Introduction and History
This article reviews the clinical use of vacuum extractor (VE) delivery instruments in modern obstetric management. The limitations and risks of the VE are considered, as is the choice of delivery technique (VE vs forceps vs cesarean delivery) when labor ceases or other complications ensue.
Both forceps and the VE are in use as delivery instruments. In recent decades, the VE has progressively replaced forceps as the instrument of choice for many practitioners. [1, 2] In the United States, more than 80% of operative vaginal deliveries involve vacuum extraction. [3] Active controversy concerns if and when operative vaginal deliveries should be conducted and which instrument is the best to use in specific clinical settings.
VE has a long history. The initial applications of vacuum techniques in deliveries began in the 18th century. While VE became widely popular in Europe, the technique was little used in the United States until after the early 1980s, following the introduction of a series of new instruments, including disposable soft-cup extractors, new rigid cup designs, and handheld vacuum pumps.
Despite the current popularity of VE, forceps are the instrument of choice for many older clinicians. This is because of medical conservatism and original training, higher success rates, and a presumption of improved speed and control of the birth process. Nonetheless, VE has gained popularity as it is seemingly easy to use, requires less anesthesia/analgesia, has lower maternal morbidity, and is commonly believed to be safe. Large differences are observed in the popularity of instrumental delivery and of the specific type of instrument used in varying parts of the United States. This reflects the biases introduced by original training, the inherent conservatism of practitioners in embracing different techniques, and the absence of fixed guidelines for instrumentation. [4]
The retirement of classically trained obstetricians, the inability to conduct training operations (which is now partially offset by new training models), the medical-legal climate, and other changes in practice (including the high incidence of cesarean deliveries) result in an unclear future for all types of instrumental delivery, including VE. Finding clear answers to important management questions concerning instrumental delivery remains elusive. A great deal of traditional lore concerning delivery practices remains. Objective analysis of what constitutes best practice by the newer methods of evidence-based medicine is limited by continuous changes in practice, small patient numbers in many studies, changes in the official definition of procedures, and, especially for VE, the introduction of new instruments.
Despite these limitations, a need still remains for safe and effective operative vaginal delivery options. Further, good data suggest that this help can be safely and expeditiously provided by an instrumental delivery using either the forceps or a VE instrument. [5, 6, 7]
For related information, see Medscape's Pregnancy Resource Center.
Prerequisites for Vacuum Extraction
Both forceps and vacuum extraction have the same general indications. Operator experience and skill generally are the factors that influence which instrument is chosen.
Informed consent
Informed consent is required for any surgical procedure, including an instrumental delivery.
Consent for an instrumental delivery, especially in the face of urgency, has always been problematic and is often incomplete. [8] This has always been a curious feature of obstetric management, as the potential for maternal or fetal injury in VE or forceps operations is always present. Further, the medical and legal risks from an assisted delivery are substantially greater than those associated with many other surgical procedures.
Routinely discussing possible obstetric interventions with families at an earlier time during the pregnancy as part of routine prenatal care is important because of the controversy concerning bedside consents in acute situations. When antepartum discussions have occurred and the need for an instrumental delivery procedure occurs during labor, misunderstandings are reduced.
In general, consent for a surgical procedure requires the following:
-
An explanation of the need for the operation
-
A discussion of risks and benefits
-
A presentation of alternative modes of treatment
-
An opportunity to ask questions
An emergent or abbreviated bedside consent process still requires the following:
-
A (brief) description of the proposed operation to mother and family
-
Review of the indications for the proposed procedure
-
An indication of the limits of effort intended
Prepared physician
The clinician must have knowledge of the instrument chosen, VE indications, and well-practiced, appropriate technique. The decision to perform instrumentation should follow a logical progression involving an analysis of the course in labor, a pelvic examination with determination of fetal position and station, and a careful consideration of the fetal/pelvic relationship. In the uncommon situation that a true trial of instrumental delivery is contemplated, the obstetric team must understand the plan of management, the limits of intended effort, and the possibility of failure and the need for cesarean delivery.
Prepared patient
The initial requirement is always informed consent. Once consented, requirements include rupture of membranes, an engaged head, a fully dilated cervix and an empty bladder.
If the fetal position or the station of the presenting part is uncertain, a transperineal or transvaginal real time ultrasonographic examination is performed before attempting the operation. [9] Ultrasonography can also be used to judge the appropriateness of the vacuum cup application. [10, 11] These procedures are easily performed at the bedside. Position is readily identified by observing the fetal orbits and identifying characteristic intracranial anatomy (falx, posterior fossa, etc) and the location of the fetal spine.
Acceptable analgesia/anesthesia
Some outlet operative VE deliveries can be conducted without anesthesia or analgesia in multiparous patients. However, parturients do find operative vaginal procedures uncomfortable. Regional anesthesia may provide a more comfortable procedure.
Indications for Vacuum Extraction
General comments
The appropriate indications for operative delivery are those described by the American College of Obstetricians and Gynecologists (ACOG) in a practice bulletin. [7] Use of a vacuum is reasonable when an indication is present and can be readily and safely done; otherwise, cesarean delivery is the better option. The indications — as stated in the ACOG practice bulletin — for operative vaginal delivery are as follows:
-
Protracted second stage of labor
-
Suspicion of immediate or potential fetal compromise
-
Shortening the second stage for maternal benefit
It should be noted that these indications are relative; no absolute indications exist. Also, cesarean delivery is an option in the same clinical setting.
Prolonged second stage of labor
An extended second stage of labor is a relative, but not absolute, indication for an instrumental delivery. From a review of the available data, an appropriate conclusion is that the longer the second stage, the lower the probability of spontaneous vaginal delivery, and the higher the risk of instrumentation or cesarean delivery. [12, 13, 14, 15]
For nulliparous women, a protracted second stage can be defined as no progress (descent, rotation) after about four hours with epidural anesthesia and about three hours without epidural anesthesia. [12] For multiparous women, a protracted second stage can be defined as no progress (descent, rotation) after about two hours with epidural anesthesia and about one hour without epidural anesthesia.
Not surprisingly, obstetrical trauma such as postpartum hemorrhage, chorioamnionitis, and perineal injury become more likely as the second stage is extended. The situation for the neonate is less clear, but some increase in overall morbidity is probable. The data suggest that the magnitude of the maternal risk is greater than that for the infant, assuming proper maternal and fetal monitoring.
Continued poor progress in labor is not to be ignored. Failure to progress is the most common indication for intervention by a cesarean or an instrumental delivery.
For patients with slow progress approaching these limits, a normal fetal heart tracing, and no other indication for expediting delivery, evaluation of the risk of operative delivery versus expectant management should be undertaken. If fetal descent is progressing, or other favorable changes have occurred, expectant management, encouragement and oxytocin are employed. If the patient is unable to continue or is exhausted and judged to be a good candidate for operative delivery, then this is a reasonable option. Recent studies have challenged an arbitrary end point to the second stage of labor. The ability of electronic fetal heart monitoring to assist in assessing fetal status makes shortening the second stage at a set point unwarranted. [16]
Suspicion of immediate or potential fetal compromise
The suspicion of immediate or potential fetal compromise (eg, abruption, acutely nonreassuring electronic fetal monitoring tracing) is a classic indication for either an operative or a cesarean delivery.
When prompt delivery is necessary, the station and position of the fetal head, the fetopelvic relationship, operator skill, and a judgment of the severity of risk dictate the mode of delivery. In most cases, cord prolapse, abruptio placentae, or persistent bradycardia at a high station, even with full dilation with an engaged head are best managed by a cesarean delivery. Evaluation must be undertaken to assess if vaginal delivery can be safely and readily achieved before proceeding.
Maternal medical disorders
Certain maternal disorders preclude the ability of the mother to perform Valsalva safely. Typically, cardiac, cerebrovascular, or pulmonary disorders are included. There are other maternal disorders (neuromuscular, spinal cord injury, etc) that make pushing ineffective. An operative vaginal delivery can be undertaken when uterine contractions/labor leads to a descended fetus to a station where the practitioner feels operative vaginal delivery can safely and effectively be done.
Contraindications to Vacuum Extraction
Vacuum operations are contraindicated in certain settings. Neither the vacuum not the forceps should be applied where the fetal risk is either unknown or perceived to be high, or when the application proves difficult or the maternal pelvic anatomy is questionable. Questions of operator skill and experience in that specific clinical setting are also noted.
General contraindications include the following:
-
Operator inexperience
-
Inability to achieve a correct application (midline, over flexion point)
-
An inadequate trial of labor or lack of a standard indication
-
Uncertainty concerning fetal position or station not resolved by examination or real-time ultrasound study
-
Suspicion of fetopelvic disproportion (advanced cranial molding, bone overlap, caput)
-
An inappropriate fetal presentation (eg, breech, face, brow)
-
A known or suspected fetal bleeding diathesis or demineralizing bone disease
Relative contraindications are as follows:
-
Prior scalp sampling
-
Prior failed forceps
-
Gestational diabetes or pregestational diabetes
-
Known or suspected fetal macrosomia
The ACOG practice bulletin discourages the use of vacuum extraction prior to 34 weeks of gestation; however, it does not establish a safe lower limit for gestational age. [7]
Definitions
ACOG has established standard definitions for instrumental delivery operations. These include outlet, low, and midpelvic operations. While the guidelines were originally written for forceps procedures, the same descriptions are easily applied to vacuum extraction operations with minor modifications. [17, 7]
Outlet forceps/vacuum
-
The leading point of the fetal skull has reached the pelvic floor, and at or on the perineum, the scalp is visible at the introitus without separating the labia.
-
The sagittal suture is in anteroposterior diameter or a right or left occiput anterior or posterior position.
-
Rotation does not exceed 45 degrees.
Low forceps/vacuum
-
The leading point of the fetal skull is ≥2 cm beyond the ischial spines, but not on the pelvic floor (ie, station is at least +2/5 cm).
-
Low forceps have two subdivisions:
-Rotation ≤45 degrees
-Rotation >45 degrees
Midforceps/vacuum
-
The head is engaged (ie, at least 0 station), but the leading point of the skull is not ≥2 cm beyond the ischial spines (ie, station is 0/5 cm or +1/5 cm).
Design of the Vacuum Extractor
Vacuum extraction instruments
Vacuum extraction (VE) instruments are constructed of varying materials including polyethylene or silastic plastic and stainless steel. Several features are found in all designs. These include the following:
-
A mushroom-shaped vacuum cup of varying composition, diameter, and depth
-
A fixed internal vacuum grid or guard within the vacuum cup
-
A combined vacuum pump / handle or a vacuum port for a vacuum hose attachment
-
A handle for traction
Rigid-cup designs include the classic Malmström stainless steel vacuum cup and the various modifications of this instrument introduced since the 1960s. New rigid plastic cup extractors mimic the Malmström device. These were originally designed for use with deflexed or posterior positioned heads but now are becoming popular for all types of deliveries. [18] A recent trend in VE design is to incorporate the vacuum pump within the handle, avoiding the need for a separate vacuum tube and for the assistance of a birth attendant in producing vacuum.
The soft-cup extractors include numerous disposable polyethylene or combined polyethylene-silastic cup designs that differ in largely inconsequential and clinically unimportant ways.
Comparison of instruments
Soft or flexible vacuum cups have a higher incidence of failure than either rigid vacuum cups (plastic or metal) or forceps. [19] This is primarily due to their higher frequency of spontaneous detachment pop-offs. However, the application of soft vacuum cups also results in less fetal cosmetic injury (principally scalp injury) than rigid cups. This partially reflects the inability of soft cups to generate the same degree of scalp traction as is possible when rigid cups are applied.
Other design issues are important to cup choice. In some plastic extractor designs, the relatively rigid tube connecting the handle to the cup precludes accurate placement of the instrument when the fetal head is markedly deflexed or occiput posterior. This contributes to failure when such cranial malpositions are present. Higher success rates have recently been reported when rigid plastic cups similar to the original Malmström design are used for such deflexed and posterior presentations
Vacuum Extraction Technique
Appropriate technique is important when the vacuum extraction (VE) is used. [20, 21, 22, 23] The safety and success of vacuum-conducted extraction operations depend on the following:
-
The accuracy of the initial cup application (ie, cup center over flexion or pivot-point)
-
Case choice
-
The traction technique, including degree of effort (number of tractions), vector of traction, method of applied force
-
The fetal cranial position (including deflection) and fetal station at the time of application
-
The cup design
-
The fetopelvic relationship
If the prerequisites for VE operation are met, informed consent is obtained. Thereafter, the position, station, and attitude of the fetal head are verified by pelvic examination and an instrument is chosen. To correctly insert and position the cup, a specific protocol is followed. [20, 21]
Correct application
Once what is believed to be a proper cup application is established, sufficient vacuum (100-150 mm Hg) to fix the cup to the fetal head is applied. A check of the cup should then again be done to ensure no maternal tissue is present before higher pressure that is required for traction is employed.
The labia are separated and the cup is compressed to allow insertion into the vagina. In order to effectively assist a vaginal delivery, placement of the vacuum should be at the correct flexion point. This is done so that the flexion point is an imaginary spot over that midline of the sagittal suture, approximately 6 cm from the anterior fontanelle and 3 cm from the posterior fontanelle (see figure). The center of the cup is placed at the pivot point, making the edge of the cup ~3 cm from the anterior fontanelle and just at the edge of the posterior fontanelle.
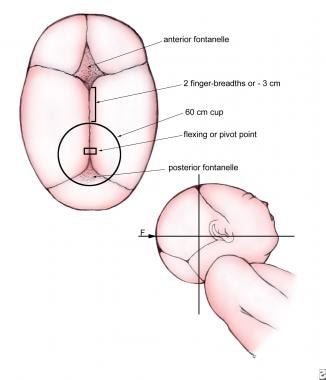
Access to the posterior fontanel is usually partially blocked once the extractor cup is correctly placed, rendering this familiar landmark unusable. The further the cup center is displaced from the cranial pivot or flexion point, the greater the failure rate. Traction with an oblique application results in progressive cranial deflexion or twisting (see the image below).

This actually increases the work of the extraction by presenting an ever larger cranial diameter to the birth canal. [21]
Traction
Once the surgeon has verified cup placement, full vacuum is applied (450-600 mm Hg) and traction follows, paralleling the uterine contractions. The direction of pull on the traction handle changes as the fetal head transverses the pelvic curve (see the images below).
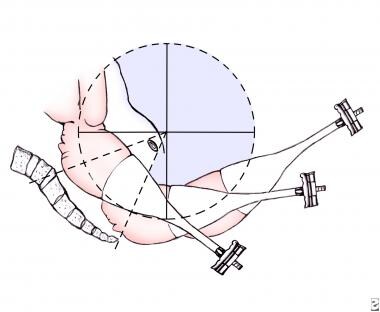
Traction efforts are timed to coincide with uterine contractions. Once the contraction begins, the vacuum pump is actuated until the appropriate degree of vacuum pressure is reached. Traction by the surgeon follows, with the force applied to the extractor handle gradually increased to the desired level, paralleling the rise in uterine force generated by the contraction.
As force is applied maternal expulsive efforts continue. As each contraction wanes, the tension on the extractor handle is relaxed. Attempting traction without the assistance of maternal bearing down efforts and/or a uterine contraction is less effective. These techniques simply predispose to failure and risk a fetal scalp injury from a pop-off.
In the relaxation phase between contractions, the vacuum can either be maintained or reduced to less than 200 mm Hg. Both techniques are acceptable. Continuous vacuum throughout the procedure and intermittent vacuum with the vacuum released between contractions, have been studied in a randomized trial. [24] No differences between groups are noted with regard to the speed of delivery, rates of instrument failure, or maternal or fetal outcomes. Thus, the use of either technique is at the discretion of the surgeon. The authors favor vacuum reduction.
A 2012 Cochrane review examined the safety and efficacy of rapid versus stepwise negative pressure application for vacuum extraction. The authors found that rapid negative pressure application reduces the duration of vacuum extraction without affecting maternal or neonatal outcomes. [25]
During traction, the surgeon should place the nondominant hand within the vagina, with the thumb on the extractor cup and one or more fingers on the fetal scalp. So positioned, the accoucheur follows the descent of the presenting part and can judge the appropriate and changing angle for traction while gauging the relative position of the cup edge to the scalp. This helps to detect cup separation. The vector of traction is in the curve of the pelvis. The initial angle for traction depends on the station but is usually downward, then progressively extending upward as the head emerges. Once the head has been extracted, the vacuum pressure is relieved, the cup removed and the usual techniques to complete the delivery are followed.
Jerking motions and oblique pulls are best avoided as they risk cup displacement. Any attempt at rotation of the device may lead to detachment or fetal scalp injury. Under traction, the fetal head usually rotates automatically as descent occurs.
An episiotomy is not recommended as a routine measure during a VE operation unless the soft tissue impedes the descent of the presenting part. Episiotomy has been shown to increase the incidence of third and fourth degree lacerations.
Ideally, descent of the presenting part should begin with the initial traction effort, assuming proper coordination with the maternal bearing down efforts and the uterine contractions. If the operator is uncertain that descent has occurred, a maximum of 2 additional tractions may be attempted. [26] The failure to clearly achieve fetal station after properly timed traction in the correct vector of force mandates prompt reassessment of the procedure both in terms of technique and desirability. Recurrent tensioning of the scalp without descent of the presenting part (negative traction) predisposes to cup pop-offs and is believed to increase the risk for scalp injury.
Limits to effort
The maximum duration of a vacuum extraction is unknown. A maximum of 2-3 pop offs, three sets of pulls and/or a total application time of 15-20 minutes have all been recommended, though some argue for lower time limits. [27]
When the number of pop-offs or the acceptable number of total tractions efforts are considered, the literature is inconsistent. In terms of traction number, studies performed with forceps and rigid-cup extractors have consistent findings. In approximately 85% of births, seemingly independent of whether the delivery is via forceps or the VE, the delivery occurs with 4 or fewer tractions. [28, 29, 30]
Although several studies have demonstrated a relationship between duration of cup application and development of cephalohematoma, the major morbidity of these lesions was largely cosmetic.
Table 1. Number of Tractions Required in Vacuum Extraction and Forceps Deliveries* (Open Table in a new window)
Number of Traction Efforts |
Successful Malmström Vacuum Extractor Deliveries (n=433) |
Successful Forceps Deliveries† (n=555) |
1-2 |
296 (68.4%) |
213 (38.4%) |
3-4 |
108 (24.9%) |
270 (48.6%) |
≥5 |
29 (6.7%) |
72 (12.9%) |
* Breech, cesarean delivery, and transverse lies, are excluded. [30] † Type unspecified |
||
The upper number of acceptable pop-offs is similarly not established. Clinical experience indicates that more than 2 pop-offs is sufficient, especially if progress has been minimal and the cup application and traction technique were proper. However, the correct number is not established.
Sequential instrument use
Recent studies by Gardella [31] and Towner [32] involving large numbers of cases report that sequential operations (vacuum extraction/forceps) are associated with an increased risk for fetal intracranial hemorrhage (ICH), exceeding the risk when either forceps or VE are used alone. Similar data concerning an enhanced risk from combined procedures comes from review of the 1998 Food and Drug Administration (FDA) advisory paper on VE, [33] as well as other sources. However, this has not been the finding in all series. [34] Additional discussion of intracranial injuries and instrumental delivery occurs in Choice of Instrument.
Injuries from multiple instrument use are most likely when a degree of unrecognized fetopelvic disproportion is present and, despite difficulty, the clinician cannot refrain from pursuing a vaginal operative delivery. When one type of instrument is applied and fails, no absolute prohibition exists to trying a different device. However, limiting effort and case choice are critical.
In some cases, changing the delivery instruments can constitute good management. These include those in which technical problems, such as a malfunctioning hand pump, a misapplied vacuum cup, or traction in the incorrect vector of force, are believed to be the cause of failure. The least desirable cases are those in which traction without progress or multiple pop-offs occur following a correct application of the vacuum extractor and appropriate traction.
For most obstetric surgeons, the failure of a properly applied delivery instrument should be followed by a prompt cesarean delivery.
Prophylactic antibiotics
Traditionally, antibiotics have not been administered for the sole indication of an instrumental delivery either with the VE or forceps. No compelling data suggest that prophylactic treatment is appropriate. [35] Antibiotics should be administered to women during labor/parturition following the usual obstetric indications and not specifically for an instrumental delivery.
Documentation
Vacuum extraction is potentially associated with delayed complications in neonates that might later be associated rightly or wrongly to the events of parturition. Especially in reference to all obstetric manipulations, full reporting in the medical record is prudent.
Preoperative note includes the following:
-
Intentions of the surgeon/limits of effort intended
-
Clinical setting
-
Discussion of consent process
-
Complemented by a detailed post procedure note
Surgical operation documentation is as follows:
-
Parallel the documentation practices for other surgical procedure; either dictate the procedure or use a computer template
-
For dictations, follow the institutional requirements for documentation (eg, preoperative/postoperative diagnoses, procedure, surgeons)
Contents of surgical note are as follows:
-
The indications for the operation/clinical setting that prompted intervention
-
Document that a consent process preceded the operation
-
Discuss maternal/fetal evaluations prior to the application of the instrument (eg, examination, Leopold, ultrasound)
-
Include standard prerequisites for vaginal delivery procedure present (eg, full dilation, engagement, bladder empty)
-
Record the station, position, and orientation of the fetal head
-
Report number of tractions and pop-offs (if any)
-
Total time of cup application
-
Report any complications (eg, maternal or fetal injuries) and their repair
-
Notifications that the pediatrician knows a VE has occurred
-
Report any other technical aspects of the procedure
Medical record is as follows:
-
If an obstetric program, card, or screen contains the information as listed above, an electronic record can replace the formal dictation
Birth Injuries
Neonatal injury
No assisted vaginal or cesarean delivery is entirely free of risk for mother and infant. [36, 37, 20, 38, 23] Important issues to consider include the magnitude of this risk and choices in procedures or techniques that might reduce risk once the natural processes of labor fail or if delivery must be expedited for maternal or fetal indications. As risk is considered, it must be judged against an appropriate control group with a similar clinical status and compared with an appropriate alternative procedure.
The reported incidence of fetal death or severe fetal injury from vacuum extraction is low, ranging from 0.1-3 cases per 1,000 extraction procedures. Birth trauma is the major complication of operative vaginal delivery. The most serious complication is intracranial hemorrhage. Other complications include hematoma, abrasion, laceration, nerve palsy, cephalohematoma, retinal hemorrhage, subgaleal hemorrhage, skull fracture.
The 2 major types of scalp injury associated with vacuum operations are the common, but clinically unimportant, cephalohematomas and the relatively rare, but potentially life-threatening, subgaleal hemorrhages (see the image below).
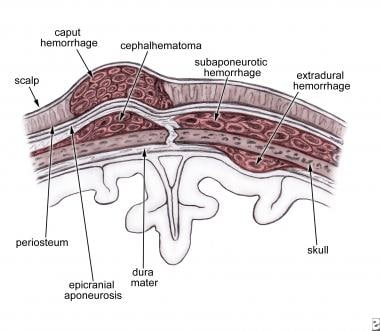
Scalp bruising or lacerations and retinal hemorrhages are usually insignificant fetal risks of extraction procedures.
When either radiographic or ultrasonic studies of the CNS are routinely performed on newborns who were delivered spontaneously or by instrumental assistance, minor trauma to the scalp, linear occult cranial fractures, and subarachnoid bleeding are discovered more frequently than are discovered by clinical signs and symptoms in the newborn. [39, 40]
Subgaleal and subaponeurotic hemorrhage
The most clinically concerning complication of VE is hemorrhage into the subgaleal (SG) or subaponeurotic space from rupture of the emissary veins. [41, 42, 37, 21, 23] This condition is potentially life threatening, with a mortality rate in identified cases reported as high as 20%.These bleeds happen occasionally after spontaneous delivery, but are most commonly associated with operative vaginal delivery. The reported incidence of clinically identified or symptomatic SG hemorrhages ranges from 0-50 per 1,000 VE operations. Judging from the largest series with close attention to neonatal condition, the higher reported rates do not reflect the rates of injury in modern practice when strict protocols for application and the limitation of effort are followed.
Of interest, SG bleeding was not observed in the large number of cases included in several major clinical reports in recent years. [26, 40] No SG cases were reported in the large VE meta-analysis by Johanson. [19] Also, in a report by Simonson et al, of 913 VE procedures, no instances of SG were reported in a study in which neonates were routinely screened postdelivery by cranial ultrasonography and radiography. [40] Further, the French study by Baume and coworkers involving 845 VE operations also did not report any clinically identified cases of SG hemorrhage. [26] These data document the rarity of such clinically significant severe scalp injuries when strict technical guidelines for the performance of VE operations are employed. Several atypical series aside, the best data from experienced practitioners indicates that the risk of symptomatic SG hemorrhage is quite small, although no clinician should ever assume that it is zero.
Because of the small but significant risk of SG bleeding, the attending pediatric personnel should be informed whenever a VE operation has occurred, regardless of the immediate condition of the neonate. SG hemorrhages are dangerous because the clinical signs and symptoms are often occult and insidious of onset. Clinically apparent difficulty may be delayed until some hours postpartum. Thus, serial observation is required.
Scalp bruising and lacerations
Ecchymoses and, uncommonly, scalp slough or lacerations can follow VE. Most of these injuries occur when the recommended 30-minute (some authors favor 20 minutes) limit to total cup application is exceeded or efforts are made at cup rotation (contraindicated). These injuries are now quite uncommon.
The vacuum is not a rotating instrument. Attempts at cup rotation to assist cranial rotation simply foster cup displacement, loss of station, or scalp injury.
Long-term neonatal outcomes
Studies evaluating both the general safety and the long-term neurologic sequelae of instrumental delivery reported no important differences in outcome between children delivered spontaneously versus those delivered by either VE or forceps. [43, 44, 45, 38, 46, 40, 47] Cohorts of children delivered by VE-assisted procedures versus spontaneous deliveries have been studied at intervals of up to 18 years. [45, 44] These children scored similarly in scholastic performance, speech, ability for self-care, and neurologic status. These latter long-term studies, although limited in total patient number and subject to flaws in completeness, provide reassurance of VE safety.
Maternal injury
Vacuum extraction has a low rate of maternal injury in comparison with forceps operations or cesarean delivery. However, maternal injuries do occur. Such trauma cannot be disregarded in evaluating the risk of the procedure. [26]
Lacerations
Maternal perineal lacerations are common complications of all operative vaginal deliveries. [26] Most significant tears are associated with episiotomy. Depending on series reflecting obstetric routines of perineal management and instrument use, the incidence of severe perineal lacerations (ie, third-degree and fourth-degree lacerations) during VE procedures ranges from 5-30%. Women who sustain vaginal lacerations in a previous delivery are at a significantly greater risk for a repeat laceration in subsequent deliveries. Women at greatest risk are those who experienced a laceration in the first delivery followed by another delivery combining both an instrumental delivery and an episiotomy. Delivery technique, skill, fetal bulk, prior scars, and instrument choice are important factors in perineal injury. [48, 49, 50, 51, 52, 53, 54, 55, 2]
One area in which the vacuum extractor has a clear advantage over forceps is the incidence of perineal trauma. Forceps operations are more likely to result in anal sphincter injury trauma than vacuum extractions. As noted, episiotomy is an important risk factor. Electively incising the perineum predisposes to perineal lacerations and rectal injuries by direct extension and therefore is not recommended. Mediolateral episiotomy has lower rates of extension, but is harder to repair and is associated with more post delivery pain than median episiotomy.
Episiotomy should not be routine and careful technique can often avoid tears, especially in multiparas. Best practice concerning whether to perform an episiotomy during an instrumental delivery, the type to use, and the timing is yet to be established. It is best avoided and if required, the type of perineal incision depends on the maternal anatomy and the station of the extraction effort.
Vacuum Extraction Versus Forceps
Forceps operations have become less popular, and vacuum extraction (VE) procedures are more common in recent years. There is long-term debate concerning when assisted delivery is appropriate and which instrument (vacuum extractor or forceps), is best. [56, 21, 57, 29, 6, 58, 38, 2, 20, 23] Although the instruments are largely interchangeable for most applications there are factors favoring the use of one instrument over the other. Important factors include the following:
-
Anesthesia: In general, low or outlet vacuum extraction (VE) operations are less uncomfortable for the mother than a forceps procedure from the same station. The meta-analysis reported by Johanson observed a significant reduction in the requirement for anesthesia with VE operations in comparison with forceps deliveries. [2] With a willing parturient, an uncomplicated VE can occasionally be performed with either a local, pudendal, or no anesthetic.
-
Instrument failure: VE operations are more likely to fail than forceps procedures. [59] The relative risk of failure with VE versus forceps operations is 1.69 (95% CI 1.31 to 2.19). The higher VE failure rate reflects a number of factors: poor instrument applications, incorrect vector of force in traction efforts, improper methods of applying traction, fetal malpositioning, poor choice of cases, and operator inexperience as well as the intrinsic inability of the vacuum extractor to exert as much force to the fetal head as forceps. [34, 60] The higher failure rate for VE operations is of concern in light of recent data regarding the risks of sequential instrument use when the application of forceps may follow a VE failure. In general, as mentioned above, infants from sequential instrument deliveries have worse outcomes than those delivered either by a cesarean delivery or by a vaginal procedure that was successful on the first attempt.
-
Maternal injury: Any instrumental delivery is associated with an increased risk of perineal/rectal injury versus the incidence of these complications following either a spontaneous or a cesarean delivery. A consistent finding is an increased incidence of perineal tears following forceps as opposed to VE deliveries. [51, 52, 2, 50, 54, 48, 31]
-
Fatal fetal injury: A study reported by Towner and coworkers collected mode of delivery and birth injury data from several large populations. [32] The report by Demissie and coworkers includes information from total United States births for 1995-8 (n= 11,939,388) as well as data from New Jersey (375,351). [36] These large numbers permit statistical evaluation of mortality information as most other studies have too restricted numbers due to the low incidence of fatal injury. These data indicate that delivery by VE is least as safe as forceps delivery with fatal complications in both cohorts statistically similar.
Other fetal injuries
Facial nerve (VII) palsies are more common following forceps operations (4.5 per 1,000) than VE procedures (0.46 per 1,000). [32] However, these injuries are uncommon, virtually always transitory and thus not of great clinical import.
Table 2. Incidence of Fetal Intracranial Hemorrhage (n=584,340) [32] (Open Table in a new window)
Mode of Delivery |
Incidence of ICH |
Cesarean delivery with no labor Spontaneous vaginal delivery |
1 per 2,750 1 per 1,900 |
Cesarean delivery during labor Vacuum-assisted vaginal delivery Forceps-assisted vaginal delivery |
1 per 907* 1 per 860* 1 per 664* |
Cesarean delivery after failed vacuum or forceps-assisted delivery |
1 per 334 |
*Differences not statistically significant |
|
Choice of instrument
Practice suggestions: The accoucheur must carefully consider the fetal condition, available resources, extent of analgesia, likelihood of maternal cooperation, and personal skill level when choosing the instrument for operative vaginal delivery. Recommendations are as follows:
-
Outlet-pelvic and low-pelvic operations (rotation < 45°): With adequate analgesia, the vacuum extractor and forceps are equivalent instruments. However, use of forceps is more likely to risk a maternal perineal injury. If a VE is chosen, any cup type is acceptable. The authors' recommendation is the use of a soft plastic cup to reduce scalp injury.
-
Rotations greater than 45° and midpelvic operations: For heads in transverse position, the appropriate cup choices include an occiput posterior (OP) metal cup or a rigid plastic or M-cup design. Forceps may also be used for these positions, but these operations are restricted to experienced physicians only. First, attempt a manual rotation because this may prove successful or partially successful either replacing the need for instrumentation or easing the subsequent procedure.
-
If an extraction is attempted from a direct OP position, appropriate choices include an OP metal cup or a rigid plastic or M-cup OP design. Forceps may also be applied to OP either for a direct "face to pubes" pull or, in experienced hands, for a rotation. Note that if the attempt is to deliver an OP infant directly, the pull can prove difficult and risks maternal soft-tissue injury. Forceps rotations from OP to OA (Scanzoni or similar procedures) are restricted to experienced accoucheurs only.
-
Instrumental deliveries that do not involve significant cranial asynclitism are equally well managed by any vacuum instrument. Note that VE is most likely to fail due to a deflexed OP presentation because of difficulty in proper placement of the vacuum cup. Also, in comparison to forceps, the vacuum extractor cannot exert the same level of traction that is possible with forceps.
Conclusion
Opinions for standard vacuum extraction procedures
The vacuum extractor is an effective and safe device for assisted vaginal delivery and an important addition to the modern obstetrical armamentarium. Proper education in the use of these devices is mandatory. The clinician must treat this instrument with respect to maximize the possibilities of its success while limiting the risks of maternal or fetal injury.
Routine notification of the pediatrician or the newborn attendants that a vacuum extraction (VE) operation has been performed is recommended to assure appropriate postoperative observation of the neonate.
Trauma to the maternal birth canal and perineum following instrumental delivery damages maternal pelvic nerves and fascial supports and can disrupt the anal sphincter, resulting in permanent pelvic floor injury or rectal dysfunction. The available data, although incomplete, prompts caution in instrumental deliveries to avoid episiotomy and perineal injury when possible.
The likelihood of serious infant injury is increased when multiple or excessive efforts at extraction are performed by either forceps or a vacuum extractor. An unsuccessful operation with any instrument should prompt great caution in applying an alternative device. Sequential instrument use is restricted to selected cases conducted only by highly experienced surgeons with the understanding that fetal risk is increased.
Routine practice
Key points for routine practice are as follows:
-
Informed consent is needed.
-
Limit the number of tractions with the VE to 4 or 5, with caution to ascertain true progress after 3.
-
Limit unintended cup detachments or pop-offs to no more than 2 or 3.
-
Require advancement of the presenting part with the initial or, certainly, the second traction.
-
Restrict the overall duration of the procedure to less than 30 minutes (note that some clinicians propose 20 min). Reduce vacuum between traction efforts.
-
Avoid sequential use of the vacuum extractor and forceps.
-
Abandon any procedure that proves difficult.
-
Dictate all procedures or record in an electronic medical record in the same manner as any operation.
Education
Traditionally, education in surgical procedures including forceps and vacuum extraction (VE) operations was based on the "see one, do one" method, in which the techniques of the surgery were taught at the perineum on actual cases. These clinical sessions were reinforced by practice on various pelvic models and review of textbook information. The most important part of the education was recognized to be in person clinical teaching. This model of education certainly does not apply in many services for numerous reasons.
Highly experienced OBGYNs are progressively lost to practice by death and retirement. "Practice" procedures performed for purposes of education are no longer performed. The overall use of instrumentation has declined, and many younger practitioners were never trained in the more complex types of vaginal instrumental delivery. Thus, educating a new series of practitioners has become difficult, and many clinicians depend entirely on outlet VE procedures only as they are uncomfortable or uncertain of their abilities to attempt higher extractions or conduct a forceps delivery.
The recent introduction of various methods of simulation of obstetric procedures is an important step in the right direction that has returned a method for "near clinical" forceps and VE procedures. The continuous improvement in these techniques and the development of better simulations will go a long way toward maintaining appropriate skills in this important part of obstetric lore.
-
Ghosting or phantom application of vacuum extraction.
-
Cranial flexion or pivot point.
-
Incorrect sites for cup placement.
-
Changing vector of traction.
-
Lateral view of maternal pelvis. Pelvic axis/curve is demonstrated.
-
Scalp cross-section and hemorrhage sites.
-
Digital evaluation of cranial molding.
-
Chignon sign.
Tables
Number of Traction Efforts |
Successful Malmström Vacuum Extractor Deliveries (n=433) |
Successful Forceps Deliveries† (n=555) |
1-2 |
296 (68.4%) |
213 (38.4%) |
3-4 |
108 (24.9%) |
270 (48.6%) |
≥5 |
29 (6.7%) |
72 (12.9%) |
* Breech, cesarean delivery, and transverse lies, are excluded. [30] † Type unspecified |
||
Mode of Delivery |
Incidence of ICH |
Cesarean delivery with no labor Spontaneous vaginal delivery |
1 per 2,750 1 per 1,900 |
Cesarean delivery during labor Vacuum-assisted vaginal delivery Forceps-assisted vaginal delivery |
1 per 907* 1 per 860* 1 per 664* |
Cesarean delivery after failed vacuum or forceps-assisted delivery |
1 per 334 |
*Differences not statistically significant |
|

What would you like to print?
- Introduction and History
- Prerequisites for Vacuum Extraction
- Indications for Vacuum Extraction
- Contraindications to Vacuum Extraction
- Design of the Vacuum Extractor
- Vacuum Extraction Technique
- Birth Injuries
- Vacuum Extraction Versus Forceps
- Conclusion
- Education
- Show All
- Media Gallery
- Tables
- References




