Background
The treatment of shock in a pregnant woman differs in two important respects from the treatment of shock in other adults. [1] First, normal physiologic changes occur in the most organ systems during pregnancy. Second, the mother and the fetus are both vulnerable during pregnancy. Therefore, obstetric critical care involves simultaneous assessment and management of the mother and fetus, who have differing physiologic profiles.
Shock is a state of compromised tissue perfusion that causes cellular hypoxia and is defined as a syndrome initiated by acute hypoperfusion, leading to tissue hypoxia and vital organ dysfunction (see the image below). It is a systemic disorder affecting multiple organ systems. Perfusion may be either decreased globally or distributed poorly, as in septic shock. During shock, perfusion is insufficient to meet the metabolic demands of the tissues; consequently, cellular hypoxia and end-organ damage ensue. [2, 3]
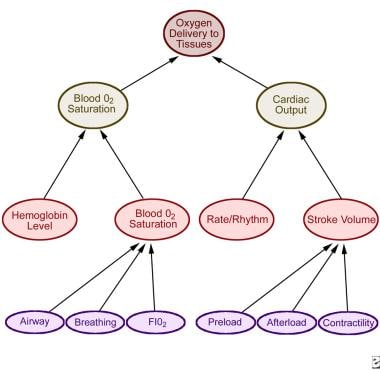 Determinants of cardiac function and oxygen delivery to tissues. Adapted from Strange GR. APLS: The Pediatric Emergency Medicine Course. 3rd ed. Elk Grove Village, Ill: American Academy of Pediatrics; 1998:34.
Determinants of cardiac function and oxygen delivery to tissues. Adapted from Strange GR. APLS: The Pediatric Emergency Medicine Course. 3rd ed. Elk Grove Village, Ill: American Academy of Pediatrics; 1998:34.
Cardiovascular Physiology During Normal Pregnancy
During pregnancy, significant cardiovascular changes occur, including changes in the blood volume, heart rate, stroke volume, cardiac output, and systemic vascular resistance. Furthermore, pregnant women also experience respiratory changes in lung volumes, minute ventilation, and acid-base status. Understanding and appreciating the normal physiologic adaptations to gestation are important for treating pregnant women.
Blood volume
Maternal blood volume increases from 25-52% by late pregnancy. [4] The plasma volume increases by 45-50%, compared with a 20% increase in red blood cell mass. This disproportionate increase in plasma volume accounts for the hemodilution or anemia of pregnancy, which is at its maximum by 32 weeks' gestation. The erythropoiesis occurs secondary to progesterone and other placental hormones. Elevated levels of estrogen and progesterone increase plasma aldosterone levels and renin activity; these promote sodium retention and an increase in total body water, the hypervolemia of pregnancy. During pregnancy, blood volume increases 1-1.5 L, total body sodium levels increase by 950 mEq/L, and the volume of total body water is 6-8 L, 4 L of which is extracellular. The expansion in blood volume and extracellular fluid volume is required for optimal uteroplacental circulation.
Blood pressure
Both the systolic and diastolic blood pressures decrease until mid pregnancy, with gradual recovery to nonpregnant values by late gestation. [5, 6] The blood pressure decrease likely occurs because of decreased vascular resistance. In pregnancy, interpret the blood pressure relative to gestational age. A blood pressure measurement of 130/80 mm Hg may be normal at term but is abnormal at 28 weeks' gestation, when it should be approximately 110/60 mm Hg. The venous pressure in the legs increases progressively during pregnancy, caused by compression of the pelvic veins and inferior vena cava by the uterus. The elevated femoral venous pressure returns to a normal level following labor.
The measurement of brachial artery pressure is not indicative of the uterine arterial blood pressure because the uterine arterial pressure can be extremely low, even when the blood pressure measurement of the arm is normal.
Heart rate
The maternal heart rate becomes elevated by 12 weeks' gestation; this reaches and stays at 120% of the baseline by 32 weeks of pregnancy. [7] The maternal tachycardia may be secondary to cardiac adaptation to volume overload and elevated free thyroxine serum levels.
Cardiac output and stroke volume
Maternal cardiac output increases 30-50% during pregnancy. [8, 9] This increase occurs by 10 weeks' gestation and peaks at the end of the second trimester. The increase in cardiac output during gestation is the result of an increase in heart rate and stroke volume. In the first half of pregnancy, the stroke volume is increased primarily as the uteroplacental circulation acts as an arteriovenous shunt. In late pregnancy, the cardiac output is increased due to the tachycardia rate. [10] Alternative hypotheses for the increase in left ventricular stroke volume have been suggested; the ventricular pressure volume curve may be shifted to the right because of a hormonally dilated heart, thereby increasing diastolic filling.
Systemic vascular resistance
Systemic vascular resistance decreases and reaches a nadir by the 24th week of pregnancy, with a progressive rise toward the baseline value at term. The 2 important factors that reduce systemic vascular resistance are the dilatation of peripheral blood vessels and the presence of the placental circulation. The placental vascular bed is a low-resistance vascular system perfused with a large portion of the maternal cardiac output. Uterine veins increase enormously in size and number during gestation, and uterine vascular resistance is greatly decreased during pregnancy.
Effect of maternal posture on maternal hemodynamics
The uterine blood flow increases from approximately 50 mL/min prepregnancy to 500 mL/min at term; this represents a change of systemic cardiac output from 2% normally to 18% during the third trimester. [11, 12] A pregnant woman has a greater tendency for pooling of venous blood; marked hypotension and syncope may be experienced with sudden standing from a sitting or lying position. The supine hypotensive syndrome manifests as dizziness, pallor, tachycardia, sweating, nausea, and hypotension that occur when a pregnant woman lies on her back. The heavy gravid uterus compresses the descending aorta and the inferior vena cava. This results in pooling of blood in the legs, a decrease in venous return to the heart, a fall in cardiac output, and hypotension. Nonreassuring fetal status may occur from decreased uteroplacental perfusion. Turning the mother to her side quickly restores the pooled blood to the circulation.
Intrapartum hemodynamics
Maternal cardiovascular responses can be further modified by uterine contractions, pain, labor, analgesia, surgery, and peripartum blood loss. Cardiac output increases during various phases of labor. The uterine contractions augment cardiac output. Each uterine contraction expresses from 300-500 mL of blood. [13] The infusion of blood back into the maternal circulation increases venous return and augments stroke volume. The magnitude of cardiac output gained during contraction is 11% less in women laboring under epidural analgesia. [14] This concept is important for patients with cardiac disease who may not tolerate hemodynamic fluctuations during labor.
Approximately 500 mL of blood loss occurs with vaginal delivery and 1000 mL with cesarean delivery. [15] The hypervolemia of pregnancy allows women to lose as much as 30% of predelivery blood volume, with little change in postpartum hematocrit values. Postpartum diuresis peaks between the second and fifth day after delivery, resulting in 3 kg of weight loss during the first week. Maternal cardiac output increases by approximately 20-30% above prelabor values during the first 24 hours following delivery. [16] Cardiac output remains elevated for at least 48 hours postpartum due to the stroke volume increase despite maternal bradycardia. The return of blood volume from the lower extremities results in approximately 1 L of autotransfusion at the time of delivery. [17]
Respiratory Physiology
Anatomic changes
Hormonal changes in pregnancy affect the upper respiratory tract and airway mucosa, producing hyperemia, mucosal edema, hypersecretion, and increased mucosal friability. Estrogen is probably responsible for producing tissue edema, capillary congestion, and hyperplasia of mucous glands.
The enlarging uterus and the hormonal effects produce anatomic changes to the thoracic cage. As the uterus expands, the diaphragm is displaced cephalad by as much as 4 cm; an increase in the anteroposterior diameter and transverse diameter of the thorax occurs, increasing the chest wall circumference. Diaphragm function remains normal, and diaphragmatic excursion is not reduced.
Pulmonary functions
Anatomic changes to the thorax produce a progressive decrease in functional residual capacity (FRC), which is reduced by 10-20% by term. The residual volume can decrease slightly during pregnancy, but this finding is not consistent; a decreased expiratory reserve volume is a definite change. The increased circumference of the thoracic cage allows the vital capacity to remain unchanged, and the total lung capacity decreases only minimally by term. Hormonal changes do not significantly affect airway function; pregnancy does not appear to change lung compliance, but chest wall and total respiratory compliance are reduced at term. [18, 19, 20]
Ventilation
The minute ventilation increases significantly, beginning in the first trimester and reaching 20-40% above baseline at term. Alveolar ventilation increases 50-70%. The increase in ventilation occurs because of increased metabolic carbon dioxide production and an increased respiratory drive due to the increased serum progesterone level. The tidal volume increases 30-35%. The respiratory rate remains relatively constant or increases slightly.
Arterial blood gases
Physiologic hyperventilation results in respiratory alkalosis with compensatory renal excretion of bicarbonate. The arterial carbon dioxide pressure reaches a plasma level of 28-32 mm Hg, and bicarbonate is decreased to 18-21 mmol/L, maintaining an arterial pH in the range of 7.40-7.47. Mild hypoxemia might occur in the supine position. Oxygen consumption increases at the beginning of the first trimester and increases 20-33% by term because of fetal demands and increased maternal metabolic processes. [21]
In active labor, hyperventilation increases and tachypnea caused by pain and anxiety might result in marked hypocapnia and respiratory alkalosis, adversely affecting fetal oxygenation by reducing uterine blood flow. In some patients, severe pain and anxiety can lead to rapid, shallow breathing with alveolar hypoventilation, atelectasis, and mild hypoxemia.
Uteroplacental and Fetal Physiology
A basic understanding of fetal physiology is required to care for pregnant patients who are critically ill. The fetal oxygen delivery is dependent on maternal arterial oxygen content and uterine blood flow. The uterine blood flow increases during pregnancy from 2% of cardiac output in a nonpregnant patient to 18% of cardiac output by the third trimester in a pregnant patient. Therefore, factors affecting either the arterial oxygen content or uterine blood flow also affect fetal oxygenation. These factors are hypotension, vasoconstriction of the placental bed, and uterine contractions. The causes of hypovolemia include supine position, hypovolemia, sepsis, and medications.
Vasoconstriction of the uterine arteries occurs in preeclampsia [22] or with vasoconstrictor drugs, and the fetal blood flow may decrease by as much as 20% with vasoconstriction. The umbilical vein PaO2 is approximately 35-40 mm Hg because it is mixed with deoxygenated blood in the fetal inferior vena cava. This level of PaO2 is sufficient to saturate fetal hemoglobin to 80-85% because of the left shift in the oxyhemoglobin dissociation curve. The oxygen consumption of the fetus is 20 mL/min, and the oxygen reserve is approximately 42 mL. However, the fetus has the capability of surviving longer by redistributing blood flow to the vital organs. A 50% decrease in uterine blood flow may be tolerated for brief periods, and further reduction produces anaerobic metabolism, brain damage, and fetal death. [23]
Determinants of fetal oxygen delivery
Oxygen delivery to fetal tissues can be affected at many levels (maternal oxygen delivery to the placenta, placental transfer, and oxygen transport from the placenta to fetal tissues). The major determinants of oxygen delivery to the placenta are the following:
-
The oxygen content of uterine blood, which is determined by maternal PaO2
-
Maternal hemoglobin concentration and saturation
-
Uterine blood flow, which depends on maternal cardiac output
Thus, a decreased PaO2 in the mother can be offset somewhat by augmentation of the blood hemoglobin concentration or cardiac output. A combination of maternal hypoxemia and decreased cardiac output has a profoundly deleterious effect on fetal oxygenation.
Variations in maternal pH also influence oxygen delivery; alkalosis causes vasoconstriction of the uterine artery, resulting in decreased fetal oxygen delivery.
The interaction of maternal and fetal circulations in the placenta most likely follows a concurrent exchange mechanism. This is less efficient than a countercurrent exchange mechanism and helps explain why the PaO2 of the fetal umbilical vein is in the range of 32 mm Hg, far lower than the uterine vein PaO2. Despite low umbilical vein PaO2, fetal oxygen content is actually quite close to maternal oxygen content because of the shape of the oxyhemoglobin saturation curve of the fetal hemoglobin.
The other placental factors that determine fetal oxygenation are the amount of intraplacental shunt, the degree of matching of maternal and fetal blood flow, and the presence of any placental abnormalities, such as placental infarcts. The fetal arterial blood has an even lower PaO2 than umbilical vein blood. This is partially compensated by a high fetal cardiac output relative to oxygen consumption, thus maintaining abundant oxygen delivery to the tissues. The umbilical vein PaO2 values of less than 30 mm Hg are saturated on the steep part of the fetal oxyhemoglobin dissociation curve; therefore, small changes in maternal PaO2 may cause significant changes in fetal oxygen content. [23]
Fetal monitoring
Fetal monitoring is performed via continuous electronic fetal heart rate (FHR) monitoring to identify any changes in fetal physiology. The baseline FHR is in the range of 120-160 beats/min. Although fetal tachycardia may be a nonspecific finding, fetal bradycardia may indicate hypoxia secondary to uteroplacental insufficiency. Absence of beat-to-beat variability in the FHR may be another indication of fetal asphyxia and anemia. While early decelerations of FHR are benign, late or variable decelerations are highly suggestive of fetal hypoxia, particularly when they are recurrent and combined with decreased variability.
Abnormalities of FHR patterns may be further evaluated by using results from a fetal biophysical profile. The fetal biophysical profile consists of an ultrasound determination of fetal movements, fetal breathing movements, limb tone, amniotic fluid volume, and reactivity to nonstress testing. Fetal acid-base measurements from scalp blood sampling are used in labor to assess the state of fetal physiology. A pH less than 7.20 indicates fetal hypoxia, whereas a pH greater than 7.25 predicts a favorable outcome. Fetal pH monitoring can be performed only when membranes are ruptured.
Fetal oxygen saturation is a new intrapartum fetal monitoring technology, which is expected to provide a more complete and accurate assessment of the fetal condition. This technique directly and objectively measures fetal oxygen status during labor and delivery. Fetal pulse oximetry has been approved for use with the conventional fetal monitor only in patients with nonreassuring heart rates. Because the degree of nonreassuring rates differs, fetal pulse oximetry requires further study to assess its role in the management of different clinical situations.
Critical Care Monitoring and Support of the Pregnant Patient
The pregnant patient is unique in an intensive care environment. A pregnant patient who is critically ill and in shock requires special expertise because of the extraordinary underlying physiology.
Intubation and mechanical ventilation
During pregnancy, the nasopharyngeal, oropharyngeal, and respiratory tract mucosa swell. Therefore, intubation and suctioning may lead to mucosal injury and bleeding. Endotracheal intubation must be performed quickly because pregnant patients have lower oxygen reserves because of the decrease in functional residual capacity (FRC). Ventilate pregnant patients to maintain their PaCO2 at approximately 30 mm Hg, which is the normal level during pregnancy. Avoid respiratory alkalosis because it may decrease uterine blood flow and, hence, fetal oxygenation. Avoid high ventilatory pressures at the expense of a rise in PaCO2; maternal hypercapnia has not been reported to be harmful to the fetus.
Cardiopulmonary resuscitation
In an arrest situation, place pregnant patients in a left lateral tilt position to avoid supine hypotension. This can be achieved by placing a pillow or wedge under the patient's right hip. Advanced cardiac life support (ACLS) is provided according to ACLS standard protocols. The precipitating events for cardiac arrest in pregnancy include amniotic fluid embolism (AFE), pulmonary embolism (PE), cardiomyopathy, anesthetic complications, myocardial infarction, and magnesium overdose.
Hemodynamic monitoring
Pregnant patients who are critically ill and in shock may require insertion of a pulmonary artery catheter. The indications for pulmonary artery catheterization are severe preeclampsia with oliguria, pulmonary edema, severe cardiac disease, acute respiratory distress syndrome (ARDS), septic shock, and AFE. In normal pregnancy, the cardiac output increases as much as 30-50%, as compared to prepregnancy levels, but the cardiac filling pressures are unchanged.
Drug therapy
For sedation, meperidine and fentanyl are commonly used; experience with propofol is limited. Benzodiazepines may be used, but these may have depressive effects on fetal respiration.
A patient who is critically ill and in shock requires vasoactive drugs. Insufficient human data are available to assess the effects of these drugs in pregnancy and labor. Animal data suggest that dobutamine, norepinephrine, and epinephrine adversely affect uterine blood flow. Dopamine and ephedrine have been shown to increase maternal blood pressure and uterine flow. The pure alpha-adrenergic agents, such as phenylephrine and norepinephrine, cause vasoconstriction of uterine arteries and should be avoided if possible. Ephedrine, which has both beta-2 properties and alpha-1 agonist properties, is known to increase uterine blood flow and maternal blood pressure. It is the vasoactive drug of choice to treat hypotension in pregnant patients.
Hemorrhagic Shock
Trauma and resultant hemorrhage cause 6-7% of all deaths in pregnancy. The cause of trauma in pregnancy includes vehicular accidents, falls, assaults, and penetrating injuries. Placental abruption occurs in 1-5% of patients with minor trauma and in 20-50% of patients with major trauma. In the United States, obstetric hemorrhages are responsible for 13.4% of all maternal deaths. [24] Antepartum hemorrhage can occur from disruption of the placenta and spontaneous or traumatic uterine rupture. [25, 26]
Placenta previa is implantation of the placenta in the lower uterine segment, with a classic presentation of painless vaginal bleeding and a soft, nontender uterus. Placental abruption may occur in a normally implanted placenta, manifesting as uterine pain and hemorrhage. The uterine pain is present between contractions, and the uterus is tender.
The signs and symptoms of uterine rupture include vaginal bleeding, lower abdominal pain, and a nonreassuring fetal tracing. Uterine rupture commonly occurs when high doses of oxytocin or prostaglandins are infused for induction. [27] The uterine fundus feels boggy and tender upon palpation. Most obstetric hemorrhages occur postpartum and are primarily due to uterine atony and cervical or vaginal lacerations; antepartum hemorrhage is less common.
Postpartum hemorrhage may be worsened by thrombocytopenia, coagulopathy secondary to AFE, or sepsis. The normal blood loss of vaginal delivery (500 mL) or cesarean delivery (1000 mL) is generally well tolerated. Excessive blood loss results in hypovolemic shock; in an antepartum patient, excessive blood loss diminishes uteroplacental blood flow and induces fetal distress.
Management
The management of hemorrhagic shock requires immediate resuscitative measures, including administration of oxygen, placement of 2 intravenous lines, intravenous volume replacement, and blood typing and crossmatching to replace packed red blood cells. [28] In emergencies, blood that is type-specific and is not crossmatched can be administered. Once the patient is stable, an abdominal ultrasound is performed immediately to definitively diagnose the cause of uterine bleeding. The ultrasound confirms whether the hemorrhage is due to placenta previa or placental abruption. Patients requiring a large amount of volume replacement may develop coagulopathy, which should be treated with appropriate blood product support. Fetal monitoring should be performed via continuous fetal heart rate (FHR) monitoring to detect fetal distress or fetal hypoxia, the presence of which should lead to prompt fetal delivery by the safest possible method.
In postpartum hemorrhage, uterine atony can be treated with uterine massage, intramuscular administration of methylergonovine (0.2 mg), and intravenous oxytocin infusion. Oxytocin is the first-line drug and is often administered as an infusion (20-40 U/L), because bolus administration can cause peripheral vasodilation, tachycardia, and hypotension. The next step is prostaglandin administration; prostaglandins increase myometrial intracellular free calcium concentrations and enhance the activity of other oxytocic agents. Hemabate (15-methyl prostaglandin F2-alpha) is the most frequently used agent and is administered at a dosage of 250 mcg intramuscularly every 15-30 minutes as necessary (not to exceed 2 mg).
Adverse effects include bronchospasm, ventilation-perfusion mismatch, and hypoxemia. Ergonovine and methylergonovine are the ergot alkaloids that produce rapid tetanic uterine contraction and are used to treat refractory uterine atony. The dose is 0.2 mg intramuscularly. These drugs can cause serious cardiovascular problems, such as hypertension, vasoconstriction, and increased pulmonary artery pressures.
If medical management fails, therapeutic embolization of the internal iliac or uterine artery has been used to control obstetric hemorrhage. Surgical exploration to repair lacerations and decrease blood loss by arterial ligation or hysterectomy may be required as a life-saving measure.
Transcatheter arterial embolization has been a recognized method of hemorrhage control and has been used successfully in the control of postpartum hemorrhage. Several advantages of uterine artery embolization include easy identification of the bleeding site, preservation of the uterus and fertility, and decreased rebleeding from collaterals. One review revealed a success rate of 94.9% and a complication rate of 8.7% in 138 cases of postpartum hemorrhage treated by arterial embolization. The most common complication is low-grade fever, but rarely, pelvic infection, groin hematoma, iliac artery perforation, transient buttock ischemia, transient foot ischemia, and bladder gangrene may occur.
Septic Shock
Septic shock may occur during pregnancy because of overwhelming infection caused by gram-positive bacteria, viruses, or fungi. [29] Gram-negative bacteria such as Escherichia coli, Klebsiella species, Pseudomonas aeruginosa, and Serratia species cause most cases of septic shock. The microorganisms produce endotoxins that activate complement systems and cytokines, initiating an inflammatory response. The mediators of sepsis are responsible for vasodilation, low peripheral vascular resistance, and hypotension. Furthermore, blood flow is poorly distributed, resulting in inadequate perfusion of certain organs, leading to cellular damage, multiorgan failure, and death.
The mediators of inflammation result in increased capillary permeability, causing leakage of intravascular fluid throughout the body, specifically the pulmonary parenchyma, and resulting in noncardiac or low-pressure pulmonary edema. During sepsis, injury to type II pneumocytes impairs surfactant production, causing alveolar collapse, lowering lung compliance, and producing severe hypoxemia. This constellation of clinical and physiologic features is described as acute respiratory distress syndrome (ARDS)
The causes of septic shock are septic abortion, chorioamnionic and postpartum infections, pyelonephritis, and respiratory tract infections. [30] Although septic shock remains one of the major causes of death in obstetric patients, the incidence of death in obstetric patients with septic shock is lower than that in nonobstetric patients with septic shock (0-3% in obstetric patients vs 10-80% in nonobstetric patients). Prolonged rupture of membranes, retained products of conception, and instrumentation of the genitourinary tract are other significant risk factors for sepsis. Patients with septic shock present with chills, fever, hypotension, mental confusion, tachycardia, tachypnea, and flushed skin. As the septic shock progresses, the patient develops cool clammy skin, bradycardia, and cyanosis. [31]
Intravaginal mifepristone in medical abortions has resulted in fulminant and lethal septic shock due to Clostridium sordellii, a gram-positive, toxin-forming anaerobic bacteria. By blocking both progesterone and glucocorticoid receptors, mifepristone interferes with the release and function of cortisol and cytokines. Thus, the failed release of cortisol and cytokine responses impairs the body's defense mechanism, which is necessary to prevent the endometrial spread of C sordellii infection. Concomitant release of potent exotoxins and an endotoxin from C sordellii contribute to the rapid development of lethal septic shock.
Treatment
Treatment of septic shock requires immediate resuscitation, identification of the underlying cause of septic shock, and treatment with antimicrobial therapy. [32, 33] Cultures of sputum, blood, and urine are sent before antibiotic administration. Provide empiric antibiotic coverage intravenously for both gram-negative and gram-positive bacteria. Later, antibiotic therapy is adjusted based on the patient's response to therapy and the results of culture and sensitivities. In puerperal sepsis, also provide anaerobic coverage. A combination used often is penicillin, aminoglycoside, and clindamycin or metronidazole. An alternative combination is a second- or third-generation cephalosporin combined with metronidazole. Piperacillin-tazobactam provides fairly comprehensive coverage for an intra-abdominal source of sepsis.
In septic shock, adequate tissue oxygenation should be maintained. Optimum mean arterial pressure, circulating blood volume, cardiac output, and sufficient oxyhemoglobin saturation are required. Patients in respiratory distress or those with severe hypoxemia may need to be intubated and mechanically ventilated. Because patients with septic shock often develop ARDS, the goals of mechanical ventilation are the use of a low tidal volume and a high positive end-expiratory pressure. This approach results in recruitment of alveoli, makes the lungs more compliant, and improves oxygenation.
Patients in septic shock require hemodynamic support with restoration of adequate circulating volume, followed by the administration of vasoactive drugs. These patients require aggressive resuscitation with crystalloids and colloids to maintain sufficient intravascular volume before considering vasopressor therapy. Although dopamine has been used in the past in patients with septic shock, norepinephrine achieves better perfusion pressure and maternal hemodynamics and helps restore oxygen delivery to hypoperfused organs. This may be achieved at a cost of reduced uterine blood flow. Ephedrine, an alpha and beta agonist, may be the preferred vasopressor in patients with acute hypotension during pregnancy.
In summary, the principles of management of septic shock include the following components:
-
Early recognition
-
Early and adequate antibiotic therapy
-
Source control
-
Early hemodynamic resuscitation and continued support
-
Corticosteroids (refractory vasopressor-dependent shock)
-
Glycemic control
-
Proper ventilator management with low tidal volume in patients with ARDS
Other Causes Of Shock In Pregnancy
Cardiogenic shock
Cardiogenic shock may also be observed during pregnancy. [34] The major cause of cardiogenic shock is severe valvular disease. In cardiogenic shock, the left ventricle is not able to pump sufficient blood to meet the metabolic demands of the tissues. The compensatory response is tachycardia, but eventually, hypervolemia, pulmonary venous congestion, and generalized edema occur. Inadequate oxygen delivery leads to cellular damage, multiorgan failure, and death. The clinical signs of cardiogenic shock are distended neck veins, dyspnea, tachypnea, the presence of a third heart sound, systolic or diastolic murmurs, and generalized edema.
Peripartum cardiomyopathy is an idiopathic disorder that occurs during the last month of pregnancy and up to 6 months postpartum. The incidence of this disease is 1 case in 1500-4000 deliveries. The risk factors include old age, multiparity, twin gestation, and preeclampsia. Upon presentation, these patients have signs and symptoms of congestive heart failure. The mortality associated with peripartum cardiomyopathy is 25-50%. [35] This disease tends to recur in subsequent pregnancies. A small percentage of these patients are found to have inflammatory myocarditis after analysis of endomyocardial biopsy specimens. The treatment consists of diuretics, vasodilators for afterload reduction, digoxin, and careful follow-up. Inflammatory myocarditis may respond to immunosuppressive therapy.
Postpartum patients may have a localized abscess, resistant organism, or septic pelvic thrombophlebitis. Patients with septic pelvic thrombophlebitis usually develop persistent fever; the diagnosis may be suggested by findings from a CT scan of the pelvis. Treatment consists of a broad spectrum of antibiotics and standard anticoagulation.
Coronary artery disease is uncommon in reproductive-aged women, but myocardial infarction has occurred because of the excessive hemodynamic stress of pregnancy. Management of coronary artery disease in a pregnant patient is similar to that in a nonpregnant patient.
Spontaneous coronary artery dissection, a rare event, causes myocardial ischemia and sudden death in younger age groups and especially postpartum women. The clinical presentation includes angina, myocardial infarction, cardiogenic shock, and death. No specific cardiac risk factors have been associated with its occurrence. In postpartum patients, the possible mechanism for dissection is thought to be pregnancy-induced degeneration of collagen and the additional stresses of parturition. The treatment is usually tailored to the individual patient's needs.
Amniotic fluid embolism
Amniotic fluid embolism (AFE) is a catastrophic peripartum syndrome that manifests as a sudden onset of severe dyspnea, hypoxemia, hemodynamic collapse, coagulopathy, and seizures. AFE is a rare disorder, occurring in 1 case in 20,000-30,000 pregnancies, but it accounts for 10% of all maternal deaths. [36] AFE may occur at any point during pregnancy, labor, or delivery. Uterine manipulation or trauma may often precede AFE. Whether the pathogenesis occurs secondary to embolization of particulate cellular contents or secondary to humoral factors has not been established.
An analysis of 46 verified cases of AFE had none of the previously cited predisposing factors: 12% of the cases occurred in women with intact membranes, 70% during labor, 11% after vaginal delivery, and 19% during cesarean delivery with or without labor.
The fetal substance may initiate an anaphylactoid reaction, resulting in endogenous mediator release and causing hypotension, tachycardia, hypoxemia, and seizures. This may lead to pulmonary arterial vasospasm and transient pulmonary hypertension, followed by left ventricular failure, decreased cardiac output, and hydrostatic pulmonary edema. The acute left ventricular dysfunction may be caused by humoral mediators or cytokines contained in amniotic fluid released during the anaphylactoid reaction.
AFE is extremely difficult to predict or prevent. Although most cases occur after the onset of labor, some may occur outside of labor. Respiratory distress and cyanosis occur suddenly within the first few minutes and are quickly followed by hypotension, pulmonary edema, shock, and neurologic manifestations, such as confusion, loss of consciousness, and seizures. More than 80% of patients experience cardiorespiratory arrest at the outset. Approximately 50% of patients do not survive this cardiopulmonary catastrophe, but of those who do, 40-50% develop coagulopathy and hemorrhage up to 4 hours later, and this may well be the first indication of AFE. Seizure activity may, at times, be the first manifestation.
The diagnosis of AFE is based on a characteristic clinical picture. Treatment consists of oxygenation and hemodynamic support. Patients often require invasive monitoring to assess the adequacy of intravascular volume status and to guide inotropic therapy. Corticosteroids have been used, but their benefit has not been established. The mortality rate for AFE is high: 86% of patients may succumb to this disorder. Approximately 40% of cases have fetal death at the time of presentation, and placental abruption occurs in 50% of the cases.
Management includes supportive measures and should begin emergently. The initial principles of dealing with obstetric emergencies include airway, breathing, and circulation. The 3 main goals of treatment are (1) oxygenation, (2) maintaining cardiac output and blood pressure, and (3) correcting coagulopathy. The fetus should be monitored continuously for signs of compromise. To ensure optimal uterine perfusion, the mother should be placed in the left lateral position.
The first priority is resuscitation of the mother and administration of oxygen (100% concentration). The patient may need to be intubated and ventilated. The initiation of fluid therapy and the administration of pharmacologic agents to maintain optimal blood pressure and cardiac output is the next step. Volume replacement and therapy for left ventricular dysfunction should be directed toward improving inotropy. A clinical guideline is to maintain the systolic blood pressure at 90 mm Hg or higher, with acceptable organ perfusion, as indicated by a urine output of 25 mL/hr or more. Administration of blood transfusions and blood components is considered the first line of treatment for correcting coagulopathy associated with AFE. Intravenous steroids to treat underlying inflammatory response and similarities of AFE to anaphylaxis may be helpful.
Pulmonary embolism
The risk of developing deep venous thrombosis (DVT) and pulmonary embolism (PE) increases markedly during the advanced stages of pregnancy and is greatest during postpartum. Rates of maternal mortality from PE have been reported at 2.6 cases per 100,000 live births in white females and 2.5-fold higher in black females. Incidence increases markedly following cesarean delivery, as compared to vaginal delivery. [37] The signs and symptoms of PE are more problematic because dyspnea and tachypnea are common in pregnancy. In nonpregnant patients, tachypnea, dyspnea, chest pain (pleuritic), apprehension, and crackles are present in only 50% or more of patients. Chest radiographic findings are abnormal in 80% or more of patients with PE, and the findings are nonspecific. Electrocardiographic findings are abnormal in 70% of patients with PE, but they are nonspecific. Arterial oxygen tension is low in most patients with PE.
Objective diagnostic testing
As with DVT, PE requires objective diagnostic testing to confidently confirm or exclude the diagnosis. This is particularly true in pregnancies, because the diagnosis of DVT or PE requires the following:
-
Prolonged therapy (potentially heparin for the entire 40 weeks of pregnancy)
-
Prophylaxis during future pregnancies
-
Avoidance of oral contraceptive pills
The first objective diagnostic test should be compression ultrasonography; if it is not available, impedance plethysmography is adequate. If findings from the noninvasive leg studies are negative, proceed to ventilation-perfusion lung scanning. Perfusion scanning alone is recommended initially, adding ventilation scanning when perfusion defects are noted. Pulmonary angiography might be necessary if lung scan findings are of low probability or indeterminate but clinical evidence is strong.
Several studies show no increased risk of teratogenicity in patients undergoing radiologic procedures for the diagnosis of maternal venous thromboembolic disease. A complete and adequate evaluation to document the presence or absence of PE requires less than 0.005 Gy. Obtaining the appropriate diagnostic study in pregnancies is mandatory.
Management
Immediately treat patients, pregnant or not, in whom PE is strongly considered. Treatment is with intravenous unfractionated heparin, unless the patient has a high risk or contraindication to the use of any anticoagulants. Extensive clinical experience and cohort studies have established that heparin is the safest anticoagulant to use during pregnancy, because it does not cross the placenta. The initial loading dose should be 5000-10,000 U. Following loading, an infusion of 18 U/kg is started. Monitor and keep the activated partial thromboplastin time in the therapeutic range, which is 1.5-2 times the baseline value.
Although data are relatively modest, low-molecular-weight heparin (LMWH), which does not cross the placenta, can be administered once a day and does not require monitoring. LMWH has not been shown to have an increased risk of bleeding with surgical procedures, including cesarean deliveries, in a small number of patients. In one report, dalteparin was used safely and effectively for prophylaxis in 47 women throughout their pregnancies. The recommended dose was 5000 U, once or twice daily, with a target trough plasma heparin level of 0.1-0.2 U/mL.
However, data on the use of LMWH during pregnancy are limited; most come from diverse case series involving prophylaxis rather than therapy. These data provide no clear conclusions as to the efficacy and adverse effects of LMWH; no optimal dose regimen; and insufficient information on risks of obstetric, fetal, or neonatal problems. Additionally, cases of epidural hematoma have occurred after epidural anesthesia.
Warfarin should be avoided throughout pregnancy because it can cause embryopathy characterized by intellectual disability, optic atrophy, cleft lip, cleft palate, cataracts, and hemorrhage. The teratogenic effects are particularly common during the first trimester. Warfarin crosses the placenta; it can cause fetal and neonatal hemorrhage and placental abruption.
Vena cava filters (Greenfield, stainless steel or titanium; bird's nest; Simon-Nitinol) are positioned within the infrarenal inferior vena cava to trap thrombi arising from the lower extremities. Patients with documented venous thromboembolic disease who have contraindications to anticoagulation therapy or in whom conventional therapy has failed are candidates for inferior vena cava filter placement. Vena cava filters and filter placement are associated with a favorable safety profile; however, both fatal and nonfatal complications have been reported. Fatal complications are rare, and most nonfatal complications are of minimal clinical significance.
Duration of anticoagulation
Patients who develop DVT or PE antepartum should receive anticoagulation therapy with heparin throughout pregnancy. After delivery, warfarin should be started; the heparin can be discontinued once an adequate international normalized ratio (INR) is achieved. Continue the warfarin for at least 6 weeks postpartum or until at least 3 months of anticoagulant therapy have been completed.
Complications of treatment
Osteopenia has been reported with unfractionated heparin administered for more than 6 months. No information is available about the beneficial effects of concomitant multivitamins, calcium, or vitamin D supplementation. The problem of osteopenia and osteoporosis might be less severe if LMWH is used, but providing optimum calcium and vitamin D supplementation to all patients receiving long-term heparin administration during pregnancy is reasonable.
-
Determinants of cardiac function and oxygen delivery to tissues. Adapted from Strange GR. APLS: The Pediatric Emergency Medicine Course. 3rd ed. Elk Grove Village, Ill: American Academy of Pediatrics; 1998:34.





