Overview
The estimation of pregnancy dates is important for the mother, who wants to know when to expect the birth of her baby, and for her health care providers, so they may choose the times at which to perform various screening tests and assessments, [1] such as serum screening, assessment of maturity, and induction of labor for postdate pregnancies.
The 3 basic methods used to help estimate gestational age (GA) are menstrual history, clinical examination, and ultrasonography. The first 2 are subject to considerable error and should only be used when ultrasonography facilities are not available. The date of feeling the first fetal movements (quickening) is far too unreliable to be useful. The date of the first documented positive pregnancy test and the beta-human chorionic gonadotropin (bHCG) level may help ascertain the minimum gestational age. In women who conceived following assisted reproduction techniques, the date of embryo transfer is known and may date the pregnancy accurately. In rare cases, the date of coitus is known, and this may be useful in calculating the length of pregnancy.
The American College of Obstetricians and Gynecologists (ACOG) recommends ultrasound measurement during the first trimester (up to and including 13 6/7 weeks of gestation) as the most accurate method to establish or confirm gestational age. If assisted reproductive technology (ART) was involved in the pregnancy, ACOG recommends that the ART-derived gestational age should be used to determine the estimated due date (EDD). According to ACOG, as soon as data from the last menstrual period (LMP), the first accurate ultrasound examination, or both are available, the gestational age and the EDD should be determined. [2]
For related information, see Medscape's Pregnancy Resource Center.
Terminology
Gestational age (GA) refers to the length of pregnancy after the first day of the last menstrual period (LMP) and is usually expressed in weeks and days. This is also known as menstrual age. Conceptional age (CA) is the true fetal age and refers to the length of pregnancy from the time of conception. This terminology does vary geographically and over time, and it may need clarification if not explicitly defined in relevant articles.
Clinical Methods of Estimating Gestational Age
Menstrual history
Gestational age (GA) has traditionally been estimated from the date of the last menstrual period (LMP). This estimation assumes that conception occurs on day 14 of the cycle. The fallacy in this assumption is that the time of ovulation varies greatly in relation to the menstrual cycle, both from cycle to cycle and individual to individual. Basing GA on the LMP tends to result in an overestimation. The 95% confidence interval of menstrual dates is -27 to +9 days. [3]
To further complicate matters, 10-45% of pregnant women cannot provide useful information about their LMP, and 18% of women with certain menstrual dates have significant differences between menstrual and ultrasonographic dating. [4] The accuracy of menstrual history in women with a history of oligo-ovulation, such as those with polycystic ovarian syndrome, should be questioned. If conception occurred while oral contraceptives or long-acting progestogens were being taken, the LMP cannot be used because it has no relation to the time of ovulation.
Date of pregnancy test
Knowing the date of the first positive pregnancy test result allows the calculation of a minimum GA. This depends on the sensitivity of the test. For example, if the test was performed 4 weeks ago and the test is known to return positive results as early as 1 week after conception, then the minimum conceptional age (CA) would be 5 weeks (GA, 5 + 2 = 7 wk of amenorrhea). This information can be useful in clinical practice if the test finding has been documented by a health care professional.
Pregnancy following assisted reproduction techniques
Not infrequently, practitioners are called upon to manage pregnancies resulting from in vitro fertilization or intrauterine insemination. The GA of pregnancies resulting from in vitro fertilization can be precisely calculated from the time of embryo replacement; however, conception may be delayed for a few days in pregnancies resulting from intrauterine insemination. In patients who have had ovulation induction, calculate GA from the day of human chorionic gonadotropin administration.
Clinical examination
The size of the uterus can be assessed by pelvic examination or by abdominal palpation. Size can be misleading in the presence of multiple pregnancy, uterine fibroids, or a full bladder. Tape measurement of the symphysis-fundus height may be useful up to 28-30 weeks' gestation, beyond which it becomes too inaccurate for dating.
Perception of fetal movement
The perception of fetal movement by the patient, often referred to as quickening, is a relatively late sign of pregnancy, usually occurring at 19-21 weeks' gestation in nulliparous women and 17-19 weeks' in multiparous women. Before the advent of pregnancy tests and ultrasonography, quickening was often the method by which a suspected pregnancy was confirmed; however, at present, it has little diagnostic value.
Estimating the Delivery Date
The expected date of delivery (EDD) is one of the earliest pieces of information a pregnant woman requests once pregnancy is confirmed. In order to calculate the EDD, the practitioner must know the median length of normal pregnancy and the last menstrual period (LMP) or ultrasonographic estimation of gestational age (GA). Pregnant women should be counselled that only 4% of all babies are born precisely on the estimated date of confinement. Failure to appreciate this may lead to unnecessary maternal anxiety if a pregnancy progresses beyond the EDD. Therefore, giving a range for the likely date of birth (eg, EDD -2 weeks to EDD +1 week) is more useful.
The median length of human pregnancy is 280 days of amenorrhea (from the first day of the LMP) or a CA of 266 days (280-14). [5] Infants born before 37 completed weeks' gestation are deemed preterm, whereas those born after 42 weeks' are considered post-term. In normal pregnancies, the length of gestation is minimally affected by maternal characteristics. However, obese women are significantly more likely to go post-term.
The Nägele rule and the obstetric wheel
In women with regular cycles and a certain LMP, the EDD is calculated by adding 7 days to the first day of the LMP and adding 9 months. [6] For example, with an LMP beginning on June 15, the EDD will be March 22 of the following year. Most antenatal clinics have obstetric wheels. These consist of an outer wheel that has markings for the calendar and an inner, sliding wheel with weeks and days of gestation. They facilitate the estimation of GA and the calculation of the EDD. The quality of these wheels varies, but in general, the larger wheels yield better results. More accurate results can be obtained by using computer software or web-based online calculators (eg, as found online at the Gestation Network).
Dates calculated on the basis of the LMP are often inaccurate because the time of ovulation can be extremely variable in relation to the occurrence of menses. Furthermore, cycle lengths among women vary greatly, as they do for individual women, changing from cycle to cycle, with a standard deviation of plus or minus 2.5 days. The tendency is toward longer anovulatory cycles, and in such women, the error in GA estimation can be much greater. [4]
Ultrasonographic Assessment of Gestational Age
The introduction of obstetric ultrasonography in the early 1970s led to a marked improvement in the evaluation of fetal and placental anatomy, as well as fetal growth. Now, it is by far the most accurate technique for estimating gestational age (GA). Most pregnant women have a first trimester scan, followed by a detailed scan for anomalies in the second trimester. According to ACOG, if an ultrasound examination that confirms or revises the EDD is not performed before 22 0/7 weeks of gestational age, the pregnancy should be considered suboptimally dated. [2]
Other documented benefits of obstetric ultrasonography include the detection of multiple pregnancies and fetal abnormalities, and the identification of placenta previa.
Ultrasonography in the first trimester
In the early first trimester, when no structures are visible within the gestational sac, GA may be estimated from the sac diameter. Several formulas can accomplish this. A common method is to measure the mean sac diameter (MSD), by calculating the mean of the 3 sac diameters. GA is then determined by consulting a table. An alternative simpler method is to add 30 to the sac size in millimeters, to give GA in days. By the time the embryo becomes visible on ultrasound the sac diameter is no longer accurate in estimating gestational age.
If cardiac activity can be detected but the embryo is not measurable, the GA is about 5.5-6.0 weeks.
GA in the first trimester is usually calculated from the fetal crown-rump length (CRL). This is the longest demonstrable length of the embryo or fetus, excluding the limbs and the yolk sac.

The correlation between CRL and GA is excellent until approximately 12 weeks' amenorrhea. No sex or race differences are appreciable, but maternal characteristics, such as age and smoking, may have a significant effect beyond 10 week' gestation. The GA estimate has a 95% confidence interval of plus or minus 6 days, and it is most accurate between 7 and 10 weeks' amenorrhea. The following formula [7] allows the estimation of GA (weeks) from the CRL (mm):
GA = –0.0007 (CRL)2 + 0.1584 (CRL) + 5.2876
Transabdominal ultrasonography may underestimate gestational age by an average of 1.6 days compared with transvaginal ultrasonography. [8]
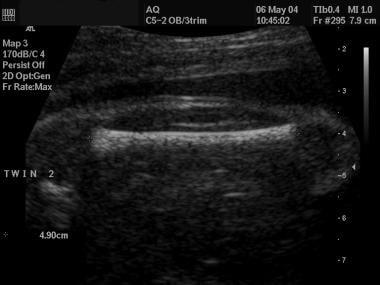
In twin pregnancies, the CRL of the smaller fetus is more accurate in determining gestational age. [9]
The biparietal diameter measured between 9 and 13 weeks’ gestation has recently been shown to be at least as accurate as the CRL, [10] with smaller random errors.
A study by Skupski et al developed a new formula to estimate gestational age from biometric data on ultrasound. The new formula was: GA = 7.85-0.127 * biparietal diameter + 0.07304 * head circumference + 0.00638 * abdominal circumference + 0.122 * femur length + 0.000685 * biparietal diameter * abdominal circumference - 0.00015 * head circumference * abdominal circumference. [11, 12]
Ultrasonography in the second trimester
Fetal biometry in the second trimester can yield acceptably accurate estimates of GA from 12 to approximately 22 weeks of amenorrhea. [7] Recent work has shown that the accuracy of ultrasonographic biometry at 12-14 weeks' gestation is at least as good as biometry performed after 14 weeks. [13, 14] The best parameters are the biparietal diameter (BPD) and the head circumference (HC), which are virtually linearly related to GA.
 Ultrasonographic image of a fetal head, with measurement of the head circumference.
Ultrasonographic image of a fetal head, with measurement of the head circumference.
The femur length (FL) can also be used and is nearly as accurate as head measurements. [15]
Racial differences in FL are significant, but differences in HC are not. GA estimates by the BPD or HC have a 95% confidence interval of plus or minus 8 days. The following formula [16] allows estimation of GA (days) from the BPD (mm):
GA = 39.1 + 2.1 (BPD)
Combinations of multiple variables to date a pregnancy have also been described; however, the improvement in accuracy from these algorithms is clinically negligible.
Ultrasonography in the third trimester
Fetal biometry in the third trimester is subject to much greater individual size variations than in the second trimester. Its accuracy for GA assignment is reduced considerably, and estimates may have confidence intervals of plus or minus 3 weeks. [17] More recent work with pregnancies resulting from in vitro fertilization suggests that third trimester scans are considerably more accurate than previously thought, with random errors (1 SD) of 8-9 days. This is equivalent to confidence intervals of about plus or minus 2 weeks. [18]
The table below illustrates the 95% confidence limits for GA estimated from the BPD in the third trimester.
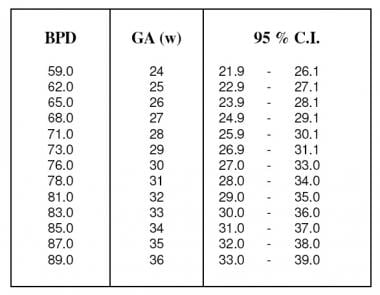 Estimate of gestational age (weeks) from the biparietal diameter in the third trimester with 95% confidence intervals. Adapted from Hadlock et al (1984).
Estimate of gestational age (weeks) from the biparietal diameter in the third trimester with 95% confidence intervals. Adapted from Hadlock et al (1984).
Confirmation of fetal maturity may also be obtained by examining the ossification centers. [19] The distal femoral epiphysis appears at a mean age of 32-33 weeks' gestation, but may be seen as early as 29 weeks' gestation [20] ; its size increases linearly with gestational age. A distal femoral epiphysis diameter greater than 7 mm indicates a gestational age greater than 37 weeks. Visualization of the proximal tibial epiphysis indicates a gestational age of at least 35 weeks. The sonographic detection of the proximal humeral epiphysis has been correlated with a mature amniocentesis lung profile.
Combining Menstrual and Ultrasonographic Dates
In many ultrasound departments, a common practice is to combine the last menstrual period (LMP) with ultrasonographic dates in what is known as the 10-day rule or 7-day rule. For example, with the 10-day rule, if LMP dates and ultrasonographic dates are in agreement within 10 days, LMP dates are accepted. On the other hand, if the discrepancy exceeds 10 days, ultrasonographic dates are used. The rationale for using these rules is to exclude large errors from incorrect menstrual dates. The implicit assumption of this method is that menstrual dating is preferable to ultrasonographic dating. Detailed analysis from large databases has not shown any advantage in using these rules. [21] Unless the fetus is thought to be anatomically abnormal, ultrasonographic dates may be used for all pregnancies if a scan is available in the first half of pregnancy. However, combining menstrual dates with ultrasonographic dates is still widely practiced in the United States and in Australia.
According to the National Institute for Health and Clinical Excellence (NICE) guidelines on antenatal care, [22] the CRL should be used to determine gestational age. If the CRL is greater than 84 mm, the HC should be used instead. [22]
Gestational age calculators
Computer software is now available for accurate determination of GA from either ultrasonographic biometry or menstrual dates, and results are more accurate than those obtained with obstetric wheels. Such software is accessible online through the Gestation Network and can be downloaded free of charge (see Gestation Network, Gestational Age Calculator).
Clinical significance of discrepancy between menstrual and ultrasonographic dates
A discrepancy more than 7 days between menstrual and ultrasound dates is noted in 25% of women, and is more common in cases with a BMI >30, in whom the estimated due date is often postponed. [23] In a large trial on ultrasonography, the risk of cesarean section increased from 10% when the ultrasonographic-based GA exceeded the LMP-based estimate by 4 days to 60% when the discrepancy increased to 21 days in nulliparous women. Also, for each day the ultrasonographic-based estimate exceeded the LMP-based estimate, birth weight was higher by 9.6 g. [24] A discrepancy of greater than +7 days can also arise from a prolonged interval between last menstruation and conception. These women, especially multiparae, are at an increased risk of preterm labor, with an OR of 1.9. [25] A smaller than expected CRL in the first trimester may rarely be due to chromosomal anomalies.
-
Ultrasonographic view of a fetus for a crown-rump measurement.
-
Ultrasonographic image of a fetal head, with measurement of the head circumference.
-
Ultrasonographic view of a fetal femur.
-
Estimate of gestational age (weeks) from the biparietal diameter in the third trimester with 95% confidence intervals. Adapted from Hadlock et al (1984).







