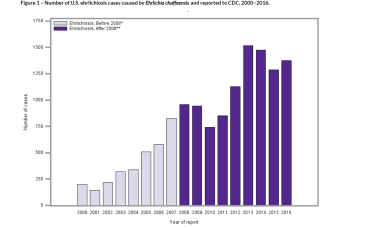 This graph displays the number of human cases of ehrlichiosis caused by Ehrlichia chaffeensis reported to the Centers for Disease Control and Prevention (CDC) annually from 2000 through 2016. *From 2000 to 2008, ehrlichiosis was included in the reporting category “human monocytic ehrlichiosis” in reports to the National Notifiable Diseases Surveillance System (NNDSS). **Since 2008, ehrlichiosis has been reported to the NNDSS under the categories “Ehrlichia chaffeensis infections,” “Ehrlichia ewingii infections,” and “Undetermined ehrlichiosis/anaplasmosis infections”, which include infections caused by Ehrlichia muris eauclairensis. Only E chaffeensis infections are shown above. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
This graph displays the number of human cases of ehrlichiosis caused by Ehrlichia chaffeensis reported to the Centers for Disease Control and Prevention (CDC) annually from 2000 through 2016. *From 2000 to 2008, ehrlichiosis was included in the reporting category “human monocytic ehrlichiosis” in reports to the National Notifiable Diseases Surveillance System (NNDSS). **Since 2008, ehrlichiosis has been reported to the NNDSS under the categories “Ehrlichia chaffeensis infections,” “Ehrlichia ewingii infections,” and “Undetermined ehrlichiosis/anaplasmosis infections”, which include infections caused by Ehrlichia muris eauclairensis. Only E chaffeensis infections are shown above. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
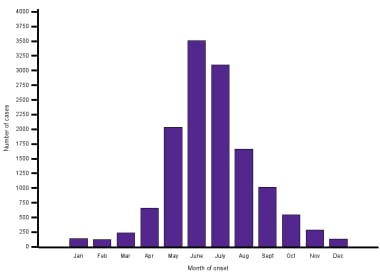 This graph shows the number of ehrlichiosis cases caused by Ehrlichia chaffeensis reported from 2000 through 2016 by month of onset to illustrate the seasonal trends. Cases are reported in each month of the year, although most are reported in June and July. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
This graph shows the number of ehrlichiosis cases caused by Ehrlichia chaffeensis reported from 2000 through 2016 by month of onset to illustrate the seasonal trends. Cases are reported in each month of the year, although most are reported in June and July. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
A 2011 study confirmed that B burgdorferi and A phagocytophilum share the same enzootic life cycle suggesting that it is important to monitor areas endemic for Lyme disease for HGA. In this study, La Crosse, WI is centrally located in a well-documented Lyme disease focus. HGA was identified by PCR in the blood of 53 patients with clinical findings consistent with HGA confirming that this region endemic for Lyme should now also be considered part of the upper Midwestern focus of endemicity for HGA. [9]
In 2005, 506 cases of human monocytic ehrlichiosis (HME) were reported. The 3 states that reported the most cases were New York (85 cases), Oklahoma (79 cases), and New Jersey (64 cases). In 2006, 578 cases of HME were reported. The 3 states that reported the most cases were New York (141 cases), Missouri (73 cases), and New Jersey (67 cases).
A 2011 report identified a new ehrlichia species in 4 patients in the Minnesota and Wisconsin areas. All patients had the traditional clinical syndrome and responded to treatment. On testing, 17 of 697 Ixodes scapularis ticks collected in Minnesota or Wisconsin were positive for the same ehrlichia species by polymerase chain-reaction testing and genetic analyses revealed that this new ehrlichia species was closely related to E muris. [10]
Notably, while cases and incidence rose, the case fatality rate (ie, the proportion of patients with ehrlichiosis who died as a result of infection) has declined since 2000, although the case fatality rate in recent publications is still roughly 1% of cases.
International occurrence
Ehrlichiosis occurs essentially worldwide, and the frequency parallels the distribution of the appropriate tick vectors for the transmission of Ehrlichia bacteria and the mammalian hosts. [11]
Ehrlichia sennetsu causes a mononucleosis-like illness in Japan and Malaysia.
Sex-related demographics
The rates of HME and HGA are higher in males than in females, most likely due to a higher rate of participation in high-risk outdoor activities among males.
In 2006, the CDC reported that of the 646 cases of HGA, 357 were males and 273 were females (16 cases did not specify sex). HME had a similar distribution, with 337 males and 234 females among the 578 cases in 2006 (7 cases did not specify sex).
The incidence rates per 100,000 for males were 0.26 for HGA and 0.24 for HME. For females, the rates were 0.19 for HGA and 0.16 for HME.
Age-related demographics
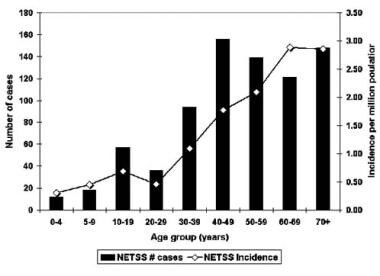
Ehrlichiosis is reported more frequently in adults than in children. The highest age range is between 40 and 64 years.
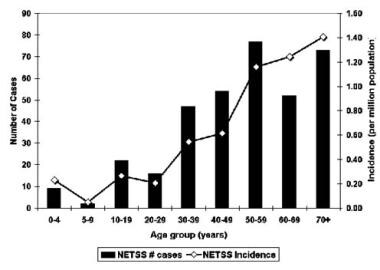
 Anaplasmosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
Anaplasmosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
 Ehrlichiosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
Ehrlichiosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
Prognosis
Ehrlichiosis carries an excellent prognosis in healthy hosts. A favorable outcome is associated with the early use of antibiotics. [12]
The mortality rate for human monocytic ehrlichiosis (HME) is reported to be 2-5%, while that for HGA is 7-10%.
Elderly patients (>60 y) are more likely than others to develop severe infections and account for most deaths due to ehrlichiosis. In addition, ehrlichiosis may be severe in immunocompromised hosts, manifesting as a Rocky Mountain spotted fever (RMSF)–like illness that may be fatal. The great majority of cases of ehrlichiosis are asymptomatic. Most cases present as mild-to-moderate acute febrile illnesses, but some cases are severe/life threatening.
HME has a reported hospitalization rate as high as 60%, while that for HGA is 28-54%.
-
Female Lone Star tick, Amblyomma americanum, found in the southeastern and Midatlantic United States. It is a vector of several zoonotic diseases, including human monocytic ehrlichiosis and Rocky Mountain spotted fever. Courtesy of the CDC/Michael L. Levin, PhD.
-
Map of the United States showing the distribution of the Lone Star Tick, which is the principle vector for ehrlichiosis.
-
Established and reported distribution of anaplasmosis vectors Ixodes scapularis and Ixodes pacificus, by county, in the United States from 1907-1996. Courtesy of the Division of Vector-Borne Infectious Diseases at the Centers for Disease Control and Prevention.
-
Anaplasmosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
-
Ehrlichiosis incidence by age. Courtesy of the Centers for Disease Control and Prevention.
-
This graph displays the number of human cases of ehrlichiosis caused by Ehrlichia chaffeensis reported to the Centers for Disease Control and Prevention (CDC) annually from 2000 through 2016. *From 2000 to 2008, ehrlichiosis was included in the reporting category “human monocytic ehrlichiosis” in reports to the National Notifiable Diseases Surveillance System (NNDSS). **Since 2008, ehrlichiosis has been reported to the NNDSS under the categories “Ehrlichia chaffeensis infections,” “Ehrlichia ewingii infections,” and “Undetermined ehrlichiosis/anaplasmosis infections”, which include infections caused by Ehrlichia muris eauclairensis. Only E chaffeensis infections are shown above. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
-
This graph shows the number of ehrlichiosis cases caused by Ehrlichia chaffeensis reported from 2000 through 2016 by month of onset to illustrate the seasonal trends. Cases are reported in each month of the year, although most are reported in June and July. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/index.html).
-
This graph shows the number of US ehrlichiosis cases caused by Ehrlichia chaffeensis and reported to the CDC from 2000 to 2018. Courtesy of the CDC (https://www.cdc.gov/ehrlichiosis/stats/).
Tables
|
Human monocytic ehrlichiosis (HME) |
Human granulocytic anaplasmosis (HGA) |
Cell type Affected |
Monocytes |
Granulocytes |
Organism |
E chaffeensis |
A phagocytophilum |
Vector |
Amblyomma americanum (Lone Star tick) |
Ixodes scapularis (black-legged tick), Ixodes pacificus (Western black-legged tick) in California, Ixodes ricinus in Europe, and probably Ixodes persulcatus in parts of Asia |
Location |
Southeastern and south-central United States |
Wisconsin and Minnesota, less active in New York and Connecticut, also California |
Rash |
30% of adults, 60% of children |
Rare |
Prognosis |
~3% mortality |
< 1% mortality |





