Practice Essentials
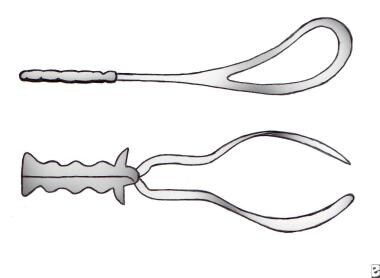
Forceps are instruments designed to aid in the delivery of the fetus by applying traction to the fetal head. Many different types of forceps have been described and developed. Generally, forceps consist of 2 mirror image metal instruments that are maneuvered to cradle the fetal head and are articulated, after which traction is applied to effect delivery.
Forceps have 4 major components, as follows:
-
Blades: The blades grasp the fetus. Each blade has a curve to fit around the fetal head. The blades are oval or elliptical and can be fenestrated (with a hole in the middle) or solid. Many blades are also curved in a plane 90° from the cephalic curve to fit the maternal pelvis (pelvic curve).
-
Shanks: The shanks connect the blades to the handles and provide the length of the device. They are either parallel or crossing.
-
Lock: The lock is the articulation between the shanks. Many different types have been designed.
-
Handles: The handles are where the operator holds the device and applies traction to the fetal head.
See the image below.
History of the Procedure
The history of obstetrical forceps is long and, often, colorful. Sanskrit writings from approximately 1500 BC contain evidence of single and paired instruments; Egyptian, Greek, Roman, and Persian writings and pictures refer to forceps that were originally used for extraction following fetal demise to save the mother’s life.
The credit for the invention of the precursor of the modern forceps to be used on live infants goes to Peter Chamberlen of England (circa 1600). Modifications have led to more than 700 different types and shapes of forceps. In 1745, William Smellie described the accurate application to the occiput, rather than the previously performed pelvic application, regardless of the position of the head. In 1845, Sir James Simpson developed a forceps that was designed to appropriately fit both cephalic curvatures and pelvic curvatures. In 1920, Joseph DeLee further modified that instrument and advocated the prophylactic forceps delivery. In an era in which many women labored and delivered under heavy sedation, forceps deliveries became common.
In current obstetrical practice, the use of forceps has become much less common. Clinical studies performed before the 1970s suggested that the risk of fetal morbidity and mortality was higher when the second stage of labor exceeded 2 hours. [1] With contemporary obstetrical management, morbidity rates no longer increase with longer labors if fetal surveillance is reassuring. Thus, the length of the second stage of labor alone is no longer an absolute indication for operative termination of labor, although it remains an indication in the American College of Obstetricians and Gynecologists (ACOG) publications. [2]
Other factors were also at work to decrease the use of forceps deliveries. In particular, the availability of blood products and greater choices in antibiotics helped make cesarean delivery a safe alternative to operative vaginal deliveries. In the 1980s, information became available suggesting that some forceps deliveries (midforceps deliveries) may be associated with an increased risk of fetal morbidity, though this issue remains controversial. These factors combined to greatly reduce the appeal of forceps delivery. Currently, many obstetrical training programs in North America struggle to teach forceps delivery. Problems include the lack of adequate personnel comfortable with teaching forceps-assisted vaginal deliveries, changes in consumer attitudes, and the demand for natural delivery. In addition, many practitioners fear litigation if a forceps-assisted delivery results in a poor outcome.
Epidemiology
United States data
The frequency of operative vaginal deliveries is now estimated to be less than 5% of all vaginal deliveries. Most of these are vacuum deliveries with forceps deliveries comprising less than 1% of total deliveries. According to Bofill et al, trained fellows of the American College of Obstetricians and Gynecologists (ACOG) were more likely to be taught vacuum extraction, and they use vacuum extraction as their instrument of choice for operative vaginal deliveries. [3]
When forceps deliveries are performed, the Simpson forceps (see image below) is the instrument most commonly used for outlet- and low-forceps deliveries. Other types of forceps are also available; one specialized type is the Piper forceps, which is used in the delivery of the after-coming head in breech vaginal deliveries. It is designed to decrease traction on the fetal neck during breech delivery. Multiple other types of forceps have been designed to rotate the fetal head or for unusual maternal pelvic or fetal head shapes. For detailed information on other forceps procedures, the reader is directed to the book Dennen's Forceps Deliveries. [1]
Forceps have 4 major components, as follows (see the image below) [2] :
-
Blades - The blades grasp the fetal head, and each one is curved to fit around the head; they can be oval or elliptical and can be fenestrated (with a hole in the middle) or solid; many blades are also curved in a plane 90° from the cephalic curve to fit the maternal pelvis (pelvic curve).
-
Shanks - The shanks connect the blades to the handles and provide the length of the device; they are either parallel or crossing.
-
Lock - The lock is the articulation between the shanks; many different types have been designed.
-
Handles - The handles allow the operator to hold the device and to apply traction to the fetal head.
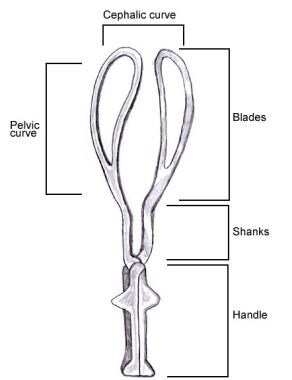 Simpson forceps, labeled to show parts of the instrument. This version has a fenestrated blade.
Simpson forceps, labeled to show parts of the instrument. This version has a fenestrated blade.
Presentation
Forceps delivery is classified according to the level and position of the head in the birth canal at the time the forceps are applied. In 1965, the ACOG issued a classification of low/outlet forceps, mid forceps, and high forceps. The low/outlet forceps categories were strictly defined and applied when the fetal scalp was visible or when the scalp had reached the pelvic floor, and only when the sagittal suture was in the anteroposterior diameter of the pelvis. In contrast, the category of mid forceps was very broad. It included many positions of the fetal head, and stations from engagement at zero station to the perineum.
When the safety of midforceps deliveries came into question in the 1980s, the ACOG redefined the classification of forceps deliveries to better define which procedures posed a significant fetal risk. [2] The revised classification uses the level of the leading bony point of the fetal head, in centimeters, measured from the level of the maternal ischial spines, to define station (-5 to 5 cm).
ACOG criteria for types of forceps deliveries
The ACOG classification of types of forceps delivery is as follows:
-
Outlet forceps: (1) The scalp is visible at the introitus, without separating the labia. The fetal skull has reached the pelvic floor. (2) The sagittal suture is in anteroposterior diameter, right or left occiput anterior or posterior position (ie, the fetal head is at or on the perineum and rotation does not exceed 45º).
-
Low forceps: The leading point of the fetal skull is at a station greater than or equal to +2 cm and is not on the pelvic floor. Low forceps deliveries without rotation are performed with a rotation of less than 45º; the procedure is described as beginning with rotation if the rotation is of more than 45º.
-
Mid forceps: The station is above +2 cm, but the head is engaged. Attempted vaginal deliveries from this station are rarely attempted and are associated with an increased rate of morbidity compared with Cesarean delivery in the second stage of labor. [4]
-
High forceps: This is not included in the classification. Previous systems classified high-forceps deliveries as procedures performed when the head is not engaged. High-forceps deliveries are not recommended.
Obstetrical pelvic evaluation (clinical pelvimetry)
The important points of interest are emphasized as follows:
-
The type (ie, gynecoid, android, anthropoid, platypoid) and adequacy of the pelvis for delivery of the fetus can be estimated clinically, with an assessment of the bony pelvis. It should be emphasized that adequate pelvic size depends not only on the pelvis but also on the size and presentation of the fetus.
-
The distance between the bottom of the symphysis pubis and the sacral promontory is measured by digital examination and is defined as the diagonal conjugate. The obstetrical conjugate, the distance from the mid symphysis to the sacral promontory, is estimated by subtracting 1.5-2 cm from the diagonal conjugate. This is used to assess the adequacy of the pelvic inlet in the anterior-posterior dimension.
-
Unfortunately, no clinical means are available to measure the mid pelvis; these measurements can only be obtained with detailed imaging studies, which themselves have not demonstrated clinical efficacy. During the examination, one may have a high index of suspicion of a contracted mid pelvis if the sacrospinous ligament is short, the sidewalls are convergent, and the concavity of the sacrum is very shallow.
-
The pelvic outlet is also important, with assessments potentially including the distance between the ischial tuberosities and the pubic angle.
-
For the purpose of assessing a patient for forceps application, one should confirm the pelvic adequacy at the time of delivery.
Indications
Indications for operative vaginal deliveries are identical for forceps and vacuum extractors. No indication for operative vaginal delivery is absolute.
The following indications apply when no contraindications exist:
-
Prolonged second stage: This includes nulliparous woman with failure to deliver after 2 hours without, and 3 hours with, conduction anesthesia. It also includes multiparous woman with failure to deliver after 1 hour without, and 2 hours with, conduction anesthesia.
-
Suspicion of immediate or potential fetal compromise in the second stage of labor.
-
Shortening of the second stage for maternal benefits: Maternal indications include, but are not limited to, exhaustion, bleeding, cardiac or pulmonary disease, and history of spontaneous pneumothorax.
-
In skilled hands, fetal malpositions, including the after-coming head in breech vaginal delivery, can be indications for forceps delivery.
Prerequisites for forceps delivery include the following:
-
The head must be engaged.
-
The cervix must be fully dilated and retracted.
-
The position of the head must be known.
-
Clinical assessment of pelvic capacity should be performed. No disproportion should be suspected between the size of the head and the size of the pelvic inlet and mid pelvis.
-
The membranes must be ruptured.
-
The patient must have adequate analgesia.
-
Adequate facilities and supportive elements should be available.
-
The operator should be competent in the use of the instruments and the recognition and management of potential complications. The operator should also know when to stop so as not to force the issue.
Relevant Anatomy
Planes and diameters of the pelvis
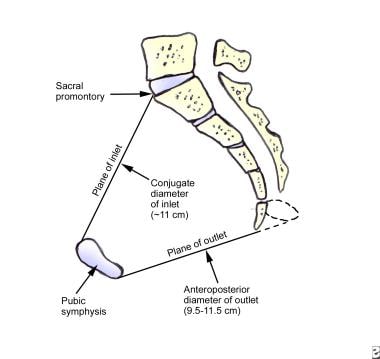
For obstetrical purposes, the pelvis is described as having 3 imaginary planes: plane of the inlet, plane of the mid pelvis, and plane of the pelvic outlet. See the images below.
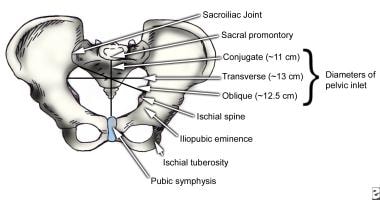
For the plane of the inlet, the following 4 diameters have been described.
-
Anteroposterior diameter: This is the distance between the sacral promontory and the symphysis pubis; it is designated the obstetrical conjugate. This conjugate normally measures approximately 10 cm or more, but it may be shortened considerably in an abnormal pelvis.
-
Transverse diameter: This is the greatest distance between the linea terminalis on either side of the pelvis. This imaginary line usually intersects the obstetrical conjugate at a point approximately 4 cm in front of the promontory.
-
Two oblique diameters: Each of these diameters extends from one of the sacroiliac joints to the iliopectineal eminence on the opposite side of the pelvis. These diameters normally average less than 13 cm each.
The plane of the mid pelvis is the plane of the smallest dimensions. This plane is extremely important following engagement of the head in obstructed labor. The interspinous diameter (usually >10 cm) is the smallest diameter of the pelvis.
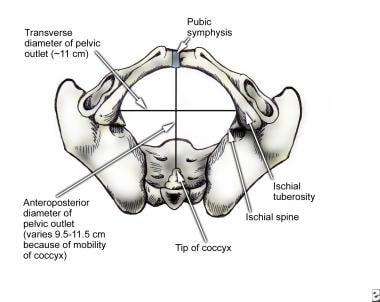
The plane of the pelvic outlet consists of 2 triangular areas created from the connection of an imaginary line between the 2 ischial tuberosities. The apex of the posterior triangle is at the tip of the sacrum, and the apex of the anterior triangle is under the pubic arch. The following 3 diameters of the outlet are of importance:
-
Anteroposterior diameter: This is normally 9.5-11.5 cm and extends from the lower margin of the symphysis pubis to the tip of the sacrum.
-
Transverse diameter: This is commonly 11 cm and is the distance between the inner edges of the ischial tuberosities.
-
Posterior sagittal diameter: This usually exceeds 7 cm and extends from the tip of the sacrum to a right-angle intersection with the line between the ischial tuberosities.
Relevant terminology
Relevant terms are listed below:
-
Engagement: This occurs when the biparietal diameter in a vertex position passes through the plane of the pelvic inlet. Thus, the widest part of the fetal head has entered the true pelvis. Engagement is generally achieved when the leading bony point of the skull has reached the level of the ischial spines (0 station).
-
Presentation: This is the description of the presenting fetal part occupying the maternal pelvic inlet (eg, cephalic, breech, shoulder).
-
Lie: This term describes the relationship between the fetal longitudinal axis and the maternal longitudinal axis (eg, longitudinal, oblique, transverse).
-
Position: This term describes the relationship of the fetal presenting part to the maternal pelvis.
-
Asynclitism: This term describes the condition when the fetal head is turned in the maternal pelvis such that one parietal bone is closer to the pelvic outlet.
Determination of position
For cephalic presentations, the reference point is the occiput, whereas in breech presentations, the reference point is the sacrum. Position is always described in reference to the maternal right or left side of the pelvis.
Determination of the position is crucial in forceps application and traction. The fontanels and sutures are used to determine the position. The finding that the fontanels are not easily palpable is not uncommon; this may occur because of distortion, molding, or caput formation.
The position can be determined by finding the location of the sagittal suture and its relationship to the posterior portion of the ear, if palpable. If the sagittal suture is in a U formation, an anterior asynclitism presentation should be suspected (ie, presentation of the anterior parietal bone of the fetal head). Conversely, if the sagittal suture is in the shape of an inverted U, this may indicate posterior asynclitism (ie, posterior parietal bone) presentation.
Most fetuses can be delivered by forceps if they are in or can be maneuvered (manually or by forceps) into an occiput anterior or posterior position.
Correct determination of the position may be the most important step prior to forceps application.
Contraindications
The following are contraindications to forceps-assisted vaginal deliveries:
-
Any contraindication to vaginal delivery (see Normal Labor and Delivery)
-
Refusal of the patient to verbally consent to the procedure
-
Cervix not fully dilated or retracted
-
Inability to determine the presentation and fetal head position
-
Inadequate pelvic size
-
Confirmed cephalopelvic disproportion
-
Unsuccessful trial of vacuum extraction (relative contraindication)
-
Absence of adequate anesthesia/analgesia
-
Inadequate facilities and support staff
-
Inexperienced operator
-
An illustration of Simpson forceps.
-
The anterior view of a pelvis.
-
The inferior view of a pelvis.
-
The sagittal section of a pelvis.
-
An illustration of a forceps delivery technique.
-
The left handle is held in the left hand (Simpson forceps).
-
The left blade is introduced into the left side of the pelvis.
-
The left blade is in place and the right blade is introduced by the right hand.
-
A median or mediolateral episiotomy may be performed at this point. A left mediolateral episiotomy is shown here.
-
The forceps have been locked. The inset shows a left occipitoanterior fetal position.
-
An illustration of horizontal traction with the operator seated.
-
An illustration of upward traction.
-
An illustration of disarticulation of the branches of the forceps; beginning modified Ritgen maneuver.
-
An illustration of Simpson forceps with a Luikart modification.
-
An illustration of Kjelland forceps with a Luikart modification.
-
Simpson forceps, labeled to show parts of the instrument. This version has a fenestrated blade.
-
An illustration of disarticulation of the branches of the forceps; beginning modified Ritgen maneuver.





